Adrenocortical carcinoma associated with giant bilateral myelolipomas in classic congenital adrenal hyperplasia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Adrenocortical carcinoma associated with giant bilateral myelolipomas in classic congenital adrenal hyperplasia
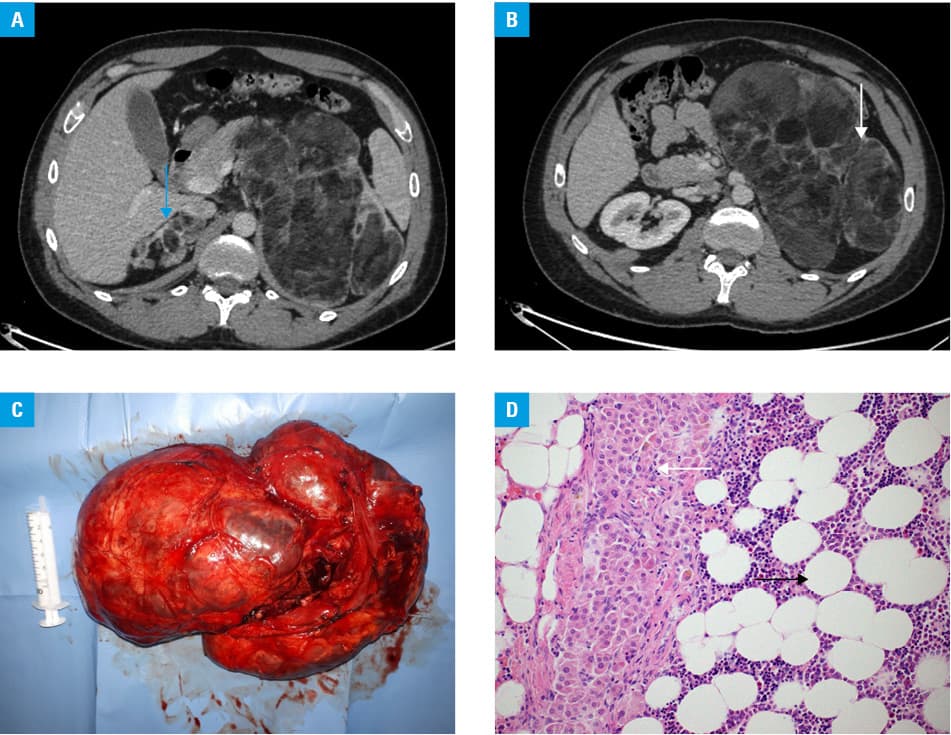
A 32‑year‑old male patient, diagnosed with a classic form of congenital adrenal hyperplasia (CAH) due to 21α-hydroxylase deficiency as a neonate was referred to the Department of Endocrinology in March 2018 because of poor disease control and rapidly enlarging bilateral adrenal masses (Figure 1A and 1B). A year and a half before the admission, an adrenal biopsy was performed (in another hospital), which revealed a benign tumor, myelolipoma. However, due to the mass effect and heterogenic appearance on imaging, the left side tumor was surgically removed 2 years after its initial presentation. Macroscopic examination revealed a mass of 350 mm in the longest dimension and almost 2 kg of weight (Figure 1C). Microscopically, the tumor was composed mainly of myelolipoma tissue, with adrenocortical cell “islands.” However, when assessed using the Weiss score, these foci were diagnosed not as an adrenocortical adenoma but adrenocortical carcinoma (ACC). From among 9 histologic criteria of malignancy, 6 were positive (with 3 necessary to diagnose ACC), including nuclear grade (Fuhrman’s III), atypical mitotic figures, 10% of clear cells, diffuse architecture, and sinusoidal and capsular invasion (Figure 1D). Therefore, chemotherapy with mitotane was introduced due to a large size of the tumor, previous biopsy, and testicular adrenal rest tumors. The patient currently adheres to rigorous hormonal treatment and monitoring regimen, and is awaiting right‑sided adrenalectomy.
Myelolipomas are uncommon, benign, and nonfunctioning adrenal masses, composed of mature adipose tissue and hemopoietic elements. They usually require surgical excision only when becoming large and symptomatic.1 However, in very rare cases, collision tumors of 2 or more histologically distinct compounds are encountered, such as myelolipoma coexisting with adrenocortical adenoma or carcinoma.2 An increased prevalence of adrenal tumors has been reported in patients with CAH and poor compliance, due to chronic adrenocorticotropic hormone (ACTH) stimulation, which acts as a growth and metaplasia‑inducing factor. However, fewer than 20 cases of giant bilateral myelolipomas in CAH patients have been reported to date, and the role of ACTH or other hormones in their development is still uncertain.3
The presented case highlights the need for proper and careful management of patients with CAH. However, it also shows that the risk of malignancy exists even in tumors considered as benign. Adrenocortical carcinoma is a rare neoplasm with low survival rates.4 Histopathologic diagnosis based on multiparameter scoring systems is often challenging. In general, adrenal tumors should preferably be excised and examined as a whole, thus indications for biopsy are very limited and only to cases in which the diagnosis would change the course of treatment. In our patient, the biopsy was completely misguided. What is more, the suspicion of ACC constitutes a strong contraindication to biopsy due to the possibility of neoplastic cell spread in the needle conduit. Therefore, mitotane treatment was introduced because this type of additional treatment may be associated with better outcome.4 Mitotane has a direct and selective cytotoxic effect on adrenal cortex cells, thereby inducing permanent atrophy of any normal or malignant adrenal tissue that is left after the operation. However, also in patients with CAH who are not candidates for surgery, it may play a role in restoring fertility impaired by testicular adrenal rest tumors.5
- Ioannidis O, Papaemmanouil S, Chatzopoulos S, et al. Giant bilateral symptomatic adrenal myelolipomas associated with congenital adrenal hyperplasia. Pathol Oncol Res. 2011; 17: 775‑778. | Crossref
- Sun X, Ayala A, Castro CY. Adrenocortical carcinoma with concomitant myelolipoma in a patient with hyperaldosteronism. Arch Pathol Lab Med. 2005; 129: 144‑147.
- Almeida MQ, Kaupert LC, Brito LP, et al. Increased expression of ACTH (MC2R) and androgen (AR) receptors in giant bilateral myelolipomas from patients with congenital adrenal hyperplasia. BMC Endocr Disord. 2014; 14: 42. | Crossref
- Nowak KM, Samsel R, Cichocki A, et al. Prognostic factors in adrenocortical carcinoma: data from a large Polish series. Pol Arch Intern Med. 2018; 128: 371‑378. | Crossref
- Bry‑Gauillard H, Cartes A, Young J. Mitotane for 21‑hydroxylase deficiency in an infertile man. N Engl J Med. 2014; 371: 2042‑2044. | Crossref
ARTICLE INFORMATION