Gastroesophageal reflux disease and Barrett esophagus: an overview of evidence-based guidelines
Key words: Barrett esophagus, cancer, chemoprevention, mortality, prevention



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Gastroesophageal reflux disease and Barrett esophagus: an overview of evidence-based guidelines
Gastroesophageal reflux disease is an extremely common condition worldwide, with the published prevalence rates varying from 2.5% in China to 51.2% in Greece. Its economic and morbidity burden is vast, and optimizing care for this condition carries huge financial and patient‑related benefits. The disease can be complicated by progression to Barrett esophagus (BE), a precancerous condition that affects approximately 2% of the population and remains undiagnosed in many individuals. The National Institute of Clinical Excellence has produced guidelines on cost‑effective management of gastroesophageal reflux disease in patients in the United Kingdom, and the Benign Barrett’s and Cancer Taskforce consensus was the largest international review of evidence known on the management of benign BE complications. This paper is a review of these guidelines with updates on new evidence. Areas for future development involve risk‑stratifying patients to surveillance, chemoprevention agents, and genetic biomarkers to help decide who will be at highest risk of malignant progression. Evidence supports the safety of proton pump inhibitors for symptom control in the medium term (ie, 9 years) and reducing the risk of progression of BE, while surgical options are cost‑effective treatments for certain patients. Barrett esophagus surveillance should be directed towards high‑risk groups, while those at lower risk may benefit from chemoprevention strategies.
Introduction
Gastroesophageal reflux disease (GERD) is a common phenomenon, affecting patients throughout their lives.1 It covers a spectrum ranging from infrequent irritating symptoms to a debilitating syndrome and can lead to the formation of a premalignant condition, Barrett esophagus (BE). GERD carries both a huge burden of morbidity and a financial burden through loss of functional working days or directly to healthcare.2-4 Add to that the potential mortality through development of esophageal adenocarcinoma (EAC) via BE,5 and this spectrum of disease requires significant investment from both primary and secondary healthcare.6,7 To address this, the National Institute of Clinical Excellence (NICE)8 produced a comprehensive guideline for the management of GERD, and there has been a thorough international consensus for the management of premalignant esophageal disease from the Benign Barrett’s and Cancer Taskforce (BoBCAT)9 – also endorsed by NICE. This paper serves to summarize the evidence from these guidelines and give an overview of current important updates in this field. The 2 guidelines reviewed in this article have been chosen as other guidelines did not reach a sufficient standard according to criteria for assessing systematic reviews.10
Gastroesophageal reflux disease
GERD is a common condition worldwide4 which presents with a range of symptoms, but is typically characterized by upper abdominal pain, heartburn, acid reflux, or vomiting. Though the NICE guideline attests there is no recognized universal diagnosis, they cite a broad consensus from the 1988 Working Party11 classification, supported by the British Society of Gastroenterology (BSG)12 1996 definition, to class GERD as any symptom conferrable to the upper gastrointestinal (GI) tract which has been present for at least 4 weeks.
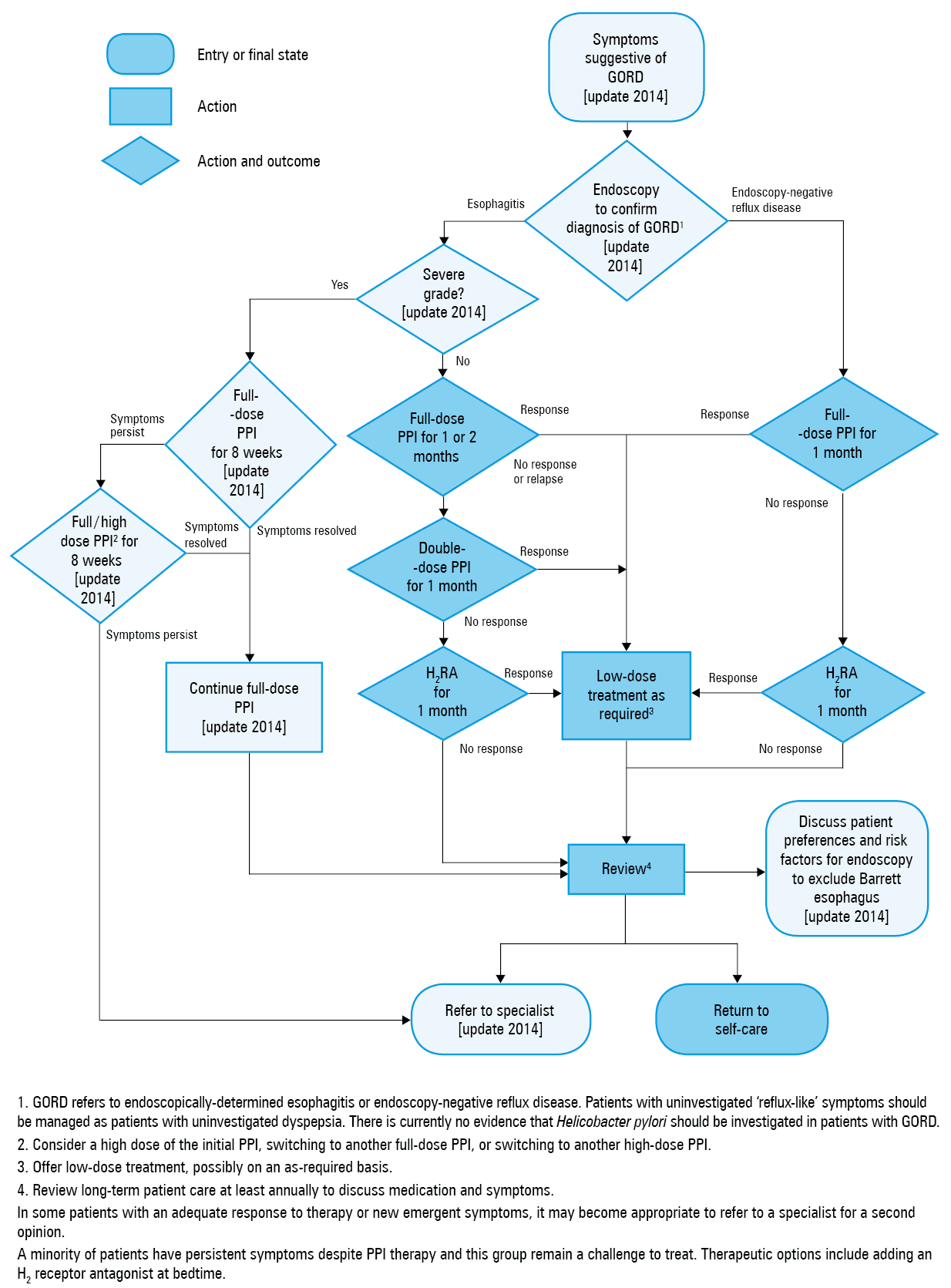
Many conditions can give the sensation of what patients describe as “heartburn” or “reflux,” but they do not actually involve true acid reflux. The differential diagnosis for this symptom includes true acid reflux, esophageal motility problems such as achalasia or jackhammer esophagus, functional esophageal discomfort, and even cardiac angina.13 Moreover, actual gastroesophageal reflux can present insidiously with rhinitis, asthma, cough, hoarseness of voice, and asymptomatically.14 The initial diagnosis of reflux can be complicated by atypical presentations, hence vigilance is key to suspect it, and the diagnosis can then be supported by response to a trial of treatment and subsequently further investigations (Figure 1).8 This will include an upper GI endoscopic evaluation and less commonly esophageal pH and manometry studies. As these investigations are invasive, the first step is a clinical diagnosis, then empirical treatment with proton pump inhibitor (PPI) alongside lifestyle modification by the patient.
Lifestyle modification
GERD has a number of specific triggers or risk factors which can be modified by the patient,15 and this can improve his or her perceived symptoms.16 The NICE guideline reviewed evidence from various studies. Randomized controlled trials were lacking; however, retrospective cohort studies showed associations and a few of the significant ones are listed here. Most of the studies reported odds ratios (ORs) of less than 2, hence no strong association: obesity (a study of 12 349 patients with body mass index [BMI] >28.2 kg/m2: OR, 1.93, 95% CI, 1.49–2.5217; and another study of 1524 patients with BMI >30 kg/m2: OR, 2.8; 95% CI, 1.7–4.5),18 smoking (7015 ever‑smokers: OR, 2.46; 95% CI, 1.89–3.1919; 1676 current smokers: OR, 1.69, 95% CI, 1.27–2.26),20 alcohol (1524 patients >6 drinks per week: OR, 1.9; 95% CI, 1.1–3.3),18 esophagitis (7015 patients, any alcohol: OR, 1.87; 95% CI, 1.44–2.43),19 coffee (no positive or protective association). There was a paucity of data for eating late at night, lying flat, chocolate, and fatty foods. In summary, individual changes generally had low to modest effects on symptoms, and there are few studies assessing these interventions on long‑term outcomes.
There was some evidence showing that weight reduction improves symptoms, with maximal benefit when reaching normal BMI.21 It also helps with many other medical comorbidities such as diabetes, hypertension, and ischemic heart disease. There was also evidence to suggest that increased visceral fat causes increased adipose tissue around the lower esophageal sphincter in obese patients that weakens the sphincter’s action.22
Educational materials can be extremely useful but such materials vary depending on the patient’s background, language, and culture. Finding well‑researched information useful to a patient can be difficult and take a long time. Likewise, many patients will be distressed by the burden of their symptoms, which may cause them to seek bad health behaviors, such as increased smoking or alcohol intake, thus compounding their condition. In a systematic review of studies looking at health‑related quality of life in relation to GERD symptoms, Becher et al23 found those with persistent symptoms had worse scores in both physical and mental health related quality of life scores, hence careful and sensitive exploration of this is important.
Proton pump inhibitors
The main principle of proton pump inhibitor (PPI) use for GERD is to use the lowest effective dose for a short period of time.24 Rates of failure to respond to PPIs have been estimated between 17% to 32% in primary care settings in a systematic review25 and 26% to 44% in secondary care in a Cochrane review.26 As with all refractory conditions, initial confirmation of compliance with PPIs is important because rates of compliance of 44% to 56% have been reported in those with refractory symptoms as compared with 84% in those with adequate symptom control.27
PPIs are overall extremely safe with few side effects and interactions.28 There have been multiple studies, many of them retrospective cohort studies, which have shown links between PPI use and several conditions. Their use was connected with an increased risk of Clostridioides (formerly Clostridium) difficile infection,29 pneumonia,30,32 dementia as well as myocardial infarction,32 chronic kidney disease,33 and fractures.34 A common limitation of large retrospective cohort studies is that associations are often overstated as causation. Therefore, careful consideration of the literature is important in the case of PPIs which have been found safe in multiple randomized controlled trials. Recent data from the AsPECT (Aspirin and Esomeprazole in Barrett Esophagus) trial, a randomized controlled trial looking at long‑term high‑dose PPI to prevent BE progression to EAC, showed no increase in adverse events.35 In the trial, 2557 patients with BE were randomized to a high‑dose PPI or low‑dose PPI with or without aspirin for a 10 year period. Only 13 serious adverse events (graded 3–5 on Common Terminology Criteria for Adverse Events) were deemed attributable to PPI, and, overall, the amount of serious adverse treatment‑related events was less than 1%.
NICE acknowledges there is some association between PPI and fractures36 and with C. difficile infection.37 Therefore, they should be used with caution in those at risk of osteoporosis, and bone density scans should be considered if a PPI is administered long term. Moreover, continuing to prescribe a drug in the absence of improvements contributes to polypharmacy and poor drug adherence.38 The take‑home message is that for GERD they should be administered in the lowest dose for the shortest period possible, but for conditions for which a long‑term administration of PPI is necessary, such as BE, they are very safe.
Identification of the spectrum of functional and organic reflux disease
Before considering endoscopy, there are other etiologies of discomfort to rule out. If a patient presents with any suggestion of GI bleeding, endoscopy transcends the importance of all other investigations in that situation. Aside from that scenario, other things are important to consider prior to escalating to endoscopic investigation. Commonly, the group presenting with symptoms will be middle‑aged or elderly patients and those who often have multiple medical comorbidities.27 Cardiac disease is important to rule out in these patients because indigestion can be a common interpretation of the heavy retrosternal discomfort that patients experience. Moreover, those who present with atypical chest pain have been shown to have worse outcomes with acute coronary syndromes.39,40 Women in particular can have atypical chest pain, radiation to the neck or jaw, which may easily mimic the tract of the esophagus/pharynx for both patients and clinicians.41,42 If there is an exertional relationship with the onset of discomfort, this may suggest a cardiac cause, but a careful consideration of the demographics, risk factors, and age of the patient may offer some stratification. If it is suspected, ruling out inconspicuous cardiac disease first may be the safest option prior to further GI investigation.
Many medications used in the treatment of other conditions can compound reflux symptoms. Nonsteroidal anti‑inflammatory drugs and steroids are particularly irritant to the upper GI tract and may need to be considered as culprits, and either reduced or stopped where possible. A recent meta‑analysis of global trends in GERD showed an OR of 1.44 (95% CI, 1.10–1.88) in patients using nonsteroidal anti‑inflammatory drugs or aspirin.43 Another important consideration is biliary disease. If a patient reports an association with fatty foods or more right‑sided pain, an ultrasound of the abdomen should be requested.
If the symptom burden is high for reflux and alternative diagnoses have been considered, then endoscopy is the next step. Findings at endoscopy can vary and do not always correlate to the severity of the symptoms. The Los Angeles Grade Classification of Erosive Esophagitis is a tried and tested system, appreciated for its diagnostic accuracy and reproducibility.44 It is a graded description of stages of esophageal mucosal damage from small areas of erosion to full circumference ulceration in grade D. As well as quantifying the amount of reflux damage, endoscopy allows for screening for associated complications, namely, BE but also esophageal cancer. Initially, assessment for BE may be difficult in the presence of inflammation, hence, if it is suspected, reflux is treated with a high‑dose PPI and the patient is brought back for reassessment. The management of suspected BE will be discussed later.
There is an important distinction to make in patients with GERD regarding the relationship between symptoms and level of inflammation on endoscopy and there are 3 phenotypes.16 In the first phenotype, there is a good correlation between the severity of symptoms with the visualized mucosal abnormality or grade on endoscopic assessment. In the second, which could be termed hypersensitive esophagus, the patient reports very significant symptoms; however, the actual evidence of mucosal damage is low at endoscopy. These patients will often have a poor response to PPI management as it is likely that there is underlying upper GI visceral hypersensitivity, which is contributing to their experience.38 To help mediate this element of their symptoms, alternative modes of therapy can be selective serotonin reuptake inhibitors or tricyclic antidepressants. The group of patients who have no reflux but who experience functional esophageal pain and esophageal motility problems is beyond the scope of this paper, all of which may mimic reflux symptoms, the key here is they are unlikely to respond to PPI therapy, and therefore need alternative treatments. Diagnosis with esophageal pH and high resolution manometry can distinguish these from true GERD.45-47 The third phenotype, insensitive esophagus, comprises patients who have very minimal symptom burden but very significant mucosal damage at endoscopy, and asymptomatic individuals have been shown to have established BE.48 Unfortunately, compliance with medications is poor because of lack of symptoms and therefore the risk of progression to dysplasia may go unchecked. Hence, these patients require quality counselling to optimize engagement with medication, and if they do progress to BE, with surveillance.
Surgical management
There is clear advice from NICE regarding patients who should be referred for laparoscopic fundoplication. The 3 main groups are individuals who are responding to PPIs but do not want to stay on long‑term treatment because of fear of complications, people who respond to PPIs who already have complications or side effects, and those who have definitive evidence on pH studies that they have severe disease that is only partially managed by the PPIs. pH and manometry studies are vital prior to referral. This is to confirm the symptoms and inflammation are related to true acid reflux but also to confirm the patient has working esophageal motility because once the fundoplication is in situ, the patient will require the functioning peristalsis of the esophagus to avoid dysphagia.
In the 2014 guideline, NICE reviewed the evidence for laparoscopic fundoplication over continued PPI use. In 6 studies, which all were randomized controlled studies of patients with GERD confirmed by endoscopic or pH studies, outcomes for health‑related quality of life favored laparoscopic fundoplication over continued PPI.49-54 They looked at 1‑year and 5‑year outcomes and found a significant improvement for all the studies in symptoms, including GERD‑related symptoms, as well as general wellbeing. Only 1 group looked at mortality and found no cases,52,53 but pooled data from 5 studies showed 15 serious adverse events (out of 337 patients) in the laparoscopic fundoplication arm as compared with none in the PPI arm.49,50,52-54 Cost analysis was performed based on data reviewed from the REFLUX (Effectiveness and Cost‑effectiveness of Minimal Access Surgery Amongst People with Gastro‑oesophageal Reflux Disease) trial. It was a large, 21‑center trial from the United Kingdom looking at surgical management as compared with medical management of GERD.55,56 Overall laparoscopic fundoplication had a greater cost at outset but had lower costs over time compared with medical management; however, patients need to be properly counselled regarding the risks associated with Nissen fundoplication, which is essentially performed in a non–life‑threatening condition. Fundoplication carries a mortality risk of approximately 0.45% within the first month,57,58 the risk of perioperative complications such as esophageal perforation or postoperative dysphagia was 1.8% to 10.8%, and there was only a 67% cure rate (in longer studies >7 years).59
Summary
In summary, there is a clear algorithm set out by NICE for the diagnosis, investigation, and management of GERD. Take‑home messages are as follows: a) lifestyle advice takes time and multiple interactions and requires sensitivity, particularly when discussing weight reduction; b) GERD symptoms can be atypical and other conditions may mimic heartburn; c) a clinician must be vigilant to complications of GERD, particularly BE; d) endoscopic findings may not correlate well with symptom burden, which can cause marked impacts on quality of life; e) pH and manometry studies must be performed prior to consideration of surgery; f) laparoscopic Nissen fundoplication and PPI are superior to other endoscopic/surgical techniques, but the surgery carries risks.
Barrett esophagus and the Benign Barrett’s and Cancer Taskforce
This section of the paper will focus on BE. Although the NICE guideline offers some advice regarding decisions on surveillance and management, a structured international consensus for the management of benign BE conditions was created in 2015 and was entitled “BOB CAT: a large‑scale review and Delphi consensus for management of Barrett esophagus with no dysplasia, indefinite for, or low‑grade dysplasia”.9 This was a process of creating an international multicenter systematic review of the evidence around the management of these conditions and the largest gathering of expert opinion for BE. Using a Delphi process, which is a validated tool to decide on group consensus where questionnaires are completed by individuals separately and the group decisions are then returned to individuals to avoid unbalanced group dynamics and individual dominance.60 During the process, consensus statements were created regarding the management of BE, and were discussed and judged for their importance and evidence using the Grading of Recommendations Assessment, Development, and Evaluation system. This system is a process of reviewing, condensing the evidence around a specific question where all important outcomes have been made explicit, then tables of evidence are produced with a rating for the strength of evidence around that question.61 It remains one of the largest systematic evidence‑based reviews in medicine to this day.
During this process an international consensus regarding the definition of BE was created:
“BE is defined by the presence of columnar mucosa in the esophagus and it should be stated whether intestinal metaplasia (IM) is present above the gastroesophageal junction.”9
It was deemed appropriate to not make IM conditional of the definition given the differences between British and American guidelines,25,26 as well as because of the evidence that suggests sampling error in missing IM and that not all EAC is preceded by the presence of IM.63 The NICE guidelines advise to take at least 8 biopsy samples at random to increase the yield of IM, more precisely, 4 biopsies per 1 cm of abnormal mucosa over the first cm should be taken in short segments. For surveillance, this has been expanded into the Seattle protocol in which quadrant biopsies are taken every 2 cm of BE in nondysplastic patients and every 1 cm in those with prior dysplasia in order to maximize the yield.64,65 As regards the NICE guidelines, if a mosaic of metaplasia is present, then it is considered BE, which is supported by consensus statements.
The prevalence of BE has been difficult to formally calculate given that it is often asymptomatic; however, in BoBCAT, using an epidemiological paper from 2005, it was estimated to be approximately 2%.66 Studies have looked at the prevalence found at endoscopy, which could have selection bias since it involves a saturated population of symptomatic patients with GERD. To overcome this, a study in the United States in which patients undergoing surveillance colonoscopy had an upper GI endoscopy, showed a prevalence of 6.8% for BE in asymptomatic patients.67 In a review of 51 studies mostly from East Asia showed an endoscopically diagnosed BE rate of 7.8% with histological diagnoses confirmed in 1.3% of patients.68 The variation in BE prevalence is unsurprising because there is a large variation in the prevalence of its precursor, GERD. A recent meta‑analysis of GERD around the world showed a range of prevalence from 2.5% in China to 51.2% in Greece.43
BE is a consequence of genetic predisposition and reflux injury causing changes to the columnar epithelium of the esophagus.5,22 Predominantly a disease of middle aged men, its frequency is increasing, particularly with the spread of the so called westernized diet.5 Risk factors associated with BE include chronic GERD, advancing age (over 50), smoking, male gender,69 white race, and particularly central obesity.70 The overall risk of progression of nondysplastic BE to EAC is approximately 0.2% to 0.5% per year,71 which is low; however, it has been deemed comparable to the risk of progression to breast cancer for carriers of BRCA1 or BRCA2 genes.72,73 The risk increases when low‑grade dysplasia (LGD) occurs and increases even further with high‑grade dysplasia (HGD).72 However, the overall risk is low, and these patients are often middle to older ages with obesity and metabolic syndrome and 90% of them will die of another condition.74 This message is often not clearly translated to patients and many live in fear of developing cancer, which is disproportionate to their actual risk.75 Surveillance programs have been widely adopted in spite of little research evidence to support this – the first randomized controlled trial investigating surveillance‑based approach as compared with patient‑reported symptom‑based approach is ongoing and known as the BOSS (BE Surveillance Versus Endoscopy at Need) study.76 Surveillance is costly to the health service but also physically and psychologically aggravating to patients, who have to go through regular invasive procedures alongside the worry of cancer. Therefore, BoBCAT did not support population screening for BE, or standard surveillance for nondysplastic BE to reduce mortality.9 Further research is ongoing into minimally invasive cell sampling techniques for population screening, such as cytosponge, including a large cluster randomization study which is currently underway within primary care units in the United Kingdom.77
Until better patient stratification can be achieved, the most important key to a successful program is patient education and involvement. BoBCAT supported the idea that when surveillance is undertaken, it should be targeted at higher risk groups (84% agreement). Moreover, it should be performed with high‑resolution endoscopy by an experienced physician (89% agreement), this was supported by a recent research priority setting exercise, in which clinicians and patients voted assessing the effectiveness of a dedicated Barrett eosphagus service as fourth out of the top 10 key research priorities.78 Allowing patients to have a clear understanding of the actual risk and the benefits and risks of BE surveillance empowers them to engage or disengage. Some of the risk factors described above can help a clinician explain an individual’s risk of progression with more accuracy, but the reality of a regular endoscopy should be clearly explained, and a clinician needs to be wary of their ability to bias a patient’s decision to engage or not. A key part of the education must be to encourage patients to contact if they are concerned about symptoms between surveillance endoscopies.
At the time of BoBCAT there was limited evidence for surveillance intervals for LGD (89% agreement). Since then, the BSG guideline had to introduce an update after the 2013 guideline following a randomized controlled trial published in the Journal of American Medical Association that looked at surveillance as compared with radiofrequency ablation (RFA) in LGD.79 The study showed a reduced risk of progression to HGD of 25% in the RFA group, and of 7.4% in EAC group. Given the significance of the findings, the study was terminated early and the BSG guideline was changed to recommend RFA in patients with confirmed LGD.80 The BSG guideline group have emphasized the importance of 2 experienced pathologists confirming the diagnosis of LGD, which was also a recommendation in BoBCAT as part of a statement around surveillance intervals for LGD (88% agreement), and that patients should be considered for ablative therapy if they are high risk and LGD is found on 2 occasions (89% agreement).
For visible lesions in patients with LGD, there was a consensus that these should be removed by endoscopic resection to aid histological diagnosis (94.7%) and that there was a strong recommendation for RFA if HGD or cancer was found. This was based on little evidence that directly indicated that visible lesions in LGD should be removed, but based on experience, such lesions often contain HGD or EAC in situ. Lesions should be defined with the Paris classification81 of lesions, as polypoidal or depressed lesions IIc/IIb most commonly have dysplasia or EAC, and in a retrospective study, histology from endoscopic resection samples changed the diagnosis in 49% of cases.82
Barrett esophagus and genetics
To further stratify patients according to risk, research into genetic biomarkers for BE has been gaining ground in the last few decades, more precisely, since the human genome project. What reflected this, were 2 statements in BoBCAT that highlighted growing emphasis on aberrant p16, p16 methylation, or p16 loss being associated with progression from nondysplastic BE to LGD (80% agreement), and overexpression of p53 as a risk factor for progression to dysplasia (87% agreement). Wang et al83 compared findings from biopsies taken from patients with BE, LGD, HGD, EAC, and healthy controls, also looking at the presence of hypermethylation of p16 and APC genes. They found that none of the normal control samples showed the presence of promoter hypermethylation of these genes, whereas there was significant presence in nondysplastic BE (31%), LGD BE (50%), HGD (54%), and EAC (68%). The same group found higher prevalence of DNA methylation in those who had undergone RFA and showed evidence of residual BE with or without LGD, suggesting a need to monitor this group more closely postintervention to predict progression to HGD.84 Other areas of study include HPP1, RUNX3, AKAP12, CDH13, SST, TAC1, and NELL1 and their aberrant methylation.85,86
For p53, though, the following statement was endorsed at 87.7% agreement: “Aberrant p53, p53 mutation, or p53 loss in nondysplastic BE is associated with an increased risk of developing dysplasia.”9 Consensus could not be reached regarding the use of p53 abnormalities in clinical practice. Likewise, as regards other biomarkers, the research is not consistent enough to use these as predictive markers in routine clinical practice, and this topic awaits further evidence.
The first genome‑wide association study was published in 2013 and was performed by the Esophageal Adenocarcinoma Genetics Consortium as part of the Wellcome Trust Case Control Consortium into 15 common diseases.87 The study located 2 genetic loci of significance in EAC. On the HLA 6p21 region there was a highly significant association, which showed predominance in men (OR, 1.38; 95% CI, 1.25–1.53) as compared with women (OR, 1.11; 95% CI, 0.95–1.30). This loci also showed changes geographically, although without strong significance, but seemed to be associated with areas of higher EAC prevalence, for example, Scotland. The second locus was found at 16q24, significant for its locality near the transcription factor FOXF1, which in deletion studies on mice has been associated with multiple esophageal abnormalities.22 Further to this, a big proportion of shared genes were found in patients with BE, obesity, and cardiac disease. There is evidence of increased visceral fat in those with BE and obesity, and patients with BE have a strong predisposition to visceral fat. An overall higher mortality in these patients may be related to this link with the metabolic syndrome.88
Barrett esophagus is a multifactorial condition but future research into genetic biomarkers may help shape the way future surveillance and screening is achieved. However, at this stage clinical practice lags behind evidence. In the recent BE research priority setting exercise, finding ways to accurately identify high‑risk groups for BE screening and how we can achieve individual risk stratification of patients with BE to target surveillance were deemed priority 1 and 2, respectively.78
Chemoprevention and Barrett esophagus
Chemoprevention is the regular use of common, safe drugs or dietary supplements to prevent cancer. Aspirin and PPIs have shown promise as chemopreventive agents, fitting with the hypothesis that EAC is an inflammatory‑mediated malignant response to prolonged acid exposure. There are no laboratory data to show a cellular mechanism for PPI chemoprevention; however, some have shown that absolute acid suppression reduced cell proliferation89,90 and increased expression of cyclin dependent kinase inhibitors p21 and p16.91 Aspirin has numerous anticancer actions which have been hypothesized, namely its anti‑inflammatory actions on prostaglandin E2 via the cyclooxygenase pathway. Prostaglandin E2 has been linked to preventing apoptosis, increasing cell proliferation and migration and also stimulation of angiogenesis.92 Aspirin has been shown to reduce cellular β-catenin,93 reducing cell proliferation via platelet‑mediated thromboxane effects,94 and reducing circulating inflammatory cytokines.95
BoBCAT statement regarding chemoprevention was as follows: “The use of PPIs (compared with no therapy or histamine receptor type 2 antagonists) is associated with a decrease in progression from benign BE metaplasia to BE neoplasia (dysplasia and EAC).”9
At the time of BoBCAT this could not be endorsed and reached only 53.3% agreement because at that stage, evidence was mostly cohort or retrospective data. Since then, the results of the AspECT (Esomeprazole and Aspirin in Barrett’s Oesophagus) trial have been released and published in The Lancet.35 The AspECT trial was an international multicenter phase 3 randomized controlled trial with 10 years of follow‑up of patients with BE who received high‑dose esomeprazole (40 mg twice daily) or low‑dose (20 mg once daily) with or without aspirin. The main outcomes reviewed were rates of all‑cause mortality, EAC, and HGD.
High‑dose PPI was superior to low‑dose PPI in decreasing all‑cause mortality. It also increased length of time to events (8 vs 10.2 years) and the data were analyzed to show a time to an event ratio. Values greater than 1 showed the intervention prolonged the time to an event. Combined use of aspirin and high‑dose PPI was superior to no aspirin and low‑dose PPI and appeared to have an additive effect (time to event ratio 1.59; 95% CI, 1.14–2.23; P = 0.007).35 The numbers needed to treat were 43 for aspirin as compared with no aspirin and 34 for high‑dose PPI as compared with low‑dose PPI. Less than 1% of participants had a treatment related serious adverse event.
The study limitations were that it focused only on a fraction of the population of BE patients, the population was predominantly Caucasian, and the drug treatments were not blinded. However, data from this randomized controlled trial supports previous observational data which suggested a chemopreventive link between EAC aspirin and PPI, and metanalysis data from cardiovascular studies with aspirin which showed lower EAC rates (though these were not primary end points).96,97 The way in which the AspECT data is interpreted may be similar to the other recommendations discussed in this paper – targeting of high‑risk groups to streamline interventions is likely to be the future.
Conclusions
This paper has outlined 2 high‑quality guidelines for the management of 2 common conditions, GERD and BE. Vigilance to new evidence and research is key to ongoing good clinical practice and contradictory evidence should not always be avoided if it is robust and postdates a guideline. For GERD, PPIs are a safe medical treatment to augment lifestyle changes and research supports an emphasis on weight reduction and smoking cessation. Surgery has shown good outcomes for quality of life in certain patient groups but carries a risk of complications for which excellent counselling is paramount. We should be vigilant to alternative etiology, and if we have doubts, endoscopy and pH manometry studies can confirm the diagnosis.
BE remains a significant target for intervention as a precursor to a malignancy that carries a dismal 5‑year survival rate relative to other luminal malignancies.98 Currently, surveillance is based on spreading a wide net to intervene in certain cases, but it is not always achieved to a sufficient standard. There are specific groups for whom the need for surveillance needs to be emphasized – men, obese, smokers, with family history, and those with long segment BE – whilst randomized controlled study data for surveillance is awaited. Approaches to BE will be shaped significantly in the coming years with advances in chemoprevention, as well as early detection through minimally invasive techniques and endotherapy for dysplasia. Until then, good quality education of patients will help improve the appropriate use of surveillance, medication, and engagement in studies to address ongoing research needs.
- Alexandropoulou K, van Vlymen J, Reid F, Poullis A, Kang J‑Y. Temporal trends of Barrett’s oesophagus and gastro‑oesophageal reflux and related oesophageal cancer over a 10‑year period in England and Wales and associated proton pump inhibitor and H2RA prescriptions: a GPRD study. Eur J Gastroenterol Hepatol. 2013; 25: 15‑21.
- Peery AF, Crockett SD, Barritt AS, et al. Burden of gastrointestinal, liver, and pancreatic diseases in the United States. Gastroenterology. 2015; 149: 1731‑1741.e3.
- Gong EJ, Choi KD, Jung H‑K, et al. Quality of life, patient satisfaction, and disease burden in patients with gastroesophageal reflux disease with or without laryngopharyngeal reflux symptoms. J Gastroenterol Hepatol. 2017; 32: 1336‑1340.
- El‑Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro‑oesophageal reflux disease: a systematic review. Gut. 2014; 63: 871‑880.
- Kuipers EJ, Spaander MC. Natural history of Barrett’s esophagus. Dig Dis Sci. 2018; 63: 1997‑2004.
ARTICLE INFORMATION