Clinical outcomes and plasma clot permeability and lysability in patients with venous thromboembolism on rivaroxaban: a cohort study
Key words: bleeding, clot properties, fibrin, rivaroxaban, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Clinical outcomes and plasma clot permeability and lysability in patients with venous thromboembolism on rivaroxaban: a cohort study
Introduction: Denser fibrin structure and impaired fibrinolysis reported in patients following venous thromboembolism (VTE) can predict recurrent VTE after cessation of anticoagulation.
Objectives: The aim of the study was to investigate whether the properties of fibrin clot may be useful in predicting adverse events in patients with VTE receiving rivaroxaban.
Patients and methods: In 132 patients with VTE treated with rivaroxaban for 8 weeks or longer, we determined plasma clot permeability (Ks) and clot lysis time (CLT) in blood samples collected 2 to 28 hours after rivaroxaban intake (20 mg/d). The primary endpoint was a composite of major and clinically relevant nonmajor bleeding, while the secondary endpoint was recurrent symptomatic VTE.
Results: During a median follow‑up of 32 months, the annual rates of primary and secondary endpoints were 3.6% and 2.7%, respectively. There were no differences in Ks and CLT between individuals who experienced the primary endpoint and the remainder. Patients with recurrent VTE had lower baseline Ks (–26.7%) and prolonged CLT (+20.8%) on rivaroxaban, without differences in rivaroxaban concentrations at the time of blood collection. After adjustment for confounding factors, Ks was the only predictor of VTE recurrence on rivaroxaban (odds ratio, 0.23; 95% CI, 0.06–0.94).
Conclusions: Our study suggests that Ks assessed on rivaroxaban may provide prognostic information about the risk of recurrent VTE in anticoagulated patients.
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), afflicts over 1 million people in Europe annually.1 The 1‑year incidence of recurrent VTE is approximately 2% among patients receiving direct oral anticoagulants (DOACs) or vitamin K antagonists (VKAs),2 and rises to 11% at 1 year and 30% at 5 years among individuals following unprovoked VTE after cessation of anticoagulation.3 The main established risk factors predisposing to VTE recurrence include older age, male sex, high body mass index (BMI), active cancer, unprovoked VTE, proximal DVT or PE, antiphospholipid antibody syndrome, short duration of anticoagulant treatment, and persistently increased plasma fibrin D‑dimer levels.4 It is well known that VTE provoked by transient risk factors is associated with lower recurrence risk compared with an unprovoked VTE, and in most cases a 3‑month anticoagulant treatment is recommended.5 Furthermore, elimination of exposure to immobilization, surgery, and trauma in patients with a first unprovoked VTE episode does not result in a decreased risk of recurrence.6
Direct oral anticoagulants are now commonly used in acute VTE treatment and secondary prevention of recurrences.7 Compared with VKAs, treatment with DOACs in patients with VTE is associated with a 39% reduction in bleeding risk and 64% reduction in mortality rates with similar efficacy.8 Rivaroxaban is the most commonly used DOAC among VTE patients in the majority of European countries.9 The EINSTEIN‑PE (Oral Direct Factor Xa Inhibitor Rivaroxaban in Patients With Acute Symptomatic Pulmonary Embolism) and EINSTEIN‑DVT (Oral Direct Factor Xa Inhibitor Rivaroxaban in Patients With Acute Symptomatic Deep Vein Thrombosis) studies showed that the risk of VTE recurrence is 2.1% during a 3- to 12‑month rivaroxaban treatment in patients with DVT or PE, while the risk of major or clinically relevant nonmajor bleeding is 8.1% and 10.3% in patients with DVT and PE, respectively.10,11 The risk of bleeding on rivaroxaban is increased by the following factors: older age, prior bleeding, malignancy‑associated VTE, renal and liver impairment, bleeding disorders, and concurrent use of antiplatelet drugs, while previous unprovoked VTE, active cancer, proximal DVT or PE, and elevated plasma D‑dimer levels have been reported as risk factors of VTE recurrences on rivaroxaban.12,13
Fibrin, a major component of venous thrombi, forms highly variable networks of different density and lysability governed by genetic and environmental factors.14 Denser fibrin clots displaying impaired lysability have been shown to be associated with an increased risk of VTE and its recurrence.15,16 It is known that effective fibrinolysis is essential for fibrin clot degradation and, subsequently, maintaining vessel patency.17 In vitro studies have demonstrated that rivaroxaban prolongs the initiation phase of thrombin generation, reduces the maximum concentration of thrombin generated, and renders the fibrin structure more permeable and susceptible to fibrinolysis.18,19 Janion‑Sadowska et al20 have shown recently that rivaroxaban at peak plasma concentrations improves plasma clot permeability and clot lysis time (CLT) in patients with previous VTE by 37% and 25%, respectively. The prothrombotic clot phenotype, reflected by clot permeability, being the main measure of clot structure, has been shown to be an independent predictor of thromboembolic events and major bleeding in patients with atrial fibrillation receiving VKA.21,22
To the best of our knowledge, it is unknown whether plasma fibrin clot properties assessed in patients on rivaroxaban during ambulatory visits may be useful in predicting thromboembolic and/or bleeding episodes in those after VTE. Therefore, our aim was to evaluate a predictive value of clot permeability and CLT in relation to plasma rivaroxaban concentrations in a cohort of patients with VTE.
Patients and methods
Patients
We recruited 132 consecutive adult patients with documented DVT and/or PE who were treated with rivaroxaban (20 mg/d) and were referred to our Center for Coagulation Disorders for clinical or laboratory workup. Patients were eligible if at least 8 weeks elapsed since the index event. The exclusion criteria were: age below 18 or above 65 years, signs of acute infection, acute coronary syndrome or ischemic stroke within the previous 3 months, indications for anticoagulant therapy other than VTE, known malignancy, chronic kidney disease stage 4 or 5, indications for anticoagulation other than VTE (eg, atrial fibrillation), self‑declared interruption in rivaroxaban use longer than 48 hours within the previous 6 weeks, major surgery or trauma within the preceding 3 months. All enrolled patients declared regular rivaroxaban intake.
The diagnosis of DVT was established by a positive finding on Doppler vein ultrasound (visualization of an intraluminal thrombus in calf, popliteal, femoral, or iliac veins). The diagnosis of PE was based on the presence of typical symptoms and positive results on high‑resolution spiral computed tomography (CT). The diagnosis of thrombosis at unusual sites (cerebral venous sinus thrombosis, portal vein thrombosis) were based on clinical symptoms combined with abnormalities on CT angiography, magnetic resonance imaging, or magnetic resonance angiography.
Unprovoked VTE was defined as VTE in a patient with no history of cancer, surgery or trauma, plaster cast, immobilization, or hospitalization in the past 3 months, use of oral contraceptives or hormone replacement therapy, and pregnancy or delivery in the past 3 months.
Data concerning demographic characteristics, risk factors for VTE, comorbidities, and current treatment were collected from all participants using a standardized questionnaire. Family history of VTE was defined as a confirmed VTE episode in a first‑degree relative. Arterial hypertension was established as systolic blood pressure of 140 mm Hg and/or diastolic blood pressure 90 mm Hg and/or treatment with antihypertensive drugs. Diabetes mellitus was defined according to the American Diabetic Association criteria. Obesity was defined as a BMI of 30 kg/m2 or greater. Coronary heart disease was established based on a documented history of myocardial infarction or a positive result on exercise stress test, or gated single‑photon emission CT (SPECT) with technetium (99mTc) sestamibi, or coronary angiography. Hypercholesterolemia was defined as a total cholesterol level of 5.2 mmol/l or higher, or a low‑density lipoprotein cholesterol level of 3 mmol/l or higher, and hypertriglyceridemia as a triglyceride concentration above 1.7 mmol/l. Hyperhomocysteinemia was defined as a plasma homocysteine concentration of 15 µmol/l or higher.
The ethical committee of Jagiellonian University approved the study. All participants gave informed consent in accordance with the Declaration of Helsinki.
Laboratory tests
Blood samples were drawn from an antecubital vein with minimal stasis using atraumatic venipuncture between 09:00 AM and 12:00 PM. Rivaroxaban was taken 2 to 28 hours prior to blood collection based on the patient’ declaration. Lipid profiles, complete blood count, glucose, and creatinine were assayed by routine laboratory techniques. Fibrinogen was determined using the Clauss assay. High‑sensitivity C‑reactive protein was measured by immunoturbidimetry (Roche Diagnostics, Mannheim, Germany). Plasma D‑dimer was measured with the Innovance D‑dimer assay (Siemens, Marburg, Germany).
All patients were tested for thrombophilia, including antithrombin, protein C, or protein S deficiency, factor V Leiden, and prothrombin G20210A polymorphism, as described elsewhere.23
Rivaroxaban concentrations were measured by the anti‑Xa chromogenic assay, Biophen DiXaI (Hyphen Biomed, Neuville‑sur‑Oise, France), according to the manufacturer’s instructions.24 We arbitrarily used the cutoff vaule of 30 µg/l25 and prespecified the group with low rivaroxaban concentrations (≤30 μg/l) and the group with high rivaroxaban concentrations (>30 μg/l).
Fibrin clot evaluation
To evaluate clot properties, venous blood samples (volume‑to‑volume ratio, 3.2% trisodium citrate at an anticoagulant‑to‑blood ratio of 9 to 1) were centrifuged at 2000 × g for 10 minutes within 30 minutes of the draw, and the supernatant was aliquoted and stored at –80°C until analysis. All measurements were performed by technicians blinded to the origin of the samples. Intra‑assay and interassay coefficients of variation were approximately 7%.
Fibrin clot permeability
Clot permeability, indicating the pore size in fiber networks, is proportional to a volume of buffer percolating through a clot under a specific hydrostatic pressure and was determined using a pressure‑driven system as described elsewhere.17 Briefly, calcium chloride (20 mmol/l) and human thrombin (1 U/ml, Calbiochem) were added to 120 µl of citrated plasma. Tubes which contained the clots were joined with a reservoir of Tris‑buffered saline (0.1 mol/l NaCl, 0.01 mol/l Tris, pH 7.5). The volume flowing for 60 minutes through the gels was assessed. Plasma clot permeability was expressed as a permeation coefficient (Ks) and was calculated from the equation: Ks = (Q × L × µ) / (t × A × Δp), where Q is the flow rate in time; L, the length of a fibrin gel; µ, the viscosity of liquid (in poise); A, the cross‑sectional area (in cm2), Δp, a differential pressure (in dyne/cm2), and t the percolating time.26
Clot lysis time
To assess CLT, we used a modified lysis assay introduced by Lisman et al.27,28 Briefly, citrated plasma was mixed with 16 mmol/l calcium chloride, 10000 pg/ml human tissue factor (Innovin, Siemens) with a final concentration of 0.6 pmol/l, 12 µmol/l phospholipid vesicles, and 32 ng/ml rtPA (Boehringer Ingelheim, Ingelheim, Germany). The turbidity was measured at 405 nm at 37°C. Clot lysis time was defined as the time from the midpoint of the clear‑to‑maximum‑turbid transition, which represents clot formation, to the midpoint of the maximum‑turbid‑to‑clear transition, which represents clot degradation.29
Follow‑up
The follow‑up started on the day of blood collection and was carried out on the 6‑month basis (a visit at the center or a telephone contact). The primary endpoint was major bleeding or clinically relevant nonmajor bleeding defined according to the International Society on Thrombosis and Hemostasis criteria.30 The secondary endpoint was recurrent symptomatic VTE defined as a subsequent VTE episode during follow‑up, using the same criteria as at the index event with imaging in each case. In cases of a suspected recurrence of DVT in the same leg as the index event, noncompressibility of a previously compressible venous segment or an increase of at least 4 mm in the residual diameters were applied to confirm the diagnosis. Patients with suspected PE underwent spiral CT, followed by pulmonary angiography in the case of a high clinical probability despite normal CT scans. In patients with signs or symptoms suggestive of DVT, color duplex sonography was performed.
Statistical analysis
The study was powered to have a 90% chance of detecting a 10% difference in CLT using an α value of 0.05, based on the CLT values presented elsewhere.31 To demonstrate such a difference or greater, 34 patients were required in each group. In turn, to demonstrate such a difference or greater in Ks using an α value of 0.05, at least 31 patients were required in each group.15
Categorical variables are presented as numbers and percentages. Continuous variables are expressed as mean (SD) or median and interquartile range (IQR), as appropriate. Normality was assessed by the Shapiro–Wilk test. Equality of variances was assessed using the Levene test. The continuous variables were compared between 2 groups using the t test for nonrelated groups for mean values and the Mann–Whitney test for median values. Categorical variables were analyzed using the χ2 test or the Fisher exact test, as appropriate. The Pearson correlation coefficient or Spearman rank correlation coefficient were calculated to assess the linear correlations between variables with normal or nonnormal distribution, respectively. Prognostic values of Ks and CLT were analyzed with logistic regression models (univariable and multivariable; the results were presented as odds ratios (ORs) and their 95% CIs. The univariate models were built to assess the crude odds ratios for the relation between factors and the outcome. Multivariable models were adjusted for potential confounders including age, sex, BMI, fibrinogen, unprovoked VTE status, and plasma rivaroxaban concentrations. A P value of less than 0.05 was considered significant. All calculations were done with STATISTICA 13.0 software (StatSoft Inc., Tulsa, Oklahoma, United States).
Results
Patient characteristics
A total of 132 patients (62 men and 70 women) were included into the analysis (Table 1). There were 48 patients (36.4%) with isolated DVT, 30 patients (22.7%) with PE alone, 49 patients (37.1%) with PE combined with DVT, and 5 patients (3.8%) with cerebral venous sinus thrombosis or portal vein thrombosis. A total of 72 patients (54.5%) experienced unprovoked VTE. The time from the last VTE to enrollment ranged between 2 and 65 months (median [IQR], 32 [19‑40]).
Variable | Low rivaroxaban levels (n = 67) | High rivaroxaban levels (n = 65) | P value |
a Women only
Abbreviations: BMI, body mass index; CLT, clot lysis time; HDL‑C, high‑density lipoprotein cholesterol; hs‑CRP, high‑sensitivity C‑reactive protein; IQR, interquartile range; Ks, clot permeability; LDL‑C, low‑density lipoprotein cholesterol; PE, pulmonary embolism; TC, total cholesterol; VTE, venous thromboembolism | |||
Age, y, median (IQR) | 42 (19) | 41 (18) | 0.83 |
Male sex, n (%) | 29 (43.28) | 33 (50.77) | 0.39 |
BMI, kg/m2, median (IQR) | 27.78 (8.22) | 26.40 (5.51) | 0.14 |
Cigarette smoking, n (%) | 16 (23.88) | 13 (20) | 0.59 |
Oral contraceptivesa, n (%) | 14 (36.84) | 12 (37.5) | 0.84 |
Family history of VTE, n (%) | 21 (31.34) | 17 (26.15) | 0.51 |
Varices, n (%) | 25 (37.31) | 21 (32.31) | 0.55 |
Unprovoked VTE, n (%) | 35 (56.92) | 37 (52.24) | 0.59 |
Obesity, n (%) | 15 (23.08) | 25 (37.31) | 0.08 |
Comorbidities, n (%) | |||
Arterial hypertension | 22 (32.84) | 19 (29.23) | 0.65 |
Diabetes mellitus | 2 (2.99) | 3 (4.62) | 0.62 |
Coronary heart disease | 3 (4.48) | 2 (3.08) | 0.67 |
Hypercholesterolemia | 33 (49.25) | 42 (64.62) | 0.07 |
Hypertriglyceridemia | 10 (14.93) | 11 (16.92) | 0.75 |
Laboratory investigations | |||
Hemoglobin, g/dl, median (IQR) | 14 (1.7) | 14.2 (2.0) | 0.53 |
Platelets, 103/μl, median (IQR) | 226 (69) | 246 (74) | 0.05 |
Creatinine, μmol/l, median (IQR) | 69 (17) | 72 (21) | 0.35 |
Glucose, mmol/l, median (IQR) | 5.2 (0.7) | 5.2 (0.8) | 0.74 |
Triglycerides, mmol/l, median (IQR) | 1.04 (0.77) | 1.17 (0.7) | 0.38 |
TC, mmol/l, median (IQR) | 5.08 (1.32) | 5.07 (1.25) | 0.9 |
HDL‑C, mmol/l, median (IQR) | 1.52 (0.56) | 1.45 (0.51) | 0.16 |
LDL‑C, mmol/l, median (IQR) | 3.25 (1.3) | 3.35 (1.2) | 0.58 |
hs‑CRP, mg/l, median (IQR) | 1.48 (2.81) | 1.32 (2.9) | 0.68 |
D‑dimer, ng/ml, median (IQR) | 270 (206) | 216 (152) | 0.04 |
Fibrinogen, g/l, median (IQR) | 3 (1.26) | 3.11 (0.97) | 0.96 |
Ks, 10–9 cm2, median (IQR) | 6.37 (1.6) | 9.04 (2) | 0.01 |
CLT, min, mean (SD) | 107.8 (19.7) | 70.66 (19.5) | 0.01 |
Thrombophilia, n (%) | |||
Factor V Leiden | 19 (28.36) | 20 (30.77) | 0.76 |
Prothrombin 20210A mutation | 7 (10.45) | 4 (6.15) | 0.27 |
Protein C deficiency | 1 (1.54) | 2 (2.99) | 0.58 |
Protein S deficiency | 2 (3.08) | 4 (5.97) | 0.43 |
Antithrombin deficiency | 1 (1.54) | 2 (2.99) | 0.58 |
Hyperhomocysteinemia | 16 (23.88) | 11 (16.92) | 0.32 |
Based on rivaroxaban concentrations at the time of blood collection, 2 subgroups were distinguished: with high rivaroxaban concentrations (n = 65, 49.2%) and with low rivaroxaban concentrations (n = 67, 50.8%), with a median (IQR) drug concentration of 103 (47–195) µg/l and 3 (0–13) µg/l, respectively (Table 1). The mean time from the last rivaroxaban administration was 12 (4–20) hours and 25 (22–27) hours, respectively. As expected, the plasma rivaroxaban concentration was inversely correlated with time from its last intake (r = –0.66, P <0.01). There were no intergroup differences with regard to demographic variables, VTE risk factors, and comorbidities (Table 1). In terms of routine laboratory tests, the group with low rivaroxaban concentrations had higher D‑dimer concentrations and lower platelet count, without other intergroup differences, including fibrinogen (Table 1).
The analysis of thrombophilias yielded similar frequencies in both groups (Table 1). The prothrombin 20210A mutation tended to occur more often in the group with high rivaroxaban levels, although the difference did not reach the level of significance.
Fibrin clot properties
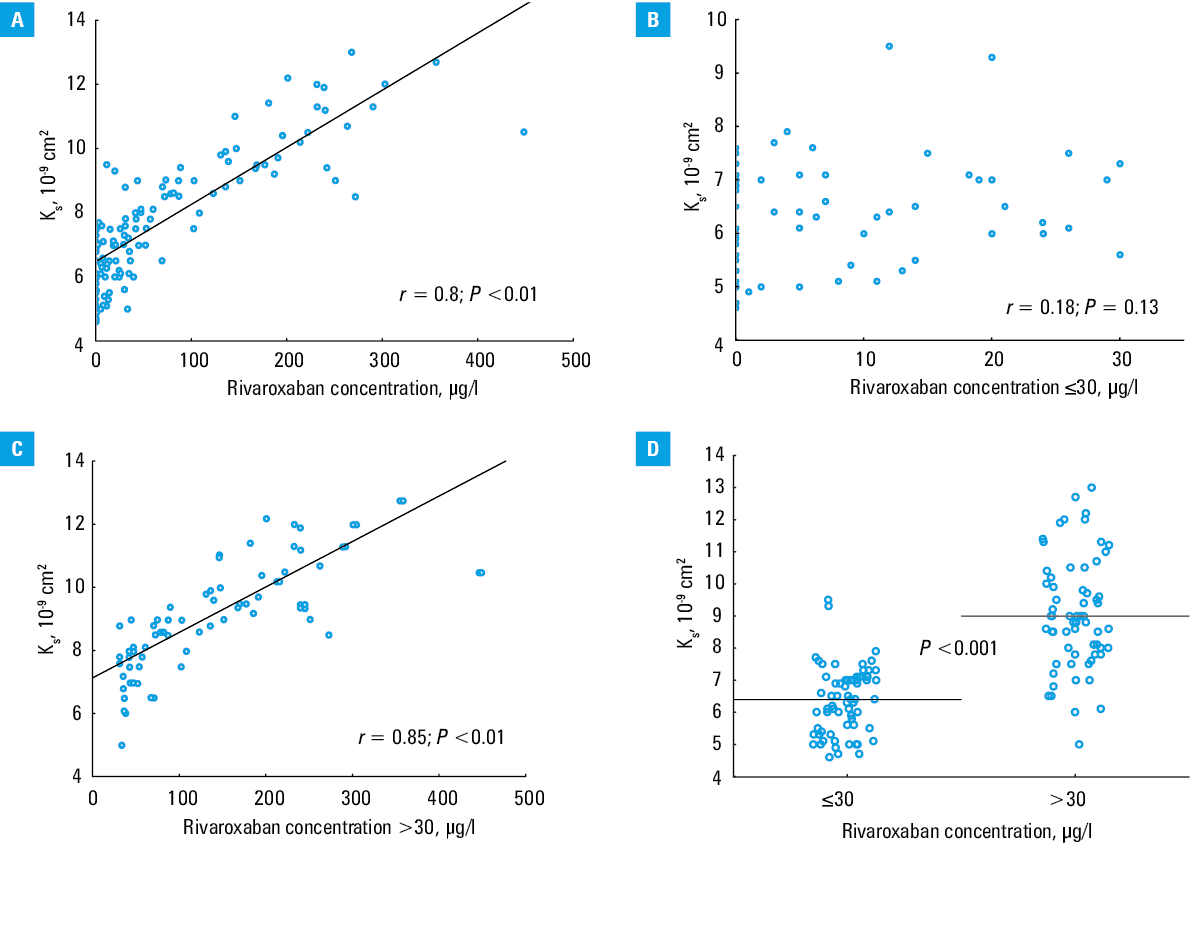
Plasma rivaroxaban concentrations were strongly positively correlated with Ks in the whole group (r = 0.8, P = 0.01) (Figure 1A). There was no correlation between plasma rivaroxaban concentrations and Ks in the group with low rivaroxaban concentrations (r = 0.18, P = 0.13) (Figure 1B), whereas in the group with high rivaroxaban concentrations, there was a positive correlation between Ks and drug concentrations (r = 0.85, P = 0.01) (Figure 1C). Patients in the low rivaroxaban group formed denser clots (mean [SD] Ks, 6.37 [1.6] 10–9 cm2 vs 9.04 [2] 10–9 cm2; P <0.001) (Figure 1D).
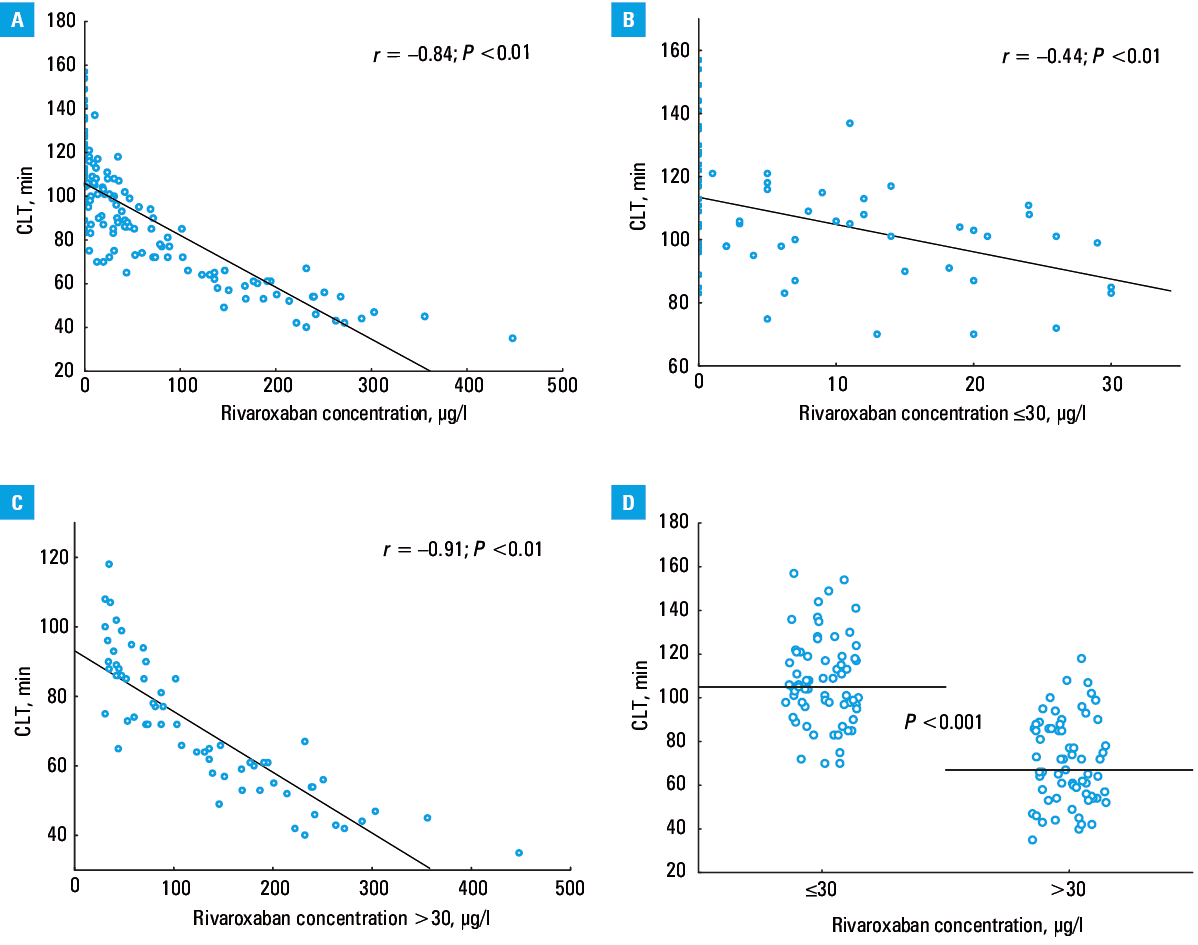
Clot lysis time correlated inversely with rivaroxaban concentrations in the whole group (r = –0.85, P = 0.01) (Figure 2A), and both in the group with low rivaroxaban concentrations (r = –0.44, P = 0.01) (Figure 2B) and with high rivaroxaban concentrations (r = –0.91, P <0.001) (Figure 2C). The group with low rivaroxaban concentrations had 57% longer CLT compared with the high rivaroxaban group (mean [SD], 107.9 [19.7] min vs 70.7 [19.5] min; P <0.001) (Figure 2D).
Both CLT and Ks were correlated with time from the last rivaroxaban administration (r = 0.61, P = 0.01 and r = –0.59, P = 0.01, respectively).
Follow‑up
The follow‑up ranged from 5 to 61 months (median, 32 months) and comprised 329.7 patient‑years. None of the patients was lost to follow‑up. We observed 12 major bleeds or clinically relevant nonmajor bleeding events (9.1% and 3.6% per year, respectively), including 7 patients with gastrointestinal bleeding (58% of all events). There was no difference between the group with high rivaroxaban concentrations and the group with low rivaroxaban concentrations in this regard (n = 6; 9.23% vs n = 6; 8.96%, respectively; P = 0.96). Among individuals who experienced significant bleeding during follow‑up, 6 patients had a history of proximal isolated DVT and 6 experienced PE. Acetylsalicylic acid or statins were used at a similar rate among patients with or without bleedings (P = 0.52 and P = 0.45, respectively) (Table 2). There was no difference in Ks and CLT values between patients who experienced relevant bleeding or not (Table 2).
Variable | Patients with VTE recurrence (n = 9) | Patients without VTE recurrence (n = 123) | Patients with bleeding (n = 12) | Patients without bleeding (n = 120) |
a Women only; b P value <0.05
Abbreviations: ASA, acetylsalicylic acid; others, see Table 1 | ||||
Age, y, median (IQR) | 43 (12) | 41 (19) | 41.5 (18) | 41.5 (18.5) |
Male sex, n (%) | 4 (44.4) | 58 (47.2) | 7 (58.3) | 55 (45.8) |
BMI, kg/m2, median (IQR) | 29.1 (6.4) | 26.8 (7.6) | 27.3 (7.7) | 26.9 (7.1) |
Cigarette smoking, n (%) | 3 (33.3) | 26 (21.1) | 2 (16.7) | 27 (22.5) |
Oral contraceptivesa, n (%) | 1 (20) | 25 (38.5) | 1 (20) | 25 (38.5) |
Family history of VTE, n (%) | 4 (44.4) | 34 (27.6) | 4 (33.3) | 34 (28.3) |
Varices, n (%) | 3 (33.3) | 43 (35) | 2 (16.7) | 44 (36.7) |
Unprovoked VTE, n (%) | 8 (88.9) | 64 (52)b | 3 (25) | 69 (57.5)b |
Obesity, n (%) | 4 (44.4) | 36 (29.3) | 4 (33.3) | 36 (30) |
Use of ASA, n (%) | 0 (0) | 4 (3.25) | 0 (0) | 4 (3.33) |
Use of statins, n (%) | 0 (0) | 21 (17.1) | 1 (8.33) | 20 (16.7) |
Comorbidities, n (%) | ||||
Arterial hypertension | 3 (33.3) | 38 (30.9) | 2 (16.7) | 39 (32.5) |
Diabetes mellitus | 1 (11.1) | 4 (3.25) | 1 (8.3) | 4 (3.3) |
Coronary heart disease | 1 (11.1) | 4 (3.25) | 0 (0) | 5 (4.2) |
Hypercholesterolemia | 3 (33.3) | 72 (58.5) | 6 (50) | 69 (57.5) |
Hypertriglyceridemia | 0 (0) | 21 (17.1) | 0 (0) | 21 (17.5) |
Laboratory investigations | ||||
Hemoglobin, g/dl, mean (SD) | 14.3 (2.7) | 14.1 (1.8) | 13.6 (2.2) | 14.05 (1.6) |
Platelets, 103/μl, median (IQR) | 209 (66) | 242 (72) | 222 (74.5) | 242 (74) |
Creatinine, μmol/l, median (IQR) | 81 (17.8) | 72.9 (14.9) | 72.5 (22.5) | 69 (19) |
Glucose, mmol/l, median (IQR) | 5 (0.2) | 5.2 (0.8) | 5.35 (1.25) | 5.2 (0.7) |
Triglycerides, mmol/l, median (IQR) | 1.24 (0.66) | 1.05 (0.77) | 1.01 (0.57) | 1.12 (0.77) |
TC, mmol/l, median (IQR) | 5.06 (0.9) | 5.08 (1.29) | 5.11 (1.62) | 5.08 (1.27) |
HDL‑C, mmol/l, median (IQR) | 1.46 (0.35) | 1.47 (0.54) | 1.59 (0.75) | 1.46 (0.51) |
LDL‑C, mmol/l, median (IQR) | 3.41 (1.5) | 3.29 (1.26) | 3.42 (1.19) | 3.28 (1.27) |
hs‑CRP, mg/l, median (IQR) | 0.94 (1.71) | 1.44 (2.87) | 1.28 (1.42) | 1.43 (2.84) |
D‑dimer, ng/ml, median (IQR) | 270 (144) | 236 (183) | 269 (170.5) | 234.5 (184.5) |
Fibrinogen, g/l, median (IQR) | 3.17 (0.57) | 3.03 (1.19) | 2.65 (0.59) | 3.13 (1.23)b |
Ks, 10–9 cm2, median (IQR) | 5.5 (0.8) | 7.8 (2.5)b | 7.1 (2.9) | 7.85 (1.55) |
CLT, minutes, median (IQR) | 106.7 (24.5) | 88.3 (26.8)b | 89 (38.5) | 96.5 (42) |
Thrombophilia, n (%) | ||||
Factor V Leiden | 3 (33.3) | 36 (29.3) | 4 (33.3) | 35 (29.2) |
Prothrombin 20210A mutation | 0 (0) | 11 (8.9) | 1 (8.3) | 10 (8.3) |
Protein C deficiency | 0 (0) | 3 (2.4) | 0 (0) | 3 (2.5) |
Protein S deficiency | 1 (11.1) | 5 (4.1) | 0 (0) | 6 (5.0) |
Antithrombin deficiency | 0 (0) | 3 (2.4) | 1 (8.3) | 2 (1.7) |
Hyperhomocysteinemia | 3 (33.3) | 24 (19.5) | 3 (25) | 24 (20) |
In the multivariable logistic regression model adjusted for potential confounders (age, sex, BMI, unprovoked VTE, fibrinogen and rivaroxaban concentrations), neither Ks nor CLT predicted bleeding on rivaroxaban (OR, 0.85; 95% CI, 0.4–1.8; P = 0.66 and OR, 0.98; 95% CI, 0.92–1.04; P = 0.58, respectively).
Recurrent VTE occurred in 9 patients (6.82%; 2.7% per year), including 5 patients with DVT alone and 4 with PE. All those patients belonged to the group with high rivaroxaban concentrations (n = 9, 13.43%). Patients who had recurrent VTE had unprovoked VTE more often as compared with those free of recurrent episodes (n = 8, 88.9%, vs n = 64, 52%, respectively; P = 0.03) (Table 2). Patients with a recurrent VTE episode presented with lower mean Ks (–26.7%) and prolonged CLT (+20.8%) at enrollment (Table 2).
The multivariable logistic regression model with adjustment for potential confounders such as age, sex, BMI, fibrinogen, rivaroxaban concentration, and unprovoked/provoked VTE status, showed that Ks (OR, 0.23; 95% CI, 0.06–0.94) was the only predictor of recurrent VTE in our cohort (Table 3). No predictors of bleeding were identified in our study group.
Variable | OR (95% CI) | |||
Unadjusted | P value | Adjusteda | P value | |
a Adjusted for age, sex, BMI, unprovoked VTE, fibrinogen and rivaroxaban concentration
Abbreviations: OR, odds ratio; others, see Table 1 | ||||
Ks | 0.14 (0.04–0.52) | 0.04 | 0.18 (0.04–0.78) | 0.02 |
CLT | 0.96 (0.92–1.00) | 0.92 | 0.96 (0.91–1.00) | 0.17 |
Discussion
To our knowledge, this cohort study is the first to assess fibrin clot properties as potential predictors of VTE recurrences and bleeding episodes in patients with VTE treated with DOACs. Our study demonstrates that patients on rivaroxaban who form more compact fibrin networks, which is reflected by lower plasma Ks with impaired clot lysability as evidenced by prolonged CLT, are more prone to VTE recurrence. Contrary to our expectations, we failed to observe any association between clot properties on rivaroxaban and major bleeds or clinically relevant nonmajor bleeding during follow‑up. Although there were strong correlations between rivaroxaban levels, assessed using an anti‑Xa assay, and clot features, we found that clot permeability, being a key measure of clot network density, remains a significant independent predictor of recurrent VTE during anticoagulation, also after adjustment for confounding factors, that is, age, sex, BMI, fibrinogen, rivaroxaban concentration, and unprovoked/provoked VTE status. Our findings suggest that there is a relationship between fibrin clot characteristics and subsequent thromboembolic events in patients with VTE receiving rivaroxaban, which expands the current knowledge about the role of fibrin clot structure in thromboembolism in various disease states.
The incidence of thromboembolic and bleeding episodes in our cohort during follow‑up corresponds to that reported in previous studies.32 The baseline characteristics of the patients, including the prevalence of VTE risk factors, were similar to other studies of VTE.26,33 It is likely that the present findings could refer to most patients with VTE treated with rivaroxaban.
According to available literature, several genetically determined and predominantly environmental factors that alter fibrin clot properties should be considered, including those affecting levels of coagulation and fibrinolysis proteins,and posttranslational modifications of fibrinogen.14,17 Fibrin, the product of thrombin‑mediated proteolytic cleavage of fibrinogen, provides biophysical and biochemical support to blood clots.34 It is well known that elevated thrombin concentrations lead to formation of denser fibrin networks composed of thinner fibers that are relatively resistant to plasmin‑mediated lysis.34
Direct inhibition of factor X induced by rivaroxaban and consequently decreased thrombin formation could favorably affect fibrin clot structure and susceptibility to lysis, as demonstrated previously.19,35,36We confirmed that the rivaroxaban concentration is strongly positively correlated with Ks and negatively with CLT. Importantly, our findings suggest that the modulation of fibrin clot properties by rivaroxaban cannot suppress the association of Ks with recurrent VTE, as demonstrated previously among patients with VTE who stopped anticoagulation.16,26Even if rivaroxaban improved clot properties, less favorable plasma clot characteristics on rivaroxaban, in particular compact clot networks, remained the risk factor for recurrent VTE. It might be speculated that the measurement of clot permeability during treatment with other oral anticoagulants might also have a predictive value. This hypothesis of potential clinical relevance merits further investigation.
The current study indicates that clot properties determined on rivaroxaban have no predictive value for relevant bleedings. Given varying duration of the time intervals between the last dose of rivaroxaban and blood draw as well as large interindividual differences in the drug’s concentration, a single measurement of Ks or CLT performed on anticoagulation is not helpful in identifying patients at risk for anticoagulation‑related bleeding episodes. The question remains whether the result would be different if the measurement of Ks or CLT was done off anticoagulation. It remains to be established whether Ks measured in patients with VTE off anticoagulation could be of similar significance.
Our study has several limitations. Our cohort was small and the number of the outcomes recorded was also low as expected given the efficacy and safety of rivaroxaban. Therefore, all outcome‑related findings should be interpreted with caution. Nevertheless, the association of Ks with recurrent VTE observed in VTE patients on rivaroxaban is interesting and this finding generates a new hypothesis to be tested on large cohorts in the future. Our findings cannot be easily extrapolated to elderly patients or patients with malignancies because they were excluded from the study. We cannot eliminate the possibility that some of the VTE recurrences were related to poor compliance and interruptions in anticoagulation, since the rivaroxaban concentration was not measured at the time of VTE diagnosis. Finally, it is unclear whether clot phenotype has its predictive value in patients with VTE on warfarin, although there is evidence from patients with atrial fibrillation that might support this concept.37
To conclude, we demonstrated that clot density is associated with an increased risk of VTE recurrences during treatment with rivaroxaban. None of the analyzed parameters was found to be predictive of bleeding episodes in anticoagulated patients with VTE. This study might suggest that clot permeability may be useful in identifying a subset of patients with VTE at high risk of thromboembolic episodes despite therapy with rivaroxaban, who could have been candidates for other medications or dosing regimens in long‑term secondary prevention. Future larger studies are warranted to validate this hypothesis.
- Cohen AT, Lip GY, De Caterina R, et al. State of play and future direction with NOACs: an expert consensus. Vascul Pharmacol. 2018; 106: 9‑21. | Crossref
- van Es N, Coppens M, Schulman S, et al. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: evidence from phase 3 trials. Blood. 2014; 124: 1968‑1975. | Crossref
- Prandoni P, Noventa F, Ghirarduzzi A, et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica. 2007; 92: 199‑205. | Crossref
- Heit JA. Predicting the risk of venous thromboembolism recurrence. Am J Hematol. 2012; 27: 63‑67. | Crossref
- Iorio A, Kearon C, Filippucci E, et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Arch Intern Med. 2010; 170: 1710‑1716. | Crossref
ARTICLE INFORMATION