A large retroperitoneal tumor mimicking adrenocortical cancer arising in an adrenal rest



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A large retroperitoneal tumor mimicking adrenocortical cancer arising in an adrenal rest
We report a case of a 39‑year‑old man who complained of an observed increase in waist circumference as well as abdominal discomfort and early satiety following food intake. On physical examination, there was a palpable mass in the left epigastric region. A computed tomography (CT) scan revealed the presence of a very large retroperitoneal tumor (Figure 1A‑1D), with no evidence of infiltration of the adjacent tissues or distant metastases. In the native phase, the neoplasm was homogenous, with one small punctate calcification. The mass was well circumscribed, without any fat stranding. Both adrenal glands were normal in size, morphology, and localization. There were no clinical or biochemical indices of abnormal hormonal activity prior to surgery. The patient underwent complete surgical resection of the tumor via conventional retroperitoneal approach.
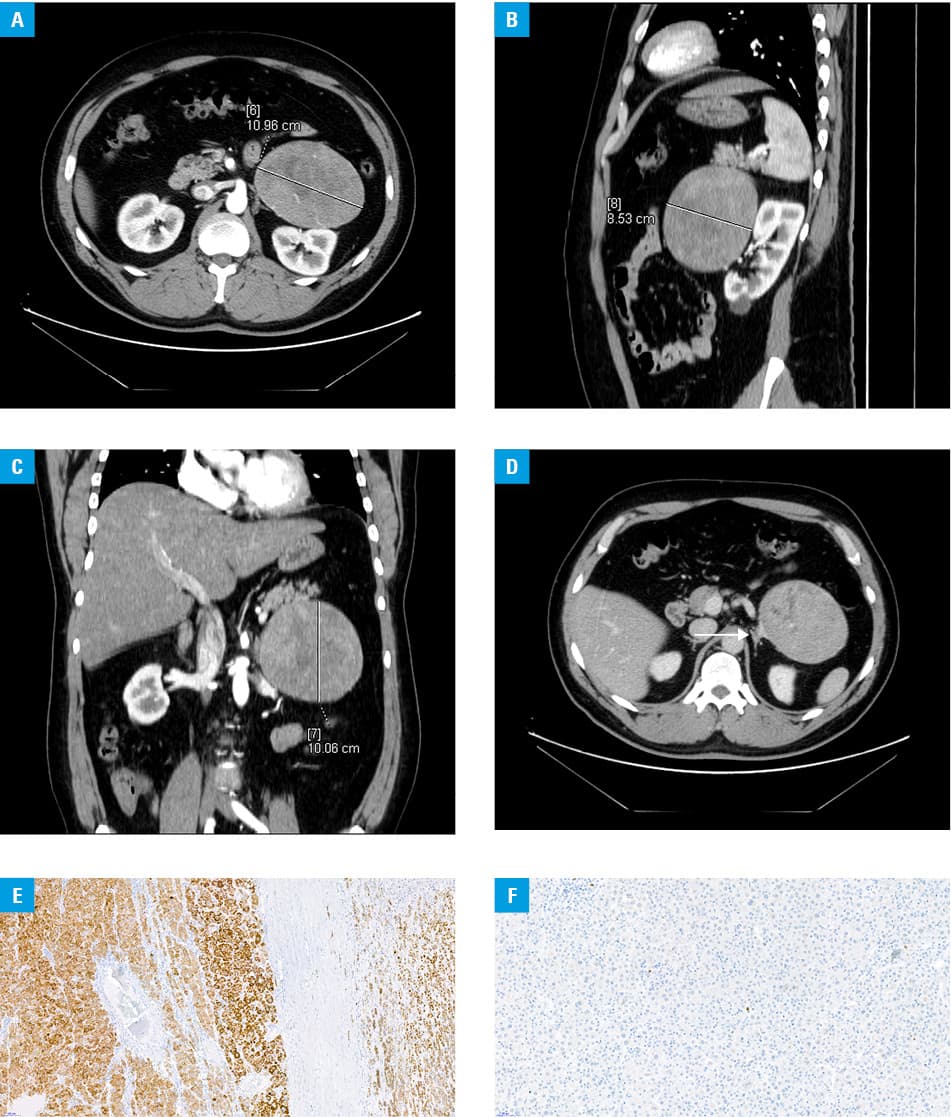
The initial histopathologic diagnosis of the tumor (measuring 15 × 9 × 6 cm) was adrenal adenocarcinoma. The immunohistochemical profile of the lesion was as follows: melan (+), inhibin (+), cytokeratin AE1/AE2 (+/–), synaptophysin (+), chromogranin (–), and the Ki67 index <1% (Figure 1Eand 1F). However, the absence of hormonal activity or any nearby tissue infiltration or distant metastases despite the extreme size of the tumor, the lack of a connection between the tumor and the adrenal gland on CT scans confirmed by 2 independent radiologists, extra‑adrenal anatomical location found on laparotomy, the presence of normal adrenal glands on a postsurgical CT scan, and full functional hormonal reserve of the adrenal glands following surgery suggested that the tumor most probably derived from heterotopic accessory adrenal tissue present in the retroperitoneal space (adrenal rest). The tumor fulfilled only the following Weiss criteria: focal invasion of the capsule, angioinvasion of a few small vessels of the capsule, and extensive necrosis (mostly ischemic).1 The mitotic rate was only 0–1/10 high power fields. The final consultation of histopathologic specimens resulted in a diagnosis of oncocytic adrenocortical neoplasm of uncertain malignant potential. The patient did not receive mitotane therapy. No recurrence or metastasis was observed during the 4 years of close monitoring and follow‑up.
A wide spectrum of benign and primary or metastatic malignant tumors can be found in the peritoneum and may constitute a diagnostic challenge.2 Although ectopic adrenal tissue is claimed to occur in 50% of neonates and children, it persists only in about 1% of adults.3 Though tumors arising from adrenal rest tend to be asymptomatic, they may occasionally present with hormonal activity or undergo neoplastic transformation.4 Considering a wide range of lesions that may arise in the retroperitoneal space, as well as their morphologic variability and histologic similarity, the differentiation between adrenocortical carcinoma and other benign or malignant adrenal neoplasms might be difficult.5 The size of the tumor and its clinical presentation in terms of symptoms associated with local growth and hormonal activity might be indicative of cancer.1,5 Additionally, adrenal cancers are in most cases functional, causing endocrinopathy.4 The accuracy of final diagnosis is crucial for proper postsurgical management planning, including the frequency of control imaging studies, selection of adjuvant therapy (ie, mitotane treatment), as well as prognosis assessment.
- Bednarczuk T, Bolanowski M, Sworczak K, et al. Adrenal incidentaloma in adults – management recommendations by the Polish Society of Endocrinology. Endokrynol Pol. 2016; 67: 234‑258. | Crossref
- Duralska M, Podkowińska‑Polak R, Kuzaka P, et al. Adrenal angiomyolipoma: a rare localization. Pol Arch Intern Med. 2019; 129: 848‑849.
- Barwick TD, Malhotra A, Webb JA, et al. Embryology of the adrenal glands and its relevance to diagnostic imaging. Clin Radiol. 2005; 60: 953‑959. | Crossref
- Cornejo KM, Afari HA, Sadow PM. Adrenocortical carcinoma arising in an adrenal rest: a case report and review of the literature. Endocr Pathol. 2017; 28: 165. | Crossref
- Cyrańska‑Chyrek E, Grzymisławska M, Ruchała M. Diagnostic pitfalls of adrenal incidentaloma. Endokrynol Pol. 2017; 68: 360‑377.
ARTICLE INFORMATION