Long-term follow-up and comparison of techniques in radiofrequency ablation of ventricular arrhythmias originating from the aortic cusps (AVATAR Registry)
Key words: aortic cusps, complications, electroanatomical mapping, radiation exposure, ventricular arrhythmia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Long-term follow-up and comparison of techniques in radiofrequency ablation of ventricular arrhythmias originating from the aortic cusps (AVATAR Registry)
Introduction: Radiofrequency ablation (RFA) of outflow tract ventricular arrhythmia (VA) that originates from the aortic cusps can be challenging. Data on long‑term efficacy and safety as well as optimal technique after aortic cusp ablation have not previously been reported.
Objectives: This aim of the study was to determine the short- and long‑term outcomes after RFA of aortic cusp VA, and to evaluate aortic valve injuries according to echocardiographic screening.
Patients and methods: This was a prospective multicenter registry (AVATAR, Aortic Cusp Ventricular Arrhythmias: Long Term Safety and Outcome from a Multicenter Prospective Ablation Registry) study. A total of 103 patients at a mean age of 56 years (34–64) from the “Electra” Registry (2005–2017) undergoing RFA of aortic cusps VA were enrolled. The following 3 ablation techniques were used: zero‑fluoroscopy (ZF; electroanatomical mapping [EAM] without fluoroscopy), EAM with fluoroscopy, and conventional fluoroscopy‑based RFA. Data on clinical history, complications after RFA, echocardiography, and 24‑hour Holter monitoring were collected. The follow‑up was 12 months or longer.
Results: There were no major acute cardiac complications after RFA. In one case, a vascular access complication required surgery. The median (interquartile range [IQR]) procedure time was 75 minutes (IQR, 58–95), median follow‑up, 32 months (IQR, 12–70). Acute and long‑term procedural success rates were 93% and 86%, respectively. The long‑term RFA outcomes were observed in ZF technique (88%), EAM with fluoroscopy (86%), and conventional RFA (82%), without differences. During long‑term follow‑up, no abnormalities were found within the aortic root.
Conclusions: Ablation of VA within the aortic cusps is safe and effective in long‑term follow‑up. The ZF approach is feasible, although it requires greater expertise and more imaging modalities.
Introduction
Radiofrequency catheter ablation (RFA) is a safe and effective method for treating patients with idiopathic ventricular arrhythmias (IVA). Approximately 15% of IVA originate from the left ventricular outflow tract (LVOT) and can be mapped and ablated within the aortic root.1,2 However, aortic cusp catheter ablation is a challenging procedure due to the risk of aortic valve leaflet damage as well as close proximity to coronary arteries and atrioventricular conduction system.1,3 The 3‑dimensional electroanatomical mapping (3D‑EAM) system enables precise reconstruction of aortic root anatomy and tracking the catheter position during ablation, thus avoiding X‑ray exposure and coronary angiography.4 Currently, efficacy and safety data on aortic cusp ablation is limited, especially considering the procedures based on 3D‑EAM without fluoroscopy.2,4,5 Available data show that aortic cusp catheter ablation of IVA can be performed safely.1-5 Most analyses are retrospective, based on small patient samples, and not aimed directly at excluding potential aortic valve injuries. No echocardiographic studies have documented long‑term safety of RFA. Current European guidelines cautiously recommend referring patients with suspected LVOT arrhythmias only to electrophysiology centers with experienced personnel.6 Therefore, the aim of this prospective multicenter registry study was to determine acute- and long‑term outcomes and safety of aortic cusp ablation, especially ablations performed without fluoroscopy.
Patients and Methods
The study population included patients from a prospective multicenter “Electra” registry, which covered ablation procedures from 10 Polish centers. The majority of procedures (74%) were performed by 5 experienced operators only, and 26% by 5 intermediate assistants under the guidance of experts. Patients undergoing aortic cusp RFA for frequent premature ventricular complexes (PVCs) and/or ventricular tachycardia (VT) were recruited between 2005 and 2017. All ablation procedures were done in line with the current guidelines6 after failure of medical treatment or directly in patients opting out of long‑term antiarrhythmic drug therapy. IVA was diagnosed in patients without structural heart disease (SHD), based on history, typical clinical features, echocardiography, exercise stress testing, cardiac catheterization, and cardiac magnetic resonance imaging (MRI) when needed. Structural heart disease was defined as ischemic or nonischemic cardiomyopathy, history of myocardial infarction (MI), revascularization, or significant (moderate or severe) valvular disease.
Baseline data included demographic characteristics, cardiac history, procedure details, echocardiography, and 24‑hour Holter monitoring. The acute- and short‑term follow‑up was set at the time of ablation procedure and 1 month after, respectively. Long‑term follow‑up extended between September 2017 and May 2018 to ensure a 1‑year or longer observation after the last ablation. The patients were informed on follow‑up appointment schedule and were contacted to schedule echocardiography and 24‑h Holter monitoring. Clinical data on follow‑up, complications, and postablation antiarrhythmic drugs were collected. A standardized definition of major complications was used as shown in Supplementary material, Table S1.
Mapping and ablation protocol
We analyzed 3 techniques: zero‑fluoroscopy (ZF) (3D‑EAM without fluoroscopy), 3D‑EAM with fluoroscopy, and conventional fluoroscopy‑based ablation (without support of 3D‑EAM system). The choice of technique was at the discretion of the operator and was dependent on the availability of the 3D‑EAM.
Local anesthesia and light conscious sedation were used in RFA. Ablation and diagnostic catheters (4 mm, 8 mm, or irrigated gold‑tip catheters; Biotronik, Berlin, Germany or Tacticath, Abbott, St. Paul, Minnesota, United States) were introduced percutaneously via femoral access. In most cases, a standard decapolar diagnostic catheter was introduced into the coronary sinus or the right ventricle under fluoroscopic guidance or using the 3D‑EAM system (Ensite Velocity NavX, St Jude Medical, St. Paul, Minnesota, United States) with near zero–fluoroscopy or ZF. First, a programmed ventricular stimulation was conducted to assess the propensity for sustained VA. Then, in most cases, classic right ventricular outflow tract (RVOT) mapping was performed to identify the optimum ablation site according to pace and local activation mapping. If no adequate RVOT sites were identified or if RFA in RVOT was unsuccessful, the mapping was extended to the LVOT. Left ventricular outflow tract sites were mapped via a retrograde aortic approach. If LVOT mapping was insufficient, a mapping catheter was inserted through distal coronary sinus, in order to validate the signals from the LVOT epicardial region, mapping the great cardiac vein and the left main ostium.7 In patients without spontaneous ectopy at the time of intracardiac mapping, pacing or isoproterenol infusions (or both) were used to induce PVCs or VT. The location of aortic cusps was determined with coronary angiography and angiography of the Valsalva sinuses. However, if ZF was used, the location of coronary artery ostia was identified with the use of 3D‑EAM and separate visualization of aortic cusps, location of the recording of right and left His bundle, and intracardiac signals. The position of ablation catheter tip within the aortic cusp was confirmed using several techniques (ie, inability to move further through the aortic valve and to bend catheter to the mitral annulus). The example of near zero–fluoroscopy for aortic cusp ablation is shown in Supplementary material, Figure S1. Mapping methods included simple maps with aortic cusp or aortic root contours, activation mapping with unipolar recordings, and pace mapping up to maximum pacing thresholds of 25 mA with evaluation of 12/12 pacing morphology when necessary. Radiofrequency ablation applications were set at 30W (for irrigated catheters) or 60W (for nonirrigated catheters) at 48°C to 60°C.
The acute procedural success of RFA was defined as a complete absence of spontaneous PVCs/VT for more than 15 minutes following the last application, noninducibility after isoproterenol infusion, and complete electrophysiology study using atrial incremental pacing, and ventricular and atrial programmed pacing up to 3 extra stimuli.
The origins of PVCs/VT were classified as left coronary cusp (LCC), right coronary cusp (RCC), LCC/RCC junction (LCC/RCC), noncoronary cusp (NCC), or aortomitral continuity (AMC)/LCC area, if both sites were required for successful ablation.
The origins of PVCs from epicardial left ventricular summit was suspected in each patient with unsuccessful procedure. They were offered the next procedure with epicardial access, yet none of the 3 patients who were suspected to have epicardial origin from inaccessible sites of left ventricular summit consented to subsequent procedure. Despite that, these patients were included in the study due to primary RFA performed in the LCC.
24‑hour Holter monitoring
The 24‑hour Holter monitoring was obligatory prior to ablation and was repeated after 1 month and at the final follow‑up visit in order to determine the PVC burden. Treatment success was referred to as 80% or higher postablation decrease in PVC burden. In case of recurrent arrhythmias, 12‑channel ECG Holter monitoring was performed to validate arrhythmia and determine the PVC/VT morphology.
Transthoracic echocardiography
Transthoracic echocardiogram was performed before and after ablation and was repeated after 1 month, at the final follow‑up visit, or more frequently depending on clinical need. The aim of transthoracic echocardiogram at the final visit was to exclude aortic/mitral leaflet damage and assess left ventricular ejection fraction (LVEF). MRI was scheduled in cases of suspected pathologic lesions in aortic leaflets. Aortic pathologies were classified as major (significant aortic regurgitation/stenosis, leaflet perforation) or minor (mild/moderate aortic regurgitation/stenosis, other cusp abnormalities). The specialists performed echocardiography according to relevant guidelines8 and were blinded to the aortic cusp ablation site. A baseline left ventricular ejection fraction more than 50% was consistent with suspected PVC‑induced cardiomyopathy.
Statistical methods
Categorical variables were expressed as numbers and percentages. Quantitative variables were expressed as medians and interquartile ranges (IQRs) or means (SD). The null hypothesis was verified using the Mann–Whitney test or t test. For categorical variables, the between‑group differences were determined using the χ2 or Fisher exact tests. The ablation details in respect to ablation cusp target with global P calculation were compared using the Kruskal–Wallis test. The changes of continuous variables in time were compared using the paired samples t test for normally distributed data or using the Wilcoxon signed‑rank test for data with skewed distribution. A P value of less than 0.05 was considered significant. No adjustment for multiple comparisons was made. All statistical analyses were performed using the R 3.4 bundle (R Foundation for Statistical Computing, Vienna, Austria).
Ethic
The study was conducted in accordance with the tenets of the Declaration of Helsinki. All patients provided written informed consent to participate in the study. The study protocol was approved by the local institutional ethics committee (decision number 5/4/2017).
Results
Patient population
Between 2005 and 2017, 1163 patients underwent RFA due to IVA. Of those, 120 patients (10.3%) had aortic cusp ablation. Additionally, 305 patients with SHD required RFA for VA. From the latter group, the origin of PVC/VT was located within the aortic cusp in 19 patients (6.2%; IVA vs PVC/VT in SHD; P = 0.03). Among 139 patients undergoing RFA for aortic cusp VA, 45% were women, the mean (SD) age was 49.1 (19.7) years, and the mean (SD) baseline LVEF was 59% (8.9).
Acute procedural success was achieved in 94% of patients. During the long‑term follow‑up, 6 patients died of causes unrelated to RFA. Another 30 patients were lost to follow‑up. Complete data on follow‑up were available for 103 patients whose characteristics are shown in Table 1.
Parameter | All | IVA | VA‑SHD | P value |
Abbreviations: BMI, body mass index; IQR, interquartile range; IVA, idiopathic ventricular arrhythmia; LVEF, left ventricular ejection fraction; PVC, premature ventricular complex; SHD, structural heart disease; VA, ventricular arrhythmia; VT, ventricular tachycardia | ||||
Number | 103 | 90 | 13 | – |
Age, y, median (IQR) | 56 (34–64) | 54.5 (33.2–63) | 64 (62–69) | <0.001 |
Women, % | 48.5 | 50 | 38.5 | 0.63 |
Hypertension, % | 61.2 | 56.7 | 92.3 | 0.03 |
Insulin‑dependent diabetes, % | 3.9 | 1.1 | 23.1 | 0.006 |
BMI, kg/m2, mean (SD) | 26.9 (4.9) | 26.6 (5) | 29.0 (3.7) | 0.06 |
LVEF before ablation, %, mean (SD) | 58.3 (8.5) | 59.9 (6.7) | 44.9 (11.2) | 0.004 |
PVC burden before ablation, %, median (IQR) | 20 (12–30) | 20 (12–30) | 23.0 (17.5–29.2) | 0.43 |
PVC/24 hours, median (IQR) | 19670 (11688–29904.5) | 19537 (11000–29838) | 23335 (18157–29231.2) | 0.38 |
PVC, % | 96.1 | 95.6 | 100 | 1.00 |
PVC/pairs, % | 55.3 | 53.3 | 69.2 | 0.44 |
PVC/nonsustained VT, % | 29.1 | 24.4 | 61.5 | 0.02 |
PVC/VT, % | 4.9 | 4.4 | 7.7 | 0.50 |
Number of antiarrhythmic drugs before ablation, median (IQR) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.42 |
Follow‑up duration, mo, mean (SD)/median (IQR) | 42.9 (38.2)/32 (12–70) | 44.5 (39.1)/35 (13–70) | 32.1 (30.3)/14 (12–60) | 0.2/0.37 |
Compared with patients with IVA, those with PVCs/VT in SHD were older, had more comorbidities, lower LVEF, and a tendency toward a higher body mass index. Most patients had a single PVC configuration. Patients with PVC/VT in SHD were more frequently affected by complex arrhythmias (nonsustained VT) than patients with IVA. There were no differences in the number of antiarrhythmic drugs or follow‑up duration.
Procedure details, short- and long‑term outcomes
The majority of patients had VA arising from the LCC (48%); less frequent locations were AMC/LCC (26%), LCC/RCC (11%), RCC (9%), and NCC (6%). The median procedure duration was 75 minutes (IQR, 58–95), fluoroscopy time was 5 minutes (IQR, 0–16), and the number of RFA applications was 9 (IQR, 5–15). Pacemapping was available only in a minority of cases (18%); therefore, activation mapping was mainly used. Procedure details regarding VA cusp location are shown in Table 2.
Origin | Age, y, median (IQR) | Male/female sex, % | Previous failed ablation, % | nVT or VT/ total, % | Procedure duration, min, median (IQR) | Fluoroscopy duration, min, median (IQR) | RF duration, s, median (IQR) | No. of RF aplications, median (IQR) |
Continuous variables are expressed as medians (interquartile ranges, Q1–Q3). Categorical variables are expressed as fractions (%).
a AMC/LCC vs LCC; P = 0.04; b LCC vs NCC; P = 0.02; c AMC/LCC vs NCC; P = 0.02; d AMC/LCC vs RCC; P = 0.04;
e LCC/RCC vs NCC; P = 0.04
Abbreviations: AMC, aorto‑mitral continuity; LCC, left coronary cusp; NCC, noncoronary cusp; nVT, nonsustained ventricular tachycardia; RCC, right coronary cusp; RFA, radiofrequency ablation; VT, ventricular tachycardia; others, see Table 1 | ||||||||
All, n = 103 | 56 (34–64) | 51/49 | 10 | 31 | 75 (58–95) | 5 (0–16) | 351 (191.5–590) | 9 (5–15) |
LCC, n = 50 | 54 (31.5–62.8)a | 44/56b | 8 | 30 | 75 (55–95) | 6 (0–16) | 348.5 (154.5–601) | 7.5 (4.8–15) |
AMC/LCC, n = 27 | 62 (53–65.5)a,c,d | 52/48 | 14 | 29 | 70 (56.5–90) | 4 (0–17.5) | 432 (302.5–544) | 12 (6.5–15) |
LCC/RCC, n = 11 | 63 (46.5–70) | 45/55e | 9 | 45 | 75 (62.5–79.5) | 0 (0–7) | 252 (180–858.8) | 8 (4.5–15) |
RCC, n = 9 | 55 (34–58)d | 67/33 | 22 | 22 | 120 (75–170) | 6 (0–40) | 240 (160–600) | 8 (4–20) |
NCC, n = 6 | 27 (20.8–52.8)c | 100/0b,e | 0 | 50 | 65 (60–95) | 2 (0–16) | 395 (252.5–505) | 10.5 (6.8–17.2) |
P value | 0.04 | 0.05 | 0.38 | 0.46 | 0.21 | 0.46 | 0.48 | 0.78 |
There were differences in respect to age between patients undergoing AMC/LCC ablation and those with LCC, NCC, and RCC targets. Patients with VA originating from NCC were solely men and were younger than those in the AMC/LCC group.
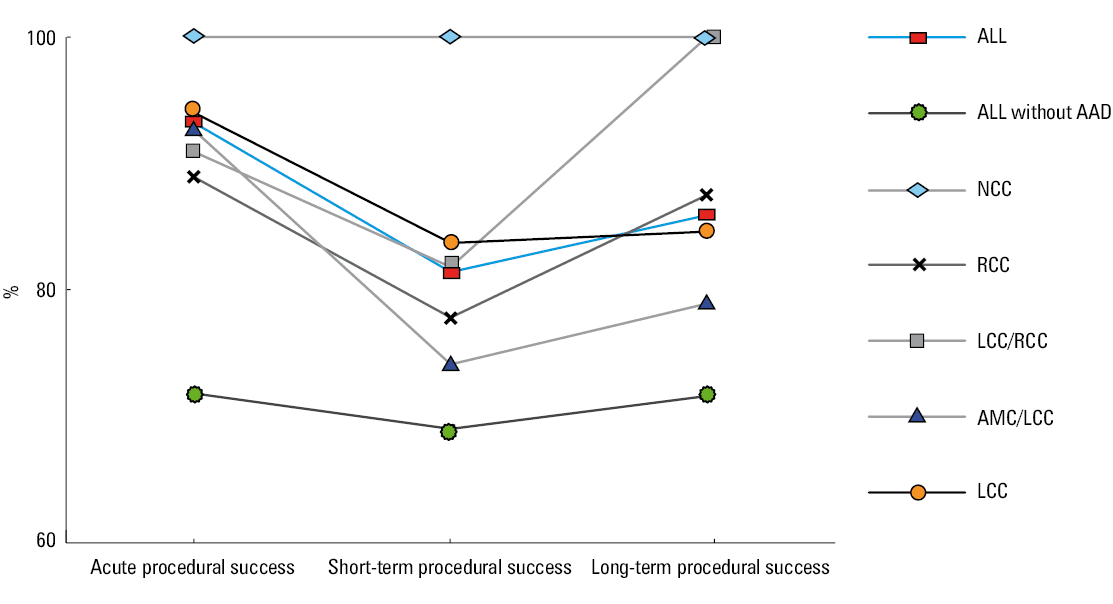
Overall, acute, short‑term, and long‑term success was achieved after a mean of 1.1 procedures in 93%, 81%, and 86% of patients, respectively. The highest ablation success rate was noted for VA arising from the NCC and the lowest was for the AMC/LCC cusp target, yet the difference was not significant (Figure 1). During the follow‑up, 8% patients underwent second ablation procedure and 3% required third ablation due to VA recurrence or procedural failure.
The ablation success was not SHD‑dependent and was comparable in the IVA and SHD groups. The success rates for acute, short- and long‑term follow‑up were 92%, 81%, and 87%, respectively in the IVA group and 100%, 85%, and 80%, respectively in the SHD group.
The total number of PVCs recorded on 24‑hour Holter monitoring decreased significantly from baseline to the long‑term follow‑up from 19670 (IQR, 11688–29907) to 96 (1–1566) (P <0.001) in the entire sample. There were no differences in degree of PVCs reduction with respect to IVA or SHD presence and aortic cusp location.
There were no differences between the patients with long‑term treatment success and those with treatment failure in all parameters but the left atrium size at baseline, which was significantly larger in the latter group (38 mm vs 44 mm, respectively, P = 0.006).
Ablation technique and procedure success
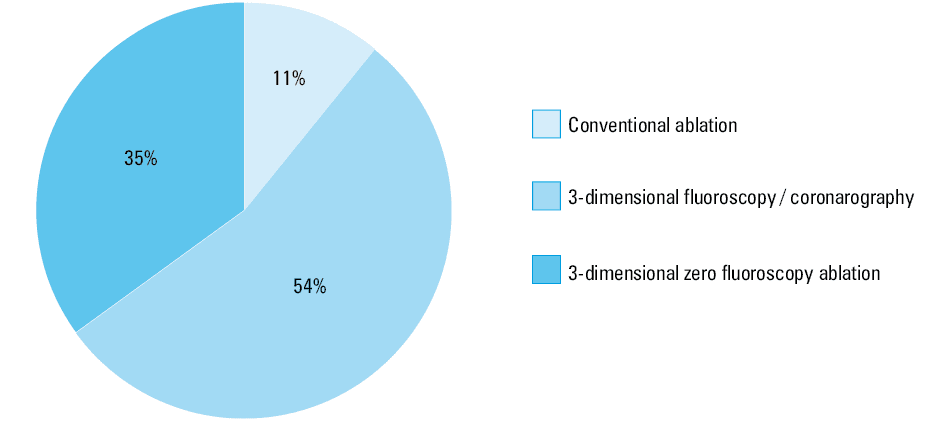
There were no differences in clinical characteristics between the 3 compared techniques (Table 3). The most commonly used ablation technique was 3D‑EAM with fluoroscopy (56 patients) (Figure 2). The ZF was used in 35% of all procedures in the registry (36 patients), with increasing preference in recent years. The least common ablation method was conventional ablation without 3D‑EAM (11 patients).
All | Conventional ablation | 3D‑EAM + F | 3D‑EAM + ZF | P value | |
a Conventional ablation vs 3D‑EAM + ZF; P <0.001 b Conventional ablation vs 3D‑EAM + F; P = 0.04 c 3D‑EAM + F vs 3D‑EAM + ZF; P <0.001
Abbreviations: 3D‑EAM, 3‑dimensional electroanatomical mapping; BMI, body mass index; F, fluoroscopy; ZF, zero fluoroscopy; others, see Table 1 | |||||
Age, y, median (IQR) | 56 (34–64) | 45 (40.5–61.5) | 57 (32.5–63) | 59 (42.2–68) | 0.32 |
Women, % | 48.5 | 36.4 | 50 | 50 | 0.69 |
Hypertension, % | 61.2 | 63.6 | 53.6 | 72.2 | 0.19 |
Insulin‑dependent diabetes, % | 3.9 | 0 | 5.4 | 2.8 | 1.00 |
BMI, kg/m2, median (IQR) | 26 (23; 31) | 25 (23.2–26.8) | 26.5 (23–32) | 26 (24–28.2) | 0.74 |
Fluoroscopy duration, min, median (IQR) | 5 (0–16) | 17.5a,b (15.5–20.2) | 9.5b,c (5–19) | 0a,c (0–0) | <0.001 |
Short‑term treatment success, % | 81 | 73 | 80 | 86 | 0.72 |
Long‑term treatment success, % | 86 | 82 | 86 | 88 | 0.84 |
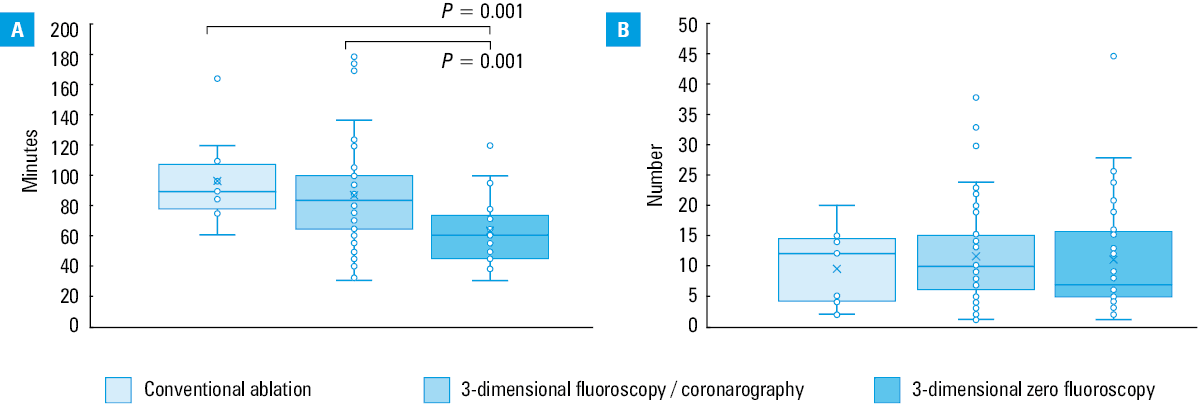
The procedure duration was the shortest with the ZF method (median, 60.0 minutes; IQR, 45.0–73.5; P <0.001), which showed a trend towards the lowest number of RFA applications as compared with the conventional and 3‑dimensional fluoroscopy/coronary angiography techniques (Figure 3). The fluoroscopy duration was the longest for conventional ablation as compared with both 3D‑EAM approaches (Table 3). The short- and long‑term success rates were the highest with ZF (86% and 88%, respectively), although the difference between ZF and other techniques was not significant (Table 3). The conventional ablation was associated with the lowest success rate (nonsignificant) and the longest duration as compared with 3D‑EAM (significant difference as compared with ZF).
Complications
Postablation echocardiography findings
No major pathologies in the aortic or mitral leaflets and aortic root were observed (Figure 4). No moderate/significant aortic stenosis/regurgitation or leaflet perforations were observed after ablation.
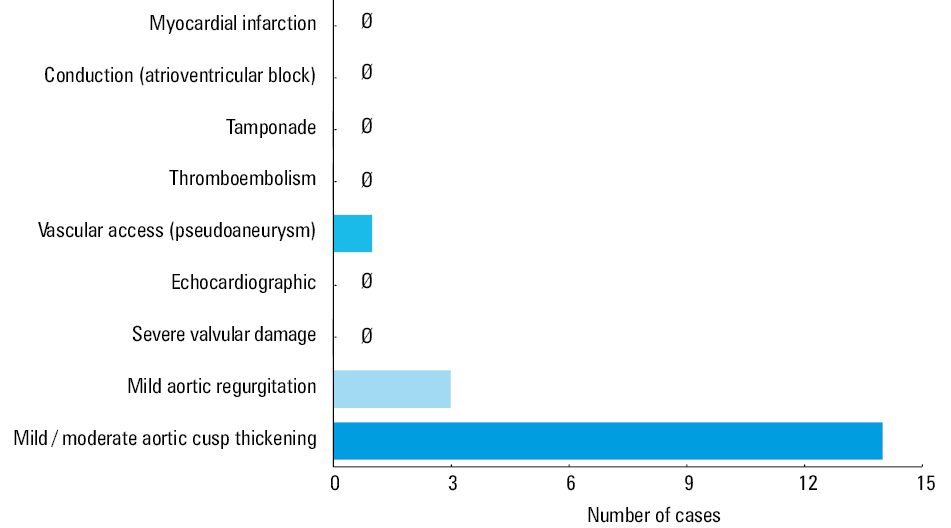
Clinically insignificant aortic valve cusp degeneration (usually marginal cusp thickening or fibrosis, less often mild aortic regurgitation) was observed in 16% of patients. Mild/moderate thickening of the aortic valve was shown in 13 patients, whereas 3 patients had minor complications of mild aortic regurgitation. There was no correlation between mild/moderate aortic thickening, mild aortic regurgitation, the ablation cusp target, and ablation details.
Six patients had echocardiography‑based indications for the MRI. It excluded suspected left ventricular noncompaction cardiomyopathy in 1 case and did not confirm moderate aortic leaflet thickening observed by the echocardiographers in 5 remaining cases. One of these patients had a small (about 4 mm) margin scar within the ablated LCC visible on the MRI, yet undetected on echocardiography. However, an NNC thickening was identified on echocardiography that was not seen on MRI. Except for the scar seen in the MRI, the patient only had insignificant mild aortic regurgitation during the 9‑year follow‑up.
Two patients had moderate aortic stenosis at baseline. There was no progression to severe aortic stenosis in either short- or long‑term follow‑up. The aortic valve area and mean aortic gradient did not increase significantly in either of them.
There were 13 cases with suspected PVC‑induced cardiomyopathy. Of those, LVEF improved after successful ablation in 6 patients, and remained low without improvement even after successful ablation in 7 patients, which suggests another mechanism for cardiomyopathy. The median values of LVEF at baseline, short- and long‑term follow‑up with regard to the ablation outcome are presented in Supplementary material, Table S2.
Other complications
There was a single case of postablation pseudoaneurysm, which was treated surgically (Figure 4). There were no other vascular access complications, no cases of MI, thromboembolism, tamponade, or conduction disorders including ablation‑induced atrioventricular block. One patient had a pacemaker implanted 2 days after ablation, yet the indication (paroxysmal third‑degree atrioventricular block) had been established prior to ablation. One woman experienced a vasovagal reaction with transient elevation of ST‑T segment in leads II, III, aVF during LCC/RCC ablation. Her symptoms resolved spontaneously with no adverse sequelae. Subsequent angiography revealed no pathologies within the coronary arteries.
Concomitant arrhythmias
Additional substrates were identified in 12 out of 103 patients (12%). These were atrioventricular nodal reentry tachycardia, paroxysmal atrial tachycardia, and separate focal areas of VA originating from RVOT (n = 8), RV (n = 1), and left ventricle (n = 2). All additional substrates were ablated during the same procedure.
Discussion
Main findings
This is the first large prospective multicenter analysis of safety and very long‑term clinical and echocardiographic outcomes (median follow‑up of 32 months; IQR, 12–70) after ablation of VAs originating from aortic cusps. The study revealed for the first time that RFA could be performed safely and successfully in the sensitive aortic cusp area, even without fluoroscopy and ablation of additional arrhythmia substrates.
Echocardiographic complications
No data have been published so far on targeted echocardiographic assessment after RFA of the aortic cusp, although this procedure is considered high‑risk for valve/aortic root damage. Serious complications following ablation, such as aortic regurgitation or aortic leaflet perforation are likely, although reluctantly reported.9,10 The iatrogenic aortic valve injury may be caused by the catheter tip as it is passed through the valve, by RFA application in the aortic leaflet area, or by cusp compression with the catheter during its prolonged placement in the left ventricle.
The risk of valvular injuries during aortic retrograde approaches potentially correlates with procedure duration, the number of RFA applications, and passages through the aortic valve, being seemingly higher in children and adolescents with smaller outflow tract diameters.10 Olsson et al10 analyzed 179 patients in whom retrograde aortic approaches were used. Clinically insignificant mild aortic insufficiency was reported in 2 patients.
Our study is the first to evaluate targeted echocardiographic assessments after RFA of aortic cusp VA. After a median observation period of about 32 months, we found no significant aortic leaflet or aortic root pathology in follow‑up echocardiography. The MRI was done in 6 patients to verify echocardiographic findings. It confirmed a single small scar on an ablated aortic cusp as the only identified abnormality. Clinically insignificant degeneration of the valve cusps found in 16% of patients did not correlate with procedure duration or number of RFA applications, but may have been related to aging, as there was little association between cusp ablation target and degenerative changes. One patient was referred for MRI due to moderate thickening of the aortic cusp. Even though the MRI could not confirm it, it revealed a marginal scar on an ablated cusp instead, which had no negative effect seen in a 9‑year follow‑up, except for the mild aortic regurgitation. This shows that echocardiography may not be suitable for detecting subtle aortic cusp changes such as postablation scars. Doppler techniques enable tracking of newly developed aortic regurgitation which might reflect injured cusp retraction and subsequent scar formation. It may be useful for screening for potential ablation‑induced leaflet perforation or for monitoring of the deterioration of preexisting valvular diseases. Such deterioration of echocardiographic parameters, which could indicate severe aortic dysfunction after aortic cusp ablation, was not seen in our 2 patients with preexisting moderate aortic stenosis. In both cases, long‑term follow‑up confirmed continued success.
In our registry, about half of suspected PVC‑induced cardiomyopathy cases were ruled out following successful ablation, with no LVEF reversal in the follow‑up. The true PVC‑induced cardiomyopathy rate was rather low (6%) as compared with other studies which reported the incidence rates up to 40% in selected groups of patients at highly specialist centers with experienced personnel.11
Aortic cusp ventricular arrhythmia origins
The prevalence rates of aortic cusp VA origins are in keeping with previous studies.1,4,7,12 The LCC was the most frequent location, followed by AMC/LCC, LCC/RCC, and RCC. The NCC was the rarest ablation target, found in 6% of subjects, only young males with frequent complex arrhythmias and high ablation success rate reaching 100%. Patients with AMC/LCC VA cusp locations were generally older than patients with other VA cusp targets except for the LCC/RCC. Procedure duration was longer in patients undergoing RCC ablation. Double tachycardia was detected during the EP study in only 2% of patients. In 10% of cases, additional focal VA was encountered, usually within the RVOT. Interestingly, aortic root could also be a substrate for the ablation of other arrhythmias like those in the Wolff–Parkinson–White syndrome, atrioventricular nodal reentrant tachycardia, and atrial tachycardia. Unlike the IVA, the RCC and NCC are targeted more frequently.13
Other complications
Although IVA ablation complications are rare, injuries to the coronary arteries, aortic root, and conduction system have been reported. Coronary angiography has traditionally been recommended before aortic cusp catheter ablation to ensure a safe distance to coronary arteries.1
Chronic left main artery occlusion has been reported as a complication of RFA of idiopathic left VT.14 In a retrospective cohort study of idiopathic PVC ablation outcomes in 1185 patients, including aortic cusp ablation in 15% of procedures,2 the overall complication rate was 5.2% including the most frequently reported vascular access complications (1.3%), tamponade (0.8%) and atrioventricular block (0.1%). In another cohort study by Oomen et al,15 5 (3.8%) of 131 patients undergoing ablation due to symptomatic VA (13% in aortic cusps) had nonfatal complications including 3 tamponades (not during aortic cusp ablation), 1 case of third‑degree atrioventricular block requiring pacemaker, and 1 case of abdominal hematoma.
Our registry included only the patients with VA ablation target in aortic cusps. There were no complications potentially associated with close proximity of the ablation catheter to the aortic root, coronary ostia and conduction system. Only one case of transient vasovagal reaction was observed with no negative consequences. There were no cases of cardiac tamponade. One patient required surgical intervention due to vascular access‑related pseudoaneurysm. One‑third of ablations in the registry were performed via the ZF approach.
Ablation outcomes
Our registry study has accumulated the largest database of VA ablation procedures in aortic cusps with echocardiographic follow‑up to date. Our database includes over 100 patients who underwent RFA at 10 Polish electrophysiology centers over 12 years. The ablations were performed mostly by experienced operators, which increases data homogeneity in statistical comparisons. Previous studies were carried out in significantly smaller patient populations.1,2,5,7,12 So far, there is no data on aortic cusp ablation in SHD. Our data shows comparable procedure outcomes in patients with or without SHD (87% vs 80% in a long‑term follow‑up, P = 0.62) with very few procedure‑related complications, even when preexisting aortic stenosis was present. There were no differences in procedure outcomes relative to VA cusp location.
Our registry ablation procedures were performed by experienced operators, resulting in high treatment success rates (acute 93%, long‑term 86%) along with relatively short median procedure duration (75 minutes), very short fluoroscopy duration (5 minutes), and even complete elimination of fluoroscopy in one‑third of patients. In a recently published retrospective cohort study, the mean procedure duration in IVA aortic cusps ablation and the fluoroscopy duration were considerably longer (178 minutes and 27 minutes, respectively) with comparable long‑term outcomes.2
Ablation technique
Compared with the conventional and 3‑dimensional fluoroscopic techniques, the ZF approach, similarly to Zhu et al,5 reduced the total procedure duration, thus maintaining the high RFA success rate. Modern 3D mapping technology and operator learning curve seem to shorten the procedure and fluoroscopy duration with acute and long‑term RFA success rates comparable with (but not better than) conventionally‑guided procedures.
According to the guidelines, unlike patients with VA of RVOT origin,16 those with VA of LVOT origin including aortic cusp locations should only be treated by RFA after previous failure of antiarrhythmic therapy as the procedure is considered high‑risk. However, VA constitutes a significant clinical problem and medical treatment is often insufficient, especially in patients with poor compliance.6,7 There is no universal best choice treatment for VA. Due to the rare but serious complications of aortic cusp ablation,2,4,5,14 RFA should only be considered in particularly difficult clinical scenarios (highly symptomatic, life‑threatening VA), and patients should be referred directly to experienced electrophysiology centers, thus shortening, or even skipping medical treatment attempts. Using a computer‑assisted semi‑automatic system, which can be implemented in commonly used ECG recorders, described elsewhere by our study group, may additionally facilitate clinical decision‑making of noninvasive cardiologists regarding the VA site of origin.7
Study limitations
One of the study limitations is the technique used for aortic root assessment before and after ablation. Since the beginning of the registry in 2005, in the majority of initial assessments, echocardiography has been used. The follow‑up assessments have also been echocardiography‑based; however, minor changes can be better detected with modern devices, causing potential study bias. Echocardiography is not a reference technique for the detection of subtle cardiac changes; however, due to limited access and high cost, MRI could not be performed in all patients.
Other limitations are a relatively large number of patients lost to follow‑up and patients with incomplete clinical data (Holter monitoring or echocardiography) which were excluded from the baseline study group. This was mainly due to the very long follow‑up, missing contact details, patient deaths or inability to perform all required tests. Also due to the long follow‑up, the final visits took place at different time points (follow‑up IQR, 12–70 months).
Conclusions
Ablation of PVCs/VT within aortic cusps is safe and effective in both short- and very long‑term follow‑up. The ZF approach is feasible and safe; however, better expertise and more imaging modalities are required.
- Yamada T, McElderry HT, Doppalapudi H, et al. Idiopathic ventricular arrhythmias originating from the aortic root prevalence, electrocardiographic and electrophysiologic characteristics, and results of radiofrequency catheter ablation. J Am Coll Cardiol. 2008; 52: 139‑147. | Crossref
- Latchamsetty R, Yokokawa M, Morady F, et al. Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes. J Am Coll Cardiol EP. 2015; 1: 116‑123. | Crossref
- Yamada T, Yoshida N, Doppalapudi H, et al. Efficacy of an anatomical approach in radiofrequency catheter ablation of idiopathic ventricular arrhythmias originating from the left ventricular outflow tract. Circ Arrhythm Electrophysiol. 2017; 10: e004959. | Crossref
- Hoffmayer KS, Dewland TA, Hsia HH, et al. Safety of radiofrequency catheter ablation without coronary angiography in aortic cusp ventricular arrhythmias. Heart Rhythm. 2014; 1: 1117‑1121. | Crossref
- Zhu TY, Liu SR, Chen YY, et al. Zero‑fluoroscopy catheter ablation for idiopathic premature ventricular contractions from the aortic sinus cusp. Nan Fang Yi Ke Da Xue Xue Bao. 2016; 36: 1105‑1109.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION