A 63‑year‑old man after cadaveric kidney transplantation performed 23 years ago was admitted to the hospital due to a sudden and severe deterioration of kidney function (an increase in creatinine level from 2.45 mg/dl to 7.06 mg/dl with the corresponding estimated glomerular filtration rate of 8 ml/min) with uremic symptoms, hyperkalemia, volume overload, and refractory hypertension (180/90 mm Hg). He had a history of transplant renal artery stenosis (TRAS) and double‑angioplasty and stenting procedure 2 and 22 years after transplantation. Cyclosporine was discontinued and therapy of hypertension was modified; however, only slight improvement in laboratory parameters and blood pressure control was achieved. Reinitiation of dialysis therapy was considered, assuming that there was end‑stage renal failure.
The ultrasound showed normal size and structure of the transplanted kidney with a length of 110 mm, parenchymal layer of 13 to 17 mm, and normal echogenicity without impairment of the urine outflow (Figure 1A and 1B). Doppler ultrasound revealed hemodynamically significant stenosis localized in the mid‑proximal part of the graft artery, most likely in the stent, with an increase in systolic peak velocity up to 416 cm/s (Figure 1C), reduced resistive indexes at parenchymal level to 0.53, and extended acceleration time to 0.09 s (Figure 1D).
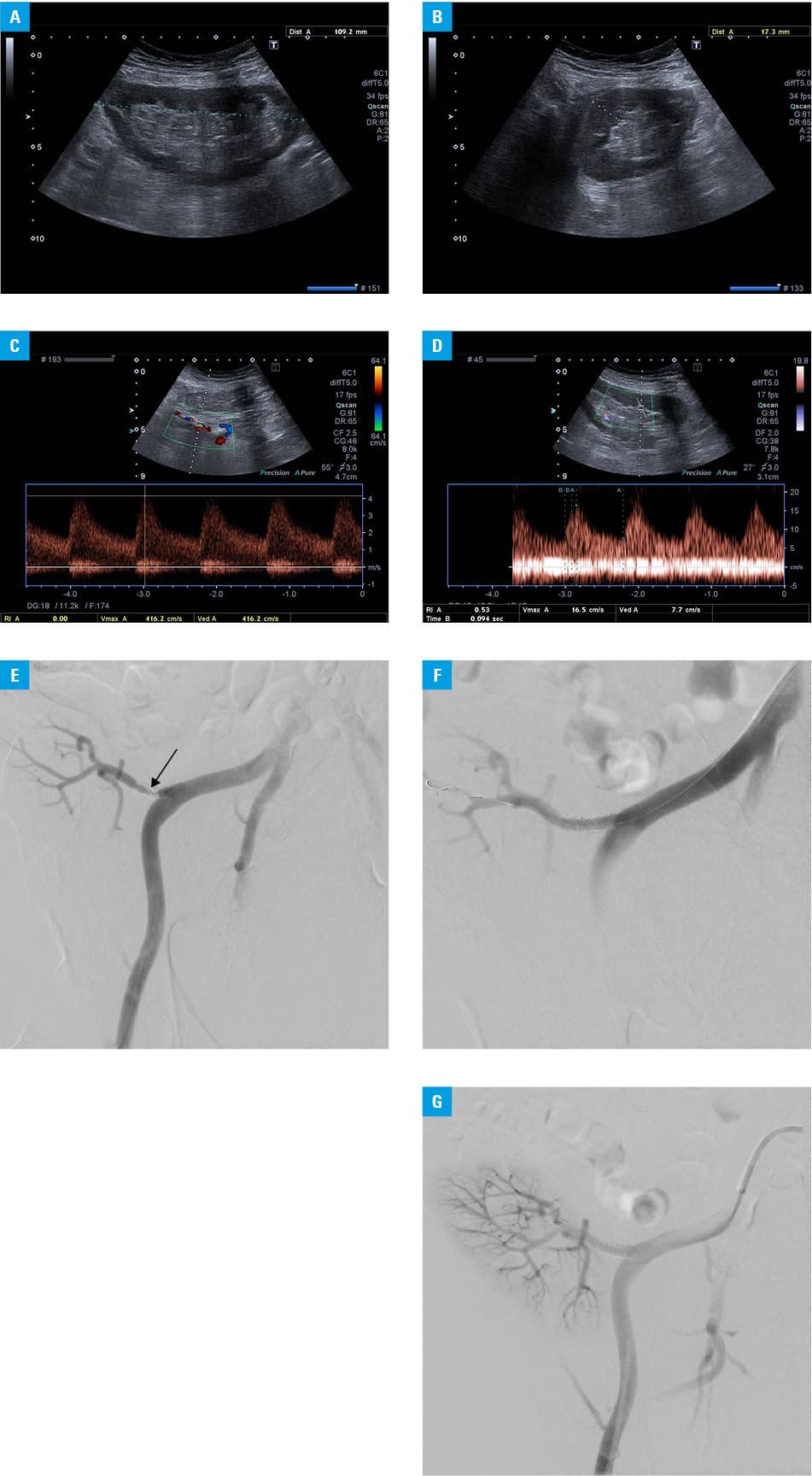
Despite advanced graft failure but with normal echogenicity on ultrasound, a decision on angioplasty was made.
Arteriography confirmed the presence of in‑stent restenosis implanted into the proximal segment of the renal artery (Figure 1E). The angioplasty of restenosis using a 5‑mm diameter balloon and an IN.PACT Pacific (drug coated) 5 × 40 mm balloon (Medtronic, Minneapolis, Minnesota, United States) was performed with no residual stenosis after revascularization (Figure 1F and 1G). In a few days after angioplasty the recovery of graft function was achieved to stable values observed in recent years (serum creatinine, 2.0 mg/dl). Moreover, blood pressure decreased, allowing for reduction of the daily doses of antihypertensive drugs (130/80 mm Hg).
TRAS represents approximately 75% of vascular complications after kidney transplantation, with the incidence rates ranging from 6% to 23%, depending on the diagnostic criteria and study population. TRAS mainly occurs from 3 months to 2 years after transplantation, but it can present at any time, leading to deterioration of function or even graft loss.1
Doppler ultrasonography is used as initial imaging modality, and systolic peak velocity of more than 2.5 m/s is the best discriminating index for TRAS.2,3 Interventional treatment of choice is percutaneous transluminal angioplasty with or without stenting.2,3 Restenosis that develops within the first 6 to 9 months after primary intervention is the main complication of percutaneous transluminal angioplasty, with incidence ranging from 15% to 28% and increasing risk with second stenting.3
The mechanism of in‑stent restenosis in the transplanted renal arteries is intimal hyperplasia, thus the use of paclitaxel‑coated balloon that inhibits arterial smooth muscle proliferation, migration, and extracellular matrix formation may be favorable in treating restenosis and potentially decreasing the incidence of late thrombosis without antiplatelet therapy.4
The presented case shows that even many years after transplantation it is worth searching for the causes of severe and sudden deterioration of allograft function, attempt treatment, and give the patient a chance to celebrate further anniversaries in life with a transplanted kidney.
- Hurst FP, Abbott KC, Neff RT, et al. Incidence, predictors and outcomes of transplant renal artery stenosis after kidney transplantation: analysis of USRDS. Am J Nephrol. 2009; 30: 459‑467. | Crossref
- Wang L, Liu B, Yan J, et al. Interventional therapy for transplant renal artery stenosis is safe and effective in preserving allograft function and improving hypertension. Vasc Endovascular Surg. 2017; 51: 4‑11. | Crossref
- Ngo AT, Markar SR, De Lijster MS, et al. A systematic review of outcomes following percutaneous transluminal angioplasty and stenting in the treatment of transplant renal artery stenosis. Cardiovasc Intervent Radiol. 2015; 38: 1573‑1588. | Crossref
- Li CM, Shang T, Tian L, Zhang HK. Short‑term outcomes using a drug‑coated balloon for transplant renal artery stenosis. Ann Transplant. 2018; 23: 75‑80. | Crossref
ARTICLE INFORMATION