Management strategies and 5-year outcomes in Polish patients with stable coronary artery disease versus other European countries: data from the CLARIFY registry
Key words: CLARIFY registry, geographical differences, management, outcome, stable coronary artery disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Management strategies and 5-year outcomes in Polish patients with stable coronary artery disease versus other European countries: data from the CLARIFY registry
Introduction: An international registry of ambulatory patients with stable coronary artery disease (CLARIFY) allows a comparison of management and outcomes in real‑life setting.
Objectives: We aimed to compare the management strategies and 5‑year outcomes in patients from Poland and from other European countries.
Patients and methods: Stable coronary artery disease was defined as previous myocardial infarction (MI) or revascularization, coronary stenosis greater than 50%, or documented symptomatic myocardial ischemia. Patients were followed on an annual basis for 5 years.
Results: Among the total of 32703 patients, 1000 were enrolled in Poland, and 17326 in other European countries. Polish patients were younger, with a higher proportion of women, smokers, and patients with previous MI, dyslipidemia, and hypertension. Patients in both cohorts received adequate medical treatment, with more Polish patients receiving β-blockers. Blood pressure and lipid control to target was similar and remained low in both cohorts. Diabetes control and successful smoking cessation rates were lower in Poland than in other European countries. Polish patients more often underwent percutaneous coronary intervention. All‑cause (8.5% vs 7.9%; P = 0.81) and cardiovascular death rates (5.3% vs 4.9%; P = 0.82) did not differ between the groups, but fatal or nonfatal MI occurred more often in the Polish cohort (5% vs 3.1%; P = 0.006). Angina control was better in Poland than in other European countries (Canadian Cardiovascular Society class II‑IV, 11.5% vs 15.8% of patients; P <0.001).
Conclusions: Risk factor control was insufficient both in patients from Poland and in those from other European countries. The more frequent use of revascularization in Polish patients was not linked to improved outcomes, but, together with more extensive prescription of β-blockers, might have contributed to better angina control.
Introduction
Stable coronary artery disease (SCAD) is a growing global medical and social problem1 due to population aging and increasing survival of patients with acute coronary syndromes. The risk of major adverse cardiovascular events in patients with SCAD depends on various factors, such as age, risk factor control, left ventricular function, kidney dysfunction, presence of angina, or the model of patient care.2-5 Treatment strategies may differ between regions and countries and may affect clinical outcomes.6
In addition, over the last decades, the clinical profile of patients with SCAD has considerably evolved.7 The CLARIFY registry (Prospective Observational Longitudinal Registry of Patients with Stable Coronary Artery Disease) was an international registry of ambulatory patients, which aimed to describe the contemporary population of patients with SCAD, identify gaps between evidence‑based recommendations and actual treatment, and establish determinants of outcome.8,9 The aim of the current analysis was to compare management strategies and long‑term clinical outcomes between patients from Poland and other European countries.
Patients and Methods
Study design
The rationale, design, and baseline characteristics of the entire CLARIFY population have been published elsewhere.9 CLARIFY participants were enrolled from 45 countries worldwide between November 2009 and June 2010. In order to be eligible for the study, the patients had to fulfill at least one of the following criteria: previous myocardial infarction (MI), history of myocardial revascularization (coronary artery bypass surgery or percutaneous coronary intervention [PCI]), coronary stenosis greater than 50%, or documented symptomatic myocardial ischemia. The main exclusion criteria were hospitalization for cardiovascular disease within the previous 3 months, planned revascularization, and serious conditions that might affect the 5‑year outcome.
In each country, study sites were selected by national coordinators according to predefined criteria that aimed to reflect the burden of SCAD. Participating physicians were asked to manage patients according to their usual practice. Each physician was requested to enroll 10 to 15 consecutive patients. In each country, the goal was to recruit approximately 25 patients per million inhabitants. Patients were followed on an annual basis for 5 years. Data were collected using standardized electronic case‑report forms available in a local language. The data were centrally verified for accuracy and completeness. Five percent of centers were randomly selected for complete on‑site audit.9
The CLARIFY registry was conducted according to the principles specified in the Declaration of Helsinki. The study was approved by the Ethics Committees and regulatory agencies according to national and local legal requirements. All participants gave a written informed consent before entering the study. CLARIFY is registered in the ISRCTN registry of clinical trials (IRSCTN43070564).
Clinical outcomes
In the current analysis, we compared management strategies and 5‑year outcomes between patients recruited in Poland and in the European cohort excluding Poland. We compared the patterns of drug treatment and revascularization procedures, analyzed the efficacy of risk factor control, and assessed clinical outcomes at 5 years, including the first occurrence of cardiovascular death or nonfatal MI, cardiovascular death, nonfatal MI or nonfatal stroke, as well as all‑cause and cardiovascular death and MI (fatal or nonfatal). We also assessed changes in the prevalence of angina at baseline and at 5‑year follow‑up in both groups.
Statistical analysis
Statistical analysis of data was performed by an independent statistics center (Robertson Centre for Biostatistics, University of Glasgow, United Kingdom). Continuous variables were presented as mean (SD) or median and interquartile range, depending on data distribution. Categorical data were presented as number and percentage. Clinical outcomes were analyzed with unadjusted Cox proportional hazards regression models in the R software, version 3.4.1 (The R Project for Statistical Computing).10,11 Ancillary analyses were performed locally by an investigator not involved in the study, using the summary independent t test for continuous data, and the χ2 test for categorical data.
Results
Patient characteristics
Among the total of 32703 patients, exactly 1000 were enrolled in Poland, and 17326 in 23 European countries included in the study. The list of participating European countries and respective number of patients recruited are presented in Supplementary material, Table S1. Baseline patient characteristics are given in Table 1. Polish patients were younger, with a higher proportion of women, current or former smokers, and patients with a history of MI, dyslipidemia, and hypertension. At baseline, a similar proportion of patients in both cohorts had Canadian Cardiovascular Society (CCS) class II to IV angina (Polish patients, 20.3% vs patients from other European countries, 20.7%).
Parameter | Poland (n = 1000) | Other European countries (n = 17326) | P value | |
Abbreviations: BMI, body mass index; BP, blood pressure; CABG, coronary artery bypass grafting; COPD, chronic obstructive pulmonary disease; HF, heart failure; HR, heart rate; MI, myocardial infarction; PAD, peripheral artery disease; PCI, percutaneous coronary intervention | ||||
Age, y, mean (SD) | 62.1 (9.0) | 64.4 (10.4) | <0.001 | |
Male sex, n (%) | 729 (72.9) | 13 628 (78.7) | <0.001 | |
Systolic BP, mm Hg, mean (SD) | 132.7 (15.4) | 132.3 (16.3) | 0.45 | |
Diastolic BP, mm Hg, mean (SD) | 79.6 (9.5) | 78.4 (9.7) | <0.001 | |
HR by palpation, bpm, mean (SD) | 69.3 (9.4) | 67.2 (10.5) | <0.001 | |
Weight, kg, mean (SD) | 83.2 (13.7) | 82.0 (14.1) | 0.009 | |
BMI, kg/m2, mean (SD) | 28.8 (4.3) | 28.3 (4.2) | <0.001 | |
Medical history, n (%) | ||||
Previous MI | 668 (66.8) | 10 601 (61.2) | <0.001 | |
Previous PCI | 606 (60.6) | 10 056 (58.0) | <0.001 | |
Previous CABG | 258 (25.8) | 4 339 (25.0) | 0.60 | |
Previous stroke | 32 (3.2) | 675 (3.9) | 0.31 | |
Previous HF hospitalization | 43 (4.3) | 897 (5.2) | 0.24 | |
Asthma or COPD | 58 (5.8) | 1 410 (8.1) | 0.01 | |
PAD | 109 (10.9) | 2 238 (12.9) | 0.07 | |
Risk factors, n (%) | ||||
Dyslipidemia | 845 (85.4) | 13 910 (80.3) | <0.001 | |
Treated hypertension | 789 (78.9) | 12 702 (73.3) | <0.001 | |
Diabetes | 279 (27.9) | 4 530 (26.2) | 0.22 | |
Smoking status | Current | 132 (13.2) | 2 183 (12.6) | <0.001 |
Former | 559 (55.9) | 8 228 (47.5) | ||
Never | 309 (30.9) | 6 914 (39.9) | ||
Provision of care, n (%) | ||||
Cardiologist | 627 (62.7) | 16 207 (93.8) | <0.001 | |
Noncardiologist | 373 (37.3) | 1070 (6.2) | ||
Medical therapy
Medical therapies used at baseline and at the end of study are shown in Table 2. In general, most patients in both cohorts received guideline‑recommended medical treatment throughout the study.12 Over 90% of patients received antiplatelet treatment with either aspirin or other agent (mostly clopidogrel). Similarly, over 90% of patients received a lipid‑lowering drug (predominantly a statin). Angiotensin‑converting enzyme inhibitors (ACEIs) and β-blockers were more frequently used in the Polish cohort, while the use of angiotensin receptor blockers and ivabradine was more frequent in the European cohort.
Drug class | Baseline | At 5 yearsa | ||
Poland (n = 1000) | Other European countries (n = 17326) | Poland (n = 866) | Other European countries (n = 11374) | |
Data are presented as number (percentage) of patients.
a Percentages provided for patients with no missing data
b Percentage of patients receiving lipid‑lowering drugs
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker | ||||
Aspirin | 952 (95.2) | 14878 (85.9) | 766 (88.5) | 8489 (80.2) |
Other antiplatelet drug | 197 (19.7) | 5 850 (33.8) | 157 (18.1) | 2616 (24.7) |
Dual antiplatelet therapy | 168 (16.8) | 4 158 (24.0) | 129 (14.9) | 1760 (16.6) |
Lipid‑lowering drugs | 958 (95.8) | 16 008 (92.4) | 815 (94.1) | 9537 (90.0) |
Statinsb | 883 (92.2) | 14 314 (89.4) | 731 (89.7) | 8373 (87.8) |
β-Blockers | 903 (90.3) | 13 508 (78.0) | 764 (88.2) | 8006 (75.6) |
Calcium antagonists | 268 (26.8) | 4 547 (26.3) | 262 (30.3) | 2970 (28.0) |
Ivabradine | 41 (4.1) | 2836 (16.4) | 70 (8.1) | 2641 (24.9) |
ACEIs | 752 (75.2) | 9 619 (55.5) | 611 (70.6) | 5600 (52.9) |
ARBs | 175 (17.5) | 4 374 (25.3) | 169 (19.5) | 2860 (27.0) |
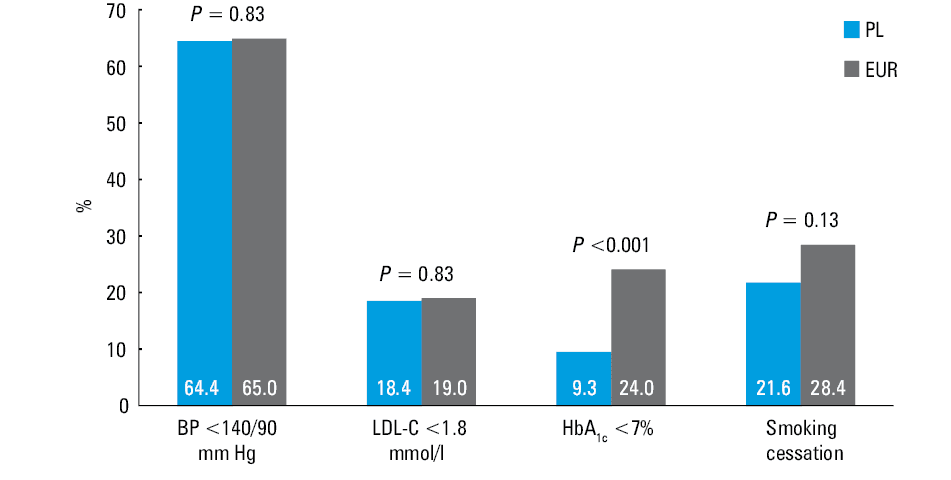
In patients with different risk factors at baseline, target values for blood pressure were achieved in similar, small number of patients (Polish cohort, 64.4% vs European cohort, 65% of hypertensive patients with blood pressure <140/90 mm Hg at 5 years; P = 0.83), similarly to lipid control (Polish cohort, 18.4% vs European cohort, 19% of patients with dyslipidemia and low‑density lipoprotein [LDL] cholesterol levels <1.8 mmol/l [<70 mg/dl] at 5 years; P = 0.83). Diabetes control (glycated hemoglobin A1c <7%) was worse in the Polish cohort (9.3% vs 20.4% in the European cohort; P <0.001). The success rate for smoking cessation was also worse in Poland than in other European countries (21.6% vs 28.4%, respectively; P = 0.13) (Figure 1).
Revascularization
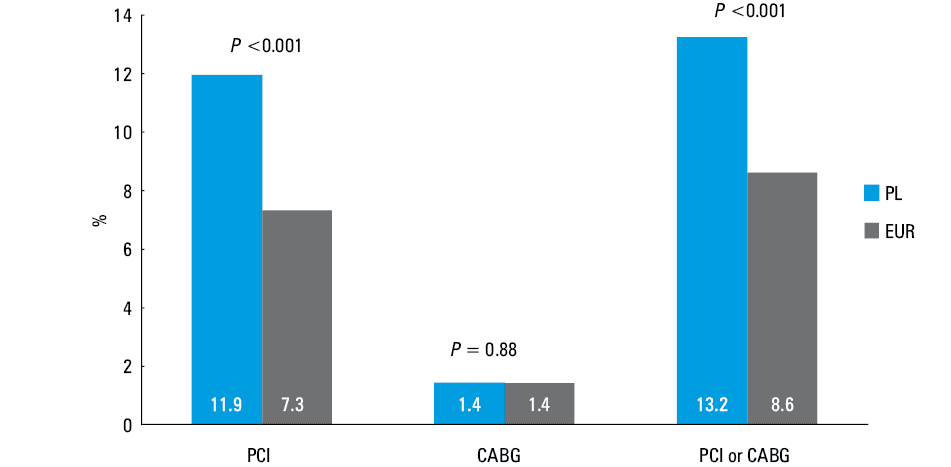
Incident revascularization rates are shown in Figure 2. Revascularization was more frequent in the Polish cohort than in the European cohort (13.2% vs 8.6%, respectively; P <0.001). The difference in myocardial revascularization rates resulted from a more frequent use of PCI in the Polish cohort (11.9% vs 7.3%, respectively; P <0.001), while the use of coronary artery bypass surgery was equally low in both groups (1.4% vs 1.4%, respectively; P = 0.88).
Clinical outcomes
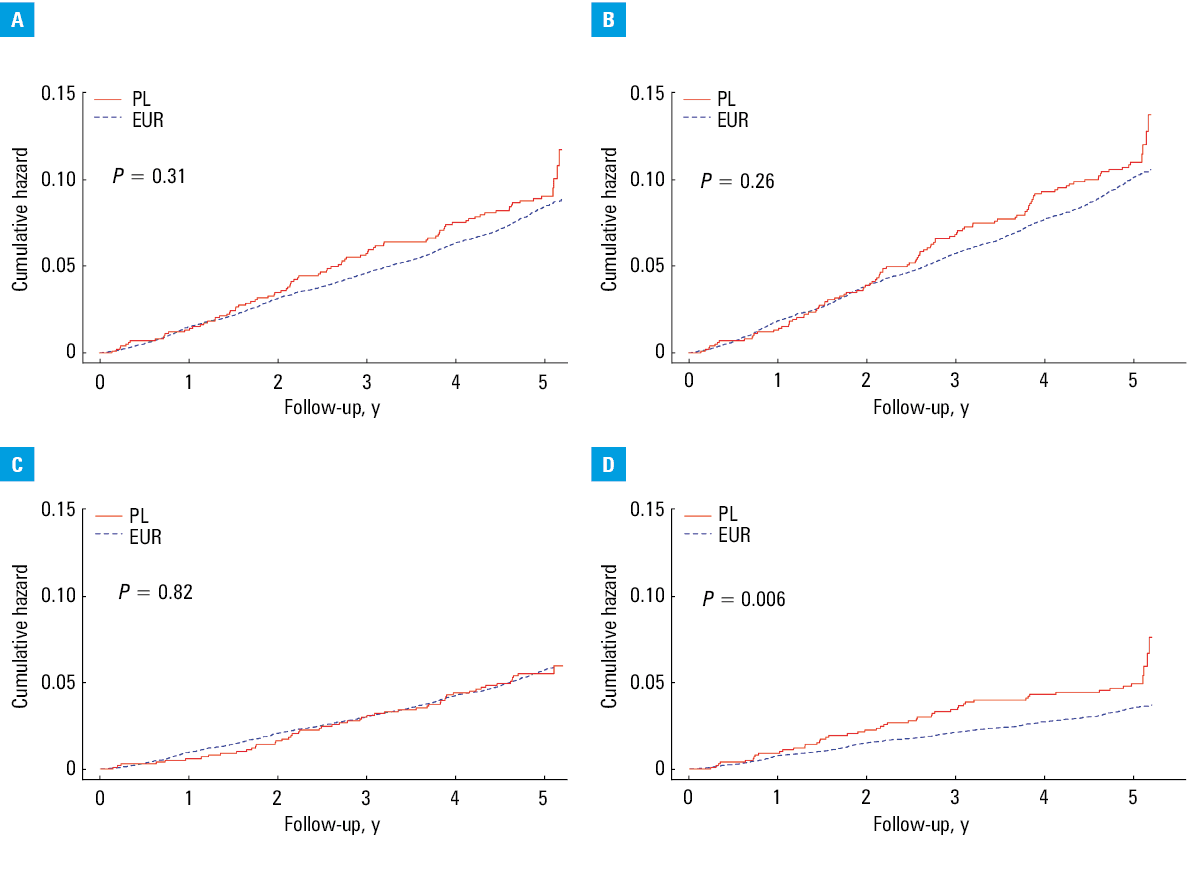
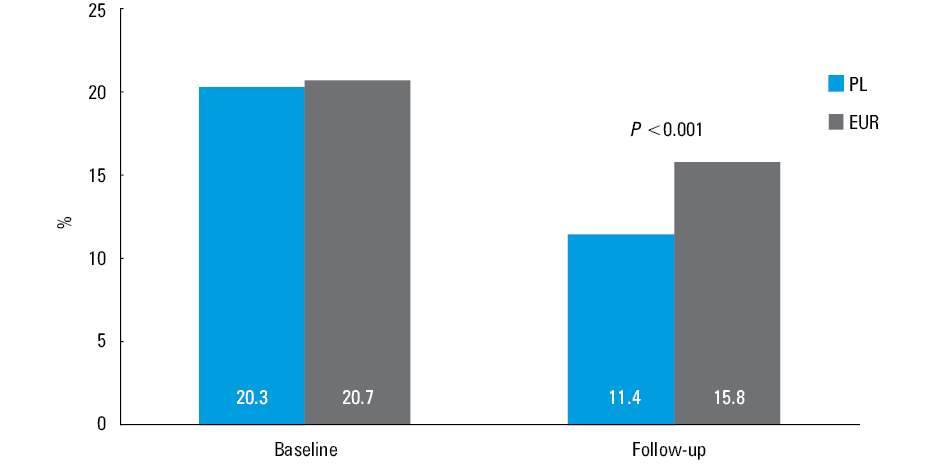
Clinical outcomes are presented in Table 3 and Figure 3. There was no difference in the combined double endpoint including cardiovascular death and nonfatal MI between patients from Poland and from other European countries (8.8% vs 7.2%, respectively; P = 0.31), as well as in the triple endpoint including cardiovascular death, nonfatal MI, and nonfatal stroke (10.5% vs 8.6%, respectively; P = 0.26). All‑cause, cardiovascular, and noncardiovascular mortality, as well as stroke rate, did not differ between groups. However, the incidence of MI was higher in the Polish cohort (5% vs 3.1%, respectively; P = 0.006). At the end of follow‑up, Polish patients had better angina control than patients from other European countries (11.5% vs 15.8% of patients with CCS class II to IV angina, respectively; P <0.001) (Figure 4).
Outcome | Events (PL compared with EUR; %) | HR (95% CI) | P value |
a For all death outcomes, the HR values are <1 despite higher proportion of patients experiencing the events in the Polish cohort than in the European cohort. This is due to the fact that the percent of events is only comparable between country groupings if the average follow‑up time is the same. There were more dropouts in other European countries than in Poland, and therefore the time of event accrual was shorter in the former than in the latter.
| |||
CV death or nonfatal MI | 8.8 vs 7.2 | 1.12 (0.90–1.39) | 0.3 |
CV death, nonfatal MI, or nonfatal stroke | 10.5 vs 8.6 | 1.12 (0.92–1.37) | 0.26 |
All‑cause deatha | 8.5 vs 7.9 | 0.97 (0.78–1.21) | 0.81 |
CV deatha | 5.3 vs 4.9 | 0.97 (0.73–1.28) | 0.82 |
Non‑CV deatha | 3.2 vs 2.9 | 0.98 (0.69–1.40) | 0.92 |
MI (fatal or nonfatal) | 5.0 vs 3.1 | 1.51 (1.13–2.01) | 0.006 |
Stroke (fatal or nonfatal) | 2.7 vs 2.2 | 1.14 (0.77–1.69) | 0.5 |
Discussion
We compared the treatment patterns and 5‑year outcomes in patients with SCAD enrolled in the contemporary CLARIFY registry from Poland and other European countries. We found that despite the wide use of antihypertensive drugs in both groups, only two‑thirds of patients with hypertension achieved target blood pressure values recommended by the guidelines.13 Lipid control in both cohorts was poor, with less than 20% of patients with dyslipidemia reaching the conventional target of LDL cholesterol concentration values below 1.8 mmol/l (70 mg/dl). Diabetes control was also inadequate, and significantly worse in Poland than in other European countries. Among patients who smoked at baseline, only about one‑fourth stopped smoking during the follow‑up. Myocardial revascularization was more common in Polish patients due to a more extensive use of PCI during the study, reflecting a good access to invasive treatment in Poland.14 All outcomes, including all‑cause and cardiovascular death, stroke, and a combination of cardiovascular death and MI, as well as cardiovascular death, MI, and stroke, did not differ between the groups, except for a higher incidence of MI in Polish patients. At the end of the 5‑year follow‑up, the prevalence of CCS class II–IV angina was significantly lower in the Polish cohort than in the European one.
Medical therapy
Patients in both groups received medical therapy according to the European Society of Cardiology (ESC) guidelines12 throughout the study. The proportion of patients on antiplatelet treatment was very high at baseline, with more aspirin, but less P2Y12 inhibitors in Polish patients, and a similar proportion of dual therapy. Lipid‑lowering treatment was also administered in over 90% of patients, with the predominant use of statins. The lower use of ACEIs in the European cohort was compensated by the more frequent use of angiotensin receptor blockers. At the end of the study, these proportions became somewhat lower, similarly to the findings from the ESC CAD pilot registry.15 The use of statins and antiplatelet agents in our patients was much higher than in the studies conducted at the beginning of the 21st century,16,17 and similar to that in more recent studies.18-20 Of note, the more frequent use of β-blockers in the Polish cohort than in the European one in our study might have partly contributed to better angina control.
Treatment‑to‑target approach
The 2013 ESC guidelines on the management of SCAD12 and the 2016 European Guidelines on cardiovascular prevention in clinical practice21 set out clear‑cut targets for several risk factors in patients with SCAD. Although the use of guideline‑recommended medication in our study was satisfactory, and similar to or better than in other studies,16-20 a large majority of patients did not reach the targets.
Our results are generally similar to those observed in the recent EUROASPIRE IV survey (European Action on Secondary Prevention through Intervention to Reduce Events), conducted in 24 European countries.22 At the 6‑month follow‑up in the hospital arm of EUROASPIRE IV including patients with CAD, over 40% of patients did not meet the criteria for adequate blood pressure control, about 20% achieved the target LDL cholesterol concentration of less than 1.8 mmol/l (70 mg/dl), and around a half of those with diabetes had glycated hemoglobin A1c values below 7%. In our study, blood pressure control was somewhat better (although still suboptimal), LDL cholesterol control was similar, and diabetes control was much worse than in EUROASPIRE IV. In both studies, the proportion of current smokers was low (13%–16%). In our study, only one‑fourth of patients quit smoking, as compared with over 50% in EUROASPIRE IV.23 Since there is a wide variation in cessation rates between countries, these results should be interpreted with caution.24 In general, our results reveal the need to direct careful attention not only to using evidence‑based therapy but also to achieving targets specified in the guidelines, especially in ambulatory patients with SCAD.
A systematic review and meta‑analysis of contemporary trials of cardiovascular prevention and rehabilitation25 showed that participation in comprehensive programs can improve the treatment to target of multiple risk factors, and thereby reduce the rates of all‑cause and cardiovascular mortality, MI, and stroke. In order to improve prognosis, patients with SCAD should be encouraged to join such programs.
Clinical outcome
Over the past 2 decades, it has become more difficult to manage patients with SCAD because of increased complexity of their medical problems.7 At the same time, the use of guideline‑based therapy has considerably increased,7 resulting in better clinical outcomes.26
Still, in patients with SCAD included in the recent ESC Pilot Registry,15 both all‑cause and cardiovascular death rates were high (3.4% and 3% at 6 months, respectively). It is difficult to compare the outcomes between different studies due to differences in inclusion criteria and duration of follow‑up, but assuming that the incidence of cardiovascular events in time is close to linear, our patients appeared to have better prognosis (all‑cause death rate at 5 years, 7.9%; cardiovascular death rate at 5 years, 5 %) than those in the ESC Pilot15 and the REACH (Reduction of Atherothrombosis for Continued Health) registries,27 and similar to those in the CORONOR (Cohort of Norway) study18 and the SIGNIFY trial (Study Assessing the Morbidity–Mortality Benefits of the If Inhibitor Ivabradine in Patients with Coronary Artery Disease).20
Importantly, in the present study, there was no difference in clinical outcomes between the groups, except for a higher rate of MI in the Polish cohort, which, to some extent, might have driven a higher rate of PCI. Nevertheless, the more frequent use of PCI in Poland cannot be solely due to a higher MI incidence. Regardless, in our study, PCI had no impact on prognosis, which is compatible with the findings from the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation).28
We have previously shown that patients managed by cardiologists might have lower rates of cardiovascular outcomes than those managed by noncardiologists.5 In the current analysis, almost all patients from other European countries were managed by cardiologists, while about one‑third of the Polish cohort were cared for by noncardiologists, with no impact on the composite outcomes and cardiovascular death. This further confirms our previous hypothesis that there is no clear evidence that cardiologists provide superior guideline‑based treatment, but the differences in outcome are most likely due to unquantifiable differences in patient characteristics.5
Angina
In the entire CLARIFY population, only a minority of patients with SCAD had angina symptoms.4 However, if present, angina with or without ischemia on noninvasive testing appeared to be associated with an increased risk of adverse cardiovascular outcomes.4 It is unclear whether alleviation of angina can result in improved mortality and morbidity, but it can definitely improve the quality of life.29 In our study, the more extensive use of β-blockers and PCI in the Polish cohort was associated with significantly better control of angina. This finding should be interpreted with caution, since we have no data on the indication for PCI (acute vs planned), and in addition, unidentified confounding factors cannot be excluded.
Study limitations
Our study has several important limitations. Since CLARIFY data came from an observational database, it was impossible to rule out selection bias and confounders. In addition, there was no central adjudication of events, although definitions of the events were provided in the case‑report forms. Direct monitoring involved only 5% of sites, while all the data were reviewed and queried remotely. Finally, the patients were recruited in 2009 and 2010, and followed up to 2015. Thus, our data may not strictly reflect current management strategies. Still, we think that our results provide important information on the treatment patterns and outcomes in patients with SCAD in Poland and other European countries.
Conclusions
Risk factor control was insufficient in both patients from Poland and other European countries. The more aggressive use of revascularization in Polish patients during the follow‑up was not linked to improved outcome, but, together with the more extensive prescription of β-blockers, it might have contributed to better angina control.
- Lopez AD, Mathers CD, Ezzati M, et al. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006; 367: 1747‑1757. | Crossref
- Ford I, Robertson M, Greenlaw N, et al. CLARIFY ‑ a simple risk model to predict cardiovascular death or myocardial infarction in patients with stable coronary artery disease. Presented at the ESC Congress 2018. August 25‑29, 2018; Munich, Germany. https://esc365.escardio.org. Accessed September 2, 2018.
- Kalra PR, Garcia‑Moll X, Zamorano J, et al. Impact of chronic kidney disease on use of evidence‑based therapy in stable coronary artery disease: a prospective analysis of 22272 patients. PLoS One. 2014; 9: e102335. | Crossref
- Steg PG, Greenlaw N, Tendera M, et al. Prevalence of angina symptoms and myocardial ischemia and their effect on clinical outcomes in outpatients with stable coronary artery disease: data from the international observational CLARIFY registry. JAMA Intern Med. 2014; 174: 1651‑1659. | Crossref
- Parma Z, Steg PG, Greenlaw N, et al. Differences in outcomes in patients with stable coronary artery disease managed by cardiologists versus noncardiologists. Pol Arch Intern Med. 2017; 127: 107‑114.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION