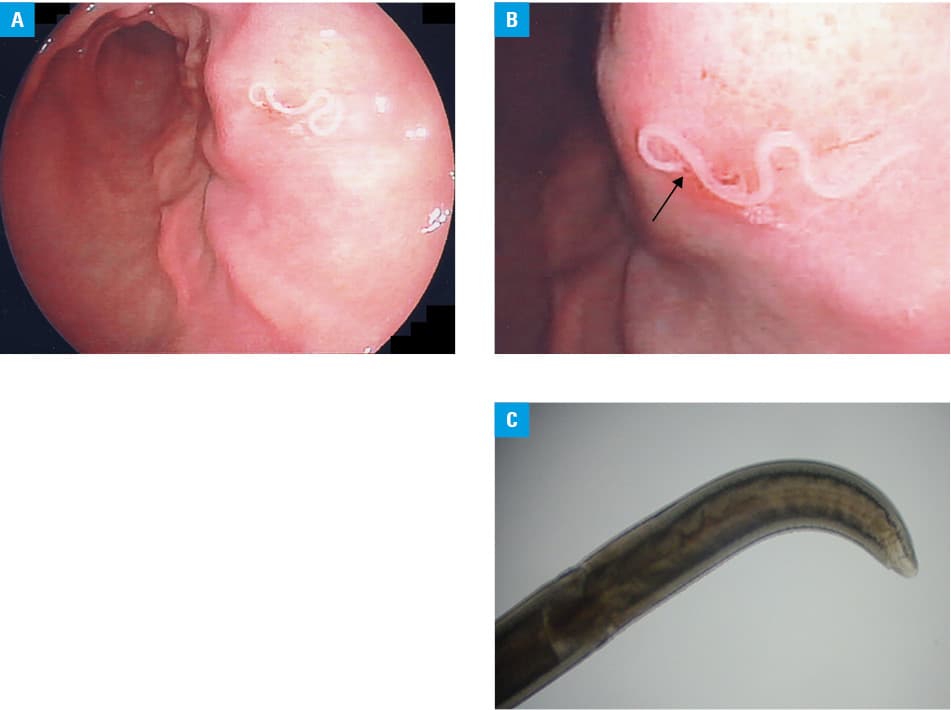
A 57‑year‑old man presented with severe epigastric pain and nausea 5 hours after eating a sushi meal (raw mackerels). Vital signs were stable, and an abdominal examination revealed abdominal tenderness without rebound in the epigastrium. As anisakidosis was suspected, the patient underwent endoscopy, which revealed a white worm penetrating the mucosa of the gastric upper body (Figure 1A). On closer observation, the white worm was biting the mucosa and was moving slowly (Figure 1B). It was removed by the biopsy forceps, after which the patient’s symptoms resolved completely. Microscopic examination confirmed an Anisakis larva (Figure 1C).
Anisakidosis is a parasitic infectious disease transmitted to humans through raw, pickled, or undercooked fish and seafood containing larvae of the nematode of the Anisakidae family.1 These larvae can be found in salmon, cod, herring, and mackerel. Most cases were reported in Japan, where sushi, a traditional dish containing raw fish, is quite popular. As eating undercooked seafood has become more popular worldwide, the number of patients with anisakidosis has been increasing globally, even in the coastal areas of Europe.2-4 Symptoms include abdominal pain, nausea, and diarrhea. This infection can lead to massive eosinophilic infiltration and formation of granulomas. Reinfection sometimes results in systemic allergic reactions, including urticaria and anaphylaxis.1,3 A history of recent consumption of raw fish followed by an acute onset of the above symptoms provides important clues for the diagnosis.4 In most acute cases, the removal of the larva by endoscopic biopsy forceps provides a definitive diagnosis. The larvae may cause chronic submucosal granulomatous nodules in the stomach, which require endoscopic submucosal resection for both diagnosis and treatment.5 Serological examination for anti–Anisakis simplex immunoglobulin E can be helpful for the diagnosis of intestinal, ectopic, and allergic disease. Although rare, intestinal and ectopic cases may require surgical removal.4 Given the growing risk of anisakidosis, the key to prophylaxis includes adequate freezing or cooking of the fish.
- Nieuwenhuizen NE. Anisakis – immunology of a foodborne parasitosis. Parasite Immunol. 2016; 38: 548‑557. | Crossref
- Chai JY, Darwin Murrell K, Lymbery AJ. Fish‑borne parasitic zoonoses: status and issues. Int J Parasitol. 2005; 35: 1233‑1254. | Crossref
- Audicana MT, Kennedy MW. Anisakis simplex: from obscure infectious worm to inducer of immune hypersensitivity. Clin Microbiol Rev. 2008; 21: 360‑379. | Crossref
- Hochberg NS, Hamer DH. Anisakidosis: perils of the deep. Clin Infect Dis. 2010; 51: 806‑812. | Crossref
- Bookhout C, Greene K. Chronic epigastric pain associated with gastric anisakidosis. IDCases. 2019; 15: e00515. | Crossref
ARTICLE INFORMATION