Prevalence of coronary artery disease (CAD) among patients with aortic abdominal aneurysms (AAAs) ranges between 40% and 60%.1 A correlation between CAD severity and AAA prevalence has also been observed. The prevalence of AAA in patients with 3‑vessel disease is substantially higher than in general population.2 Coronary artery disease is an important risk factor for early mortality after aneurysm repair.3,4 We present a case of a ruptured abdominal aneurysm mimicking acute coronary syndrome in a middle‑aged patient with 3‑vessel disease.
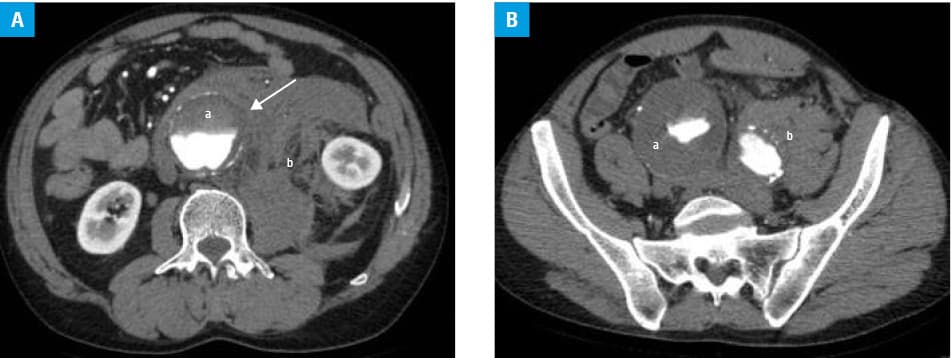
A 55‑year‑old man with a suspicion of acute myocardial infarction (AMI) was admitted to the emergency department. Due to symptoms indicative of acute coronary syndrome, the patient was pretreated with 300 mg of oral clopidogrel during transportation to the hospital. He presented with sweating as well as acute retrosternal and upper abdominal pain, among other symptoms. Examination at admission revealed a blood pressure of 70/50 mm Hg and a regular heart rate of 76 bpm. Physical examination of the abdomen was unremarkable (no rebound tenderness or abdominal guarding). Acute coronary syndrome was suspected at that point based on patient’s age, 2‑year history of 3‑vessel disease eligible for coronary artery bypass grafting, and current symptoms. Electrocardiogram and chest X‑ray were unremarkable. Relevant laboratory tests did not confirm AMI (creatine kinase, 23 U/l, creatine kinase muscle‑brain fraction, 12.1 U/l, troponin I, 0.004 ng/ml) and revealed only slight macrocytic anemia (red blood cells, 3.97 × 106/μl; hemoglobin, 12.7 g/dl; hematocrit, 39.2%; mean corpuscular volume, 98.7 fl). Abdominal ultrasound indicated abdominal aortic dilation of approximately 46 mm with concentric perimural thrombus, which prompted further imaging examinations. Computed tomography angiography depicted infrarenal AAA with bilateral iliac involvement, namely, the largest aneurysmal dilation of 61 mm located within the right common iliac artery, and signs of blood extravasation (Figure 1A–1D).
The patient was referred for emergency endovascular repair due to severe cardiac comorbidity. He was treated under general anesthesia with a successful implantation of a branched stent‑graft (Zenith, Cook Medical, Bloomington, Indiana, United States) to the infrarenal abdominal aorta and both iliac arteries. Temporary inflation of the latex balloon in the infrarenal aortic segment was used to prevent excessive blood loss during the procedure. The patient developed typical symptoms of myocardial ischemia the day after procedure. Due to elevated serum markers of myocardial infarction (troponin I, 0.245 ng/ml), he was transferred to an intensive cardiology unit and underwent coronary angiography, based on which he was again referred for cardiac surgery. The patient underwent urgent coronary artery bypass grafting. He was discharged after 8 days in good clinical condition. Follow‑up computed tomography angiography at 3 months (Figure 1E) confirmed effective endovascular repair of the abdominal aorta and both iliac arteries, with no signs of endoleaks.
Our case shows that one should stay alert and consider the possibility of other serious etiologies despite a relatively young age, typical history, and clinical symptoms suggestive of AMI in a patient.
- Hirose K, Chikamori T, Hida S, et al. Prevalence of coronary heart disease in patients with aortic aneurysm and/or peripheral artery disease. Am J Cardiol. 2009; 103: 1215‑1220. | Crossref
- Durieux R, Van Damme H, Labropoulos N, et al. High prevalence of abdominal aortic aneurysm in patients with three‑vessel coronary artery disease. Eur J Vasc Endovasc Surg. 2014; 47: 273‑278. | Crossref
- Kieffer E, Chiche L, Godet G, et al. Type IV thoracoabdominal aneurysm repair: predictors of postoperative mortality, spinal cord injury, and acute intestinal ischemia. Ann Vasc Surg. 2008; 22: 822‑828. | Crossref
- Kieffer E, Chiche L, Baron JF, et al. Coronary and carotid artery disease in patients with degenerative aneurysm of the descending thoracic or thoracoabdominal aorta: prevalence and impact on operative mortality. Ann Vasc Surg. 2002; 16: 679‑684. | Crossref
ARTICLE INFORMATION