Insulinoma mimicking psychogenic nonepileptic seizures in a patient with refractory epilepsy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Insulinoma mimicking psychogenic nonepileptic seizures in a patient with refractory epilepsy
Epilepsy has a high rate of false‑positive diagnoses.1 Seizures may be mimicked by several conditions including syncope, psychogenic nonepileptic seizures (PNESs), and hypoglycemia. Insulinoma is an uncommon tumor that produces excess amounts of insulin, resulting in hypoglycemia. Neuropsychiatric symptoms of insulinoma‑related hypoglycemia are frequently misdiagnosed as seizures.2-5 We describe a patient diagnosed both with insulinoma and epilepsy.
A 39‑year‑old man with epilepsy was referred to the department of neurology with suspicion of PNES. His epilepsy started at the age of 19 years with episodes of unresponsiveness as well as oral and gestural automatisms consistent with temporal lobe seizures. Computed tomography of the brain was normal, while electroencephalogram revealed focal sharps in the right temporal region. Magnetic resonance imaging (MRI) was not performed because of the presence of metallic osteosynthesis material in his maxilla and right humerus. Despite the use of many antiepileptic drugs, he continued to have 4 to 5 seizures lasting 2 to 3 minutes per month. The new episodes differed from his previous seizures. For the past 4 months, the patient had experienced numerous episodes of weakness, sweating, tremor, and confusion lasting 5 to 25 minutes and occurring more often before breakfast. Neurologic and general examinations were unremarkable, and medications included valproate, levetiracetam, and gabapentin. On admission, low blood glucose levels were detected (1.8 mmol/l; normal range, 3.3–5.6 mmol/l). Repeated measurements demonstrated consistently low levels with numerous concentrations of less than 1.0 mmol/l. The patient was transferred to the department of endocrinology for further investigation.
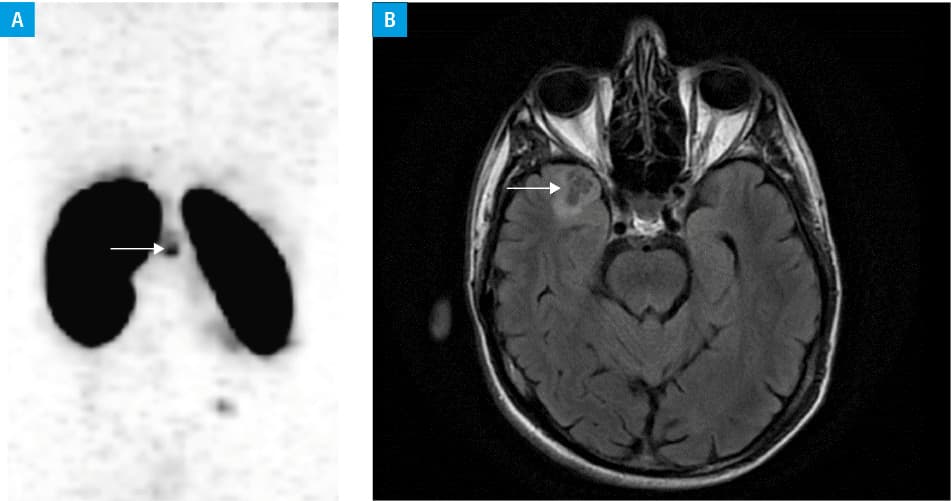
Whole‑body scintigraphy with somatostatin analogue showed tracer accumulation in the projection of the pancreas (Figure 1A). The patient underwent abdominal surgery with excision of the insulinoma and complete resolution of hypoglycemic episodes. Histopathologic investigation confirmed a pancreatic islet cell low‑grade tumor (insulinoma). Subsequently, metallic elements were removed and brain MRI was performed, revealing a right temporal tumor (Figure 1B). The patient underwent brain surgery. Histopathology revealed a dysembryoplastic neuroepithelial tumor. Antiepileptic drugs have been discontinued, with no recurrence of seizures. Five years after abdominal and brain surgeries, the patient was symptom free.
Metabolic causes of seizure‑like episodes such as hypoglycemia are potentially curable and may be fatal if untreated. Insulinoma is the most common pancreatic neuroendocrine tumor and is the most common endogenous cause of hyperinsulinemic hypoglycemia. The diagnosis of insulinoma is often delayed, with a substantial proportion of patients with a false diagnosis of epilepsy.5 Several reports on insulinomas misdiagnosed as epilepsy have been published.2,3 Fox et al4 described insulinoma triggering both neuroglycopenic episodes and seizures in a patient with well‑controlled epilepsy. To the best of our knowledge, this is the first report on a patient with pharmacoresistant epilepsy and insulinoma. Moreover, 2 types of low‑grade tumors, dysembryoplastic neuroepithelial tumor and insulinoma, were diagnosed and surgically removed in our patient. At long‑term follow‑up, the patient was seizure free and hypoglycemia free. This report highlights the need for a careful assessment of new seizure types emerging in a patient with epilepsy. In most cases of epilepsy coexisting with other types of paroxysmal episodes, PNESs are diagnosed. Although PNESs have been suspected in this case, investigations revealed neuroglycopenic episodes.
In conclusion, although very rare, the possibility of the co‑occurence of epileptic seizures and hypoglycemic episodes due to insulinoma should be considered in the presence of a new type of paroxysmal events.
- Xu Y, Nguyen D, Mohamed A, et al. Frequency of a false positive diagnosis of epilepsy: a systematic review of observational studies. Seizure. 2016; 41: 167‑174. | Crossref
- Aupy J, Benoilid A, Sarhan M, et al. Misleading features of neuroimaging and electroencephalography: insulinoma misdiagnosed as temporal lobe epilepsy. Epileptic Disord. 2013; 15: 93‑97. | Crossref
- Deleo F, Matricardi S, Didato G, et al. An unusual behavioural and motor paroxysmal disorder caused by insulinoma‑related hypoglycemia: a possible cause of epilepsy misdiagnosis. Seizure. 2014; 23: 909‑911. | Crossref
- Fox R, Heartshorne R, Kobylecki C, Murphy C. An unusual cause of seizures. Pract Neurol. 2015; 15: 145‑147. | Crossref
- Falconi M, Eriksson B, Kaltsas G, et al. ENETS Consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non‑functional pancreatic neuroendocrine tumors. Neuroendocrinology. 2016; 103: 153‑171. | Crossref
ARTICLE INFORMATION