…if my explanation of these classes of facts be at all right, whole classes of organic beings must be included in one line of descent. (Charles Darwin, letters to Leonard Jenynes, January 7, 1860)
The work of Charles Darwin is synonymous with the development of the taxonomy of all living beings, which has given understanding and order to the chaos and beauty of the natural world.
In this issue of Polish Archives of Internal Medicine (Pol Arch Intern Med), Podolec et al1 present an updated version of their previously published classification of “rare arrhythmogenic and conduction disorders, and rare arrhythmias.” The update was undertaken with the admirable aim of planning clinical studies and improving the standards of care of patients with rare arrhythmic conditions. Using a predefined prevalence of less than 5 per 10000 individuals, rare “primary electrical disorders of the heart” were subdivided into those predisposing to bradyarrhythmia, supraventricular tachyarrhythmias, and ventricular tachyarrhythmias. It is the latter group that has potentially the most significant clinical impact since these conditions carry a risk of sudden cardiac death, often in young and otherwise healthy individuals. In fact, a number of these conditions will only be diagnosed following an episode of ventricular fibrillation (VF).1
Sudden cardiac arrest is common with an estimated 300000 cases per year in Europe.2 The large majority of individuals sadly do not survive to hospital admission, let alone to discharge. In the context of ischemic and structural heart disease, VF accounts for the large majority of cases. However, in some cardiac arrest survivors, the initial investigations comprising 12‑lead electrocardiogram (ECG), coronary angiogram, and transthoracic echocardiogram, will not reveal a specific diagnosis. In a recent cohort study of out‑of‑hospital cardiac arrests in Paris, 12.3% of individuals3 who survived to undergo investigation fell into this group of “unexplained cardiac arrest” (UCA). Therefore, UCA could be considered a rare arrhythmogenic disease worthy of separate classification (Figure 1).
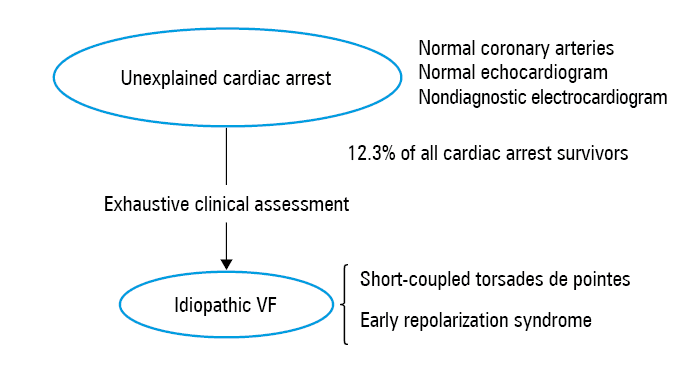
Work from the CASPER registry (Cardiac Arrest Survivors with Preserved Ejection Fraction Registry) has shown that an in‑depth clinical examination of such UCA cases will reveal a specific diagnosis in approximately 40% of patients,4 either at the time of assessment or during subsequent follow‑up. Genetic testing in UCA survivors will also identify pathogenic variants in genes associated with established cardiac disease in 17% of patients.5 A significant proportion of the diagnoses will include the primary electrical disorders predisposing to ventricular arrhythmias listed in the current classification (VI‑1B 1–6).1 However, whether a patient’s diagnosis evolves from UCA to a more specific condition can depend on the depth of clinical evaluation. For this reason, it is important to differentiate UCA from idiopathic VF, as described below, where it is assumed that exhaustive clinical assessment has been carried out. In addition, several disorders listed in the classification can be considered to significantly overlap with one another.
Of those conditions included in the classification, Brugada syndrome (BrS) and long QT syndrome (LQTS) are most commonly diagnosed following UCA4 and have the most well‑established and accepted diagnostic criteria.6 These diagnoses may not be made, however, if appropriate provocation tests (ajmaline provocation for BrS and exercise ECG for LQTS) are not performed. Other conditions listed include early repolarization syndrome, short‑coupled torsades de pointes, and idiopathic VF. They are rarer, have less well‑established diagnostic criteria, and may be considered as very similar and overlapping conditions.
Early repolarization (ER) syndrome (ERS) is classified by the authors as a channelopathy. However, the underlying pathophysiology remains incompletely described, with contrasting evidence for depolarization and repolarization abnormalities described,7 echoing previous debates in BrS. Furthermore, there is no convincing evidence for the involvement of specific ion channels as there is in BrS and LQTS. The diagnosis of ERS is based on the presence of inferolateral J‑point elevation of 0.1 mV or higher in the context of any otherwise unexplained cardiac arrest.6 The diagnosis came about following the recognition that the ER pattern was overrepresented in patients with idiopathic VF compared with controls8 and that individuals with the ER pattern were at higher lifetime risk of arrhythmic death.9 However, the ECG pattern can be highly variable in any individual, depending on a wide variety of factors including heart rate, vagal tone, and levels of physical training. Therefore, its absence on a single ECG cannot exclude a dynamic substrate which may have contributed to an episode of VF. Conversely, the ER pattern is common, particularly in young males, and so identifying it in an otherwise unexplained cardiac arrest survivor may not be indicative of a causal association. Therefore, it may be misleading to classify ERS as a ion channel disease, and it may be more accurate to consider the ER pattern as a risk factor for arrhythmia, modifying the so‑far incompletely described substrate for “idiopathic VF.”
Short‑coupled torsades de pointes is also considered a separate rare cause of cardiac arrest. Premature ventricular contractions (PVCs) occur very soon after the preceding QRS (coupling interval <300 ms) and directly initiate torsades de pointes, which may then progress to VF. The diagnosis relies on the observation of the initiating PVC. Therefore, it is usually only made after the initial episode, either in the context of a “VF storm” where recurrent episodes are observed in the hospital or after a remote event documented on an implantable cardioverter‑defibrillator electrogram. Therefore, in UCA without recurrence, it is not possible to exclude the diagnosis of short‑coupled torsades de pointes. If frequent PVCs are seen, the initiating PVC can be mapped and ablated with a reduction in the risk of future events. Mapping consistently demonstrates that these PVCs originate from within the His‑Purkinje conducting system.10 It is likely that many cases of apparently idiopathic VF are initiated by this mechanism.
In 2013, Priori et al11 stated that idiopathic VF is diagnosed: “in a resuscitated cardiac arrest victim … in whom known cardiac respiratory, metabolic and toxicological aetiologies have been excluded through clinical evaluation”.11 By the 2015 European Society of Cardiology guideline on the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death, this had evolved to the simple statement that idiopathic VF “is a diagnosis by exclusion but may change in the future due to improved diagnostics.”6 No consensus was offered on the minimum clinical evaluation that should be undertaken before the label of idiopathic VF is used.
Investigation of a cardiac arrest survivor can be considered in a tiered approach, with the first tier of investigations including those routinely undertaken and with the highest diagnostic yield: 12‑lead ECG, coronary imaging, and transthoracic echocardiogram. In UCA, the second tier of investigations should be undertaken, including additional ECGs (high right ventricular leads, signal‑averaged ECGs), additional cardiac imaging (usually with magnetic resonance imaging), exercise testing, and ajmaline provocation test. This would be considered the minimum investigation before making a diagnosis of idiopathic VF. The third tier of discretionary tests can include additional provocation tests, electrophysiology studies, cardiac biopsy, and genetic testing.
While taxonomies and disease classification systems undoubtedly help understand otherwise complex systems and how they relate to one another, it is important to allow room within them for a diagnosis to evolve from one state to another. With appropriate evaluation, an UCA may evolve into a specific diagnosis, as classified by Podolec et al,1 a number of which may show significant overlap between one another.
- Podolec P, Baranchuk A, Brugada J, et al. Clinical classification of rare cardiac arrhythmogenic and conduction disorders, and rare arrhythmias. Pol Arch Intern Med. 2019; 129: 154‑159. | Crossref
- Townsend N, Nichols M, Scarborough P, Rayner M. Cardiovascular disease in Europe ‑ epidemiological update 2015. Eur Heart J. 2015; 36: 2696‑2705. | Crossref
- Waldmann V, Bougouin W, Karam N, et al. Characteristics and clinical assessment of unexplained sudden cardiac arrest in the real‑world setting: focus on idiopathic ventricular fibrillation. Eur Heart J. 2018; 39: 1981‑1987. | Crossref
- Herman ARM, Cheung CC, Gerull B, et al. Outcome of apparently unexplained cardiac arrest: results from investigation and follow‑up of the Prospective Cardiac Arrest Survivors With Preserved Ejection Fraction Registry. Circ Arrhythm Electrophysiol. 2016; 9: e003619.
- Mellor G, Laksman ZW, Tadros R, et al. Genetic testing in the evaluation of unexplained cardiac arrest: from the CASPER (Cardiac Arrest Survivors with Preserved Ejection Fraction Registry). Circ Cardiovasc Genet. 2017; 10: 10e001686.
ARTICLE INFORMATION