Estimation of 24-hour urinary sodium, potassium, and creatinine excretion in patients with hypertension: can spot urine measurements replace 24-hour urine collection?
Key words: hypertension, Kawasaki formula, Pan American Health Organization formula, spot urine measurement, Tanaka formula



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Estimation of 24-hour urinary sodium, potassium, and creatinine excretion in patients with hypertension: can spot urine measurements replace 24-hour urine collection?
Owing to inconvenience of a 24‑hour urine collection, diagnostic methods based on spot urine samples are becoming increasingly popular. Spot urine sodium measurements could replace 24‑hour urinary sodium (24hUNa) excretion, considered a surrogate measure of dietary sodium intake. Spot urine–based approaches to estimating 24hUNa and 24‑hour urinary potassium (24hUK) excretion are potentially useful in patients with hypertension, for example, to identify increased urinary potassium excretion in individuals with primary aldosteronism and high dietary sodium intake in those with resistant hypertension. In this review, we summarized our research on spot urine–based estimation of 24hUNa, 24hUK, and 24‑hour urinary creatinine (24hUCr) excretion to avoid the need for a 24‑hour urine collection in patients with hypertension. We found that the Pan American Health Organization (PAHO) formula was generally the best for predicting the average 24hUNa and 24hUK excretion in hospitalized patients with hypertension, while the Kawasaki equation was inferior for estimating 24hUNa and the Tanaka equation was inferior for estimating 24hUK excretion. However, all 3 equations were imprecise in terms of estimating individual 24hUNa or 24hUK excretion. We also confirmed the general utility of the equations for estimating 24hUCr excretion in hypertensive individuals but with significant differences between various equations, the best formulas being Chronic Kidney Disease Epidemiology Collaboration (CKD‑EPI) and Rule. Compared with the combined PAHO/CKD‑EPI formula, the Tanaka and Kawasaki equations underestimated increased 24hUNa and 24hUK excretion. Thus, the combined PAHO/CKD‑EPI formula might be the best for identifying increased 24hUNa and 24hUK excretion in patients with hypertension.
Introduction
Due to inconvenience of a 24‑hour urine collection, attempts have been made to replace it with diagnostic approaches based on spot urine measurements. The most successful of these efforts is probably the measurement of the albumin‑to‑creatinine ratio, which has been gaining popularity as a surrogate measure of albuminuria. At the population level, there has been much interest in using spot urine sodium measurements as a replacement for 24‑hour urinary sodium (24hUNa) excretion, the latter being considered a surrogate measure of dietary sodium intake. Such spot urine–based approaches to estimating 24hUNa and 24‑hour urinary potassium (24hUK) excretion are also potentially useful in patients with hypertension. In the present review, we summarized our previous and current research on estimating 24hUNa, 24hUK, and 24‑hour urinary creatinine (24hUCr) excretion in patients with hypertension with the aim to avoid the need for a 24‑hour urine collection.
Rationale for measuring 24‑hour urinary sodium and potassium excretion in patients with hypertension
The assessment of 24hUNa and 24hUK excretion in patients with hypertension may be clinically useful for several important reasons. The measurements of 24hUNa excretion are widely used to assess dietary sodium intake, as sodium restriction is recommended as an important lifestyle modification both in the general population and in patients with hypertension, and 24hUNa may serve as a surrogate measure of daily oral sodium intake.1 This approach to estimating dietary sodium intake by measuring 24hUNa excretion may be particularly helpful in patients with uncontrolled blood pressure despite an apparently adequate drug therapy, as it might provide an insight into the patient’s compliance regarding dietary sodium restriction.2
The measurement of urinary potassium excretion is most useful in patients evaluated for primary aldosteronism, a common form of secondary hypertension.3 Although the diagnosis of primary aldosteronism is based on identification of autonomous aldosterone secretion, adrenal imaging, and localization of the source of aldosterone excess,3 the detection of hypokalemia and increased urinary potassium excretion remains of some value. Although hypokalemia due to an increased urinary potassium loss is observed only in a minority of patients with primary aldosteronism,4 it is more common in patients with an aldosterone‑producing adenoma, which is potentially curable by adrenalectomy. In a large study, 50% of patients with an adrenal adenoma presented with hypokalemia, compared with only 17% of patients with bilateral adrenal hyperplasia.5 In addition, hypokalemia may produce symptoms such as muscle weakness, paresthesias, and cardiac arrhythmia. On the other hand, hypokalemia may be unrelated to aldosterone and result, for example, from potassium loss due to diuretic use or gastrointestinal disorders. Thus, confirmation of an increased urinary potassium loss that accompanies hypokalemia may help establish an underlying pathophysiologic mechanism and may also help identify patients with primary aldosteronism who are more likely to have a disease amenable to surgical treatment.
Comparison of 24‑hour urine collection and spot urine measurements
Twenty‑four–hour urine collection may be difficult to perform, as it is cumbersome, labor‑intensive, and requires adequate patient cooperation. The need to collect complete urine output over a 24‑hour period imposes a high burden on patients, especially in the outpatient setting.6 These limitations are reflected by low response rates in large population studies.7 In addition, the collection may be unreliable due to difficulties in obtaining a complete 24‑hour sample, resulting both in under- and overcollection.1,7,8 The rates of incomplete collection have been reported to be as high as 30%,8 and no simple methods are available to accurately identify incomplete samples.
The approach we have evaluated to eliminate the need for 24‑hour urine collection is the use of spot (single) urine samples, as they are much easier to collect and store without a risk of under- or overcollection. Spot urine samples are routinely used for the evaluation of urinary albumin excretion9 and have been studied for their utility to assess urinary sodium excretion, mostly for the purpose of estimating salt intake in populations.1,7
Equations to estimate 24‑hour urinary sodium and potassium excretion based on spot urine measurements
Three formulas—Kawasaki,10 Tanaka,11 and Pan American Health Organization (PAHO)12—have been proposed to estimate both 24hUNa and 24hUK excretions based on spot urine measurements. They have been used in several previous studies, mostly to estimate 24hUNa excretion in a healthy general population.13-15 In addition, based on previous comparisons of the Tanaka and Kawasaki formulas, the latter was selected to estimate 24hUNa and 24hUK excretion in a number of large worldwide observational analyses evaluating the relation between urinary sodium and potassium and cardiovascular events.16-18
Other equations have also been developed for sodium, but not potassium, including the INTERSALT formula.19-23 In our studies, however, we chose only those formulas that could be used both for sodium and potassium. Except for the INTERSALT equation, all other formulas were only used in single studies or developed in specific populations, such as patients with chronic kidney disease.19 The INTERSALT equation is more popular, but in the available comparative studies, it was not superior to the equations we selected for the purpose of our research.13,24
The Kawasaki, Tanaka, and PAHO equations for sodium and potassium are presented in Table 1.
Formula | Equation |
Abbreviations: BSA, body surface area; CKD‑EPI, Chronic Kidney Disease Epidemiology Collaboration; Cr, creatinine; K, potassium; Na, sodium; PAHO, Pan American Health Organization | |
Estimated 24‑hour urinary sodium excretion, mmol/24 h | |
Kawasaki10 | 16.3 × [spot urine Na (mmol/l)/spot urine Cr (mmol/l) × estimated 24‑hour urinary Cr (mg)]0.5 |
Tanaka11 | 21.98 × {[spot urine Na (mmol/l)/spot urine Cr (mg/dl) × 10] × [estimated 24‑hour urinary Cr (mg)]}0.392 |
PAHO12 | (measured spot urine Na / measured spot urine Cr) × estimated 24‑hour urinary Cr |
Estimated 24‑hour urinary potassium excretion, mmol/24 h | |
Kawasaki10 | 7.2 × [spot urine Na (mmol/l)/spot urine Cr (mmol/l) × estimated 24‑hour urinary Cr (mg)]0.5 |
Tanaka11 | 7.59 × {[(spot urine K (mmol/l)/spot urine Cr (mg/dl) × 10] × [estimated 24‑hour urinary Cr (mg)]}0.431 |
PAHO12 | (measured spot urine K / measured spot urine Cr) × estimated 24‑hour urinary Cr |
Estimated 24‑hour urinary creatinine excretion, mg/24 h | |
CKD‑EPI36 | 879.89 + 12.51 × weight (kg) – 6.19 × age + (34.51 if black) – (379.42 if female) |
Cockcroft–Gault28 | [28 – (0.2 × age)] × weight (kg) × 0.85 if female |
Walser29 | Men: (28.2–0.172 × age) × weight (kg)
Women: (21.9–0.115 × age) × weight (kg) |
Goldwasser31 | [23.6 – (age/8.3) (+ 1.9 if black)] × weight (kg) |
Rule35 | {exp[7.26–0.26 (if female) – (0.011 × (age – 55) if age >55 years)]} × BSA/1.73 (m2) |
Gerber and Mann27 | 699–421.9 if female + (16.83 × weight) (kg) – 25.82 (if white) – 2.67 × age |
Kawasaki34 | Men: –4.72 × age + 8.58 × weight (kg) + 5.09 × height (cm) – 74.5
Women: –12.63 × age + 15.12 × weight (kg) + 7.39 × height (cm) – 79.9 |
Tanaka34 | –2.04 × age + 14.89 × weight (kg) + 16.14 × height (cm) – 2244.45 |
Estimation of 24‑hour urinary creatinine excretion Any analyte evaluated in spot urine can be expressed as the analyte‑to‑creatinine ratio, as in the case of albumin, iodine, or even catecholamines.9,25,26 However, if the 24hUCr excretion is also known, either measured or estimated, it is possible to convert the spot urine analyte‑to‑creatinine ratio into a more easily comprehensible parameter, namely, an estimated 24‑hour urinary excretion of the evaluated analyte.27 As the ultimate purpose of the spot urine–based approach is to eliminate the need for 24‑hour urine collection, a reliable estimation of 24hUCr excretion is needed. However, although relatively constant, 24hUCr excretion varies by a number of factors including age, sex, body weight, muscle mass, ethnicity, and others.28-33
Although in some studies only rough estimates of 24hUCr excretion based on age and sex were used,15 a number of equations have been developed to estimate 24hUCr excretion based on simple demographic and anthropometric parameters including age, sex, race, and, most commonly, body weight.27-29,31,34-36 Of other reported equations, some are not based on any anthropometric variables reflecting body size,37,38 and some others include parameters that are often not available in routine clinical practice, such as estimates of muscle mass.35,39
The 8 equations for estimating 24hUCr based on demographic and anthropometric variables (Cockcroft–Gault, Walser, Goldwasser, Rule, Chronic Kidney Disease Epidemiology Collaboration [CKD‑EPI], Gerber–Mann, Kawasaki, and Tanaka) that were included in our comparative study on patients with hypertension40 are presented in Table 1.
Statistical approaches to comparing measured and estimated 24‑hour urinary excretion
While numerous previous studies only evaluated the correlation between spot urine measurement and 24‑hour urine collection, we used the Bland–Altman approach, which is considered superior for assessing the agreement between 2 measurement methods, particularly in relation to individual patient management.14,15 The correlation coefficient may not be an appropriate statistical test to assess the agreement between the 2 compared methods, as a high correlation does not necessarily indicate a good agreement between the 2 related measurements.41
The Bland–Altman approach is a method that allows both a numerical and visual assessment of the extent to which the measurements using the new method (ie, estimation using a spot urine–based formula) differ from the reference method (ie, measurement of the actual 24‑hour urinary excretion). This is achieved by plotting measurement differences between the 2 methods against the mean of the 2 measurements (so called Bland–Altman plot). The 95% limits of agreement (LoAs), that is, the expected range of individual differences between the measurements by the 2 methods in 95% of cases, are estimated as the mean difference ±1.96 standard deviation of the mean difference.42,43 The mean difference between the 2 measurements, also called the mean bias, is important from the population perspective, while the LoA may be more important from the clinical or individual point of view. Another parameter is the slope of the regression line on the Bland–Altman plot, which shows how the differences between the measurements by the 2 methods change over the whole measurement range. In our case, it indicated whether a given formula remained similarly precise at the lower and upper end of the 24‑hour urinary excretion range.
Our studies also provided evidence corroborating the concept that the Bland–Altman approach is superior to analyses based on the correlation only. In our comparison of the 3 formulas to estimate 24hUNa and 24hUK excretion,44 correlations between the measured and estimated 24‑hour urinary excretion were similar for all equations both for sodium (r = 0.53 for all 3 formulas) and potassium (r = 0.69 to 0.70). Moreover, these findings were consistent with previous literature data,1,10,11 but the analysis of the Bland–Altman plots revealed important differences between these formulas.
In some previous studies, another approach used to assess the individual precision of the evaluated formulas was to calculate the percentage of the estimated values within a certain margin of error (eg, 15%, 30% and 50%, designated as P15, P30, and P50, respectively) compared with the measured values. We also used this approach in our comparisons of the formulas to estimate 24hUNa, 24hUK, and 24hUCr excretion. Based on previous studies,19 the 30% threshold for individual errors in urinary excretion estimation may be considered clinically most useful and might serve as a reasonably good measure of the utility of a given formula at an individual level. For example, P30 was commonly used to evaluate individual accuracy of equations to estimate glomerular filtration rate.45,46
Comparison of formulas to estimate 24‑hour urinary sodium and potassium excretion in patients with hypertension
In a previous study,44 we used single morning urine samples to compare the estimates of 24hUNa and 24hUK excretion with the Kawasaki, Tanaka, and PAHO equations against the actual measured 24hUNa and 24hUK excretion in patients hospitalized in a specialist hypertension unit and evaluated in the routine clinical practice setting. The rationale for our study was that these 3 formulas for estimating 24hUNa and 24hUK excretion were rarely systematically compared with each other, and no previous study has compared all 3 formulas in patients with hypertension.
The results of our study showed important differences between the 3 formulas. For the estimation of 24hUNa excretion, the mean bias (measured minus estimated 24‑hour urinary excretion) was significantly smaller for the Tanaka (10.5 mmol/d) and PAHO equations (11.5 mmol/d), as compared with the Kawasaki equation (–29.9 mmol/d). The P30 values for Tanaka, PAHO, and Kawasaki equations were 64%, 51%, and 49%, respectively. The Bland–Altman plots also showed that the Tanaka equation underestimated high 24hUNa excretion and overestimated low 24hUNa excretion, becoming clearly less precise at the lower and upper end of the 24hUNa excretion range compared to the PAHO equation. The Kawasaki equation was clearly the least precise of the 3 formulas, and it was characterized by constant overestimation of 24hUNa excretion over its whole range.
For the estimation of 24hUK excretion, the mean bias was significantly smaller for the Kawasaki (7.3 mmol/d) and PAHO equations (8.3 mmol/d), as compared with the Tanaka equation (–16.5 mmol/d). The P30 values for Tanaka, PAHO, and Kawasaki equations were 71%, 61%, and 56%, respectively. The Bland–Altman plots showed that the Kawasaki equation underestimated high 24hUK excretion and overestimated low 24hUK excretion, becoming clearly less precise at the lower and upper end of the 24hUK excretion range compared to the PAHO equation. The Tanaka equation was clearly the least precise of the 3 formulas for potassium.
The overall conclusion from our study was that we found the PAHO formula to be generally the best predictor of the average 24hUNa and 24hUK excretion in hospitalized patients with hypertension. In addition, we observed that the Kawasaki equation was clearly inferior for estimating 24hUNa excretion, and the Tanaka equation was clearly inferior for estimating 24hUK excretion. However, none of the evaluated equations was very precise in terms of estimating individual 24hUNa or 24hUK excretion, and thus their individual precision and accuracy may be inadequate for the purpose of individual clinical decision‑making.
Our findings are generally consistent with the results of previous studies, although most of those studies evaluated these formulas only for sodium and usually in healthy individuals in the general population.13,47 A number of reviews that evaluated the use of spot urine measurements for estimating 24hUNa excretion concluded that this approach may provide adequate mean estimates at the population level, but it is inadequate to evaluate individual 24hUNa excretion.1,7,48 Similar conclusions were also drawn in studies that used P30 or P40 as the measure of individual accuracy of the evaluated formulas.19,24,49
Regarding the relative value of the compared equations, the available data also come mostly from studies performed in the general population. The estimates of 24hUNa excretion using the Kawasaki and Tanaka equations were found to be inadequate in non–Asian populations.15,20,48 In one of these studies, performed in New Zealand in healthy individuals aged 18 to 65 years,15 the PAHO equation was better than the Kawasaki and Tanaka equations for estimating 24hUNa excretion. The usefulness of the PAHO equation for estimating 24hUNa and 24hUK excretion was confirmed in studies performed in various ethnic groups and geographical regions of the world, including Israel and Africa.50,51
The above observations are generally consistent with our findings, but there have also been studies providing conflicting results. For instance, in the only study that directly compared the Tanaka and Kawasaki equations for both potassium and sodium in a large international sample from the general population, the Kawasaki formula performed better than the Tanaka formula both for potassium and sodium.34 Importantly, however, both the Kawasaki and Tanaka equations in that study included the 24hUCr excretion estimated using formulas derived in Asian populations, and the optimal formula for estimating 24hUCr excretion may be different in non–Asian compared with Asian populations, as shown in our study40 (see below). Of note, the PAHO formula was not evaluated in the study by Mente et al.34 However, in a recent study, the Tanaka formula for sodium was found to be more precise than the Kawasaki formula.24
Only few previous studies assessed the usefulness of these 3 formulas for sodium and potassium in patients with hypertension. For example, the Kawasaki formula for sodium was better than the Tanaka formula with morning urine samples in untreated patients with hypertension with normal renal function.52 In addition, most earlier studies evaluated correlations only but did not use the Bland–Altman approach.53,54 No previous study compared all 3 equations for estimating 24hUNa and 24hUK excretion based on spot urine measurements in patients with hypertension. In addition, prior to our studies, the Bland– –Altman approach has not been used to evaluate the diagnostic precision of estimating 24hUK excretion based on spot urine potassium measurements in patients with hypertension.
Comparison of formulas to estimate 24‑hour urinary creatinine excretion in patients with hypertension
Any spot urine–based formulas to estimate 24hUNa and 24hUK excretion require input about the 24hUCr excretion. As noted above, the ultimate purpose of the spot urine–based approach is to render 24‑hour urine collection unnecessary, and thus the estimation of the 24hUCr excretion is needed. A number of equations are available to estimate 24hUCr excretion, preferably using easily available demographic and anthropometric parameters. However, the relative performance of various equations to estimate 24hUCr excretion has not been well studied, and published comparisons with the measured 24hUCr36 include only some of these formulas. In particular, prior to our study, various formulas for estimating 24hUCr had never been compared in patients with hypertension. Thus, we aimed to perform such comparisons in hospitalized patients with hypertension undergoing routine inpatient clinical evaluation, which provided an opportunity to obtain 24‑hour urine collections for the reference measurement of 24hUCr excretion. Therefore, our study provided the first assessment of bias, precision, and accuracy of a number of available equations for estimating 24hUCr in this population.40
In our study, we confirmed a general utility of the equations to estimate 24hUCr excretion in patients with hypertension, but we also found significant differences between the various compared equations. The best formulas in our study population were the CKD‑EPI (mean bias, 0.002 g/d; P30, 86%) and Rule equations (mean bias, 0.022 g/d; P30, 89%), while some other formulas, including the Gerber–Mann, Tanaka, and Kawasaki, were clearly inferior. Of note, the Bland–Altman plots showed that the 2 best formulas, namely, CKD‑EPI and Rule, tended to underestimate high 24hUCr excretion. Two of the older equations (Cockcroft–Gault and Walser) were worse in terms of the mean bias, 95% LoA, and P30 but did not underestimate high 24hUCr excretion.
Another interesting novel finding of our study is an inferior precision of the 24hUCr‑estimating component of the Kawasaki equation, as compared with a number of other equations. This observation may have particular significance because the Kawasaki formula was previously chosen for the spot urine–based estimation of 24hUNa and 24hUK excretion in a number of large worldwide observational studies evaluating the relation between urinary sodium and potassium excretion and cardiovascular events.16-18
In summary, we concluded that at the individual level, the precision of estimating 24hUCr excretion in patients with hypertension was not ideal, even when using the best equations, due to underestimation with higher excretion values, but it was generally similar to the precision of established clinical tools such as equations estimating glomerular filtration rate,36,45 which are considered sufficiently precise for individual clinical decision‑making.
Our results are in line with previous studies that compared some of these equations, mostly in patients with chronic kidney disease. For example, 5 equations were compared by Ix et al,36 who developed the CKD‑EPI formula. In that study, the mean bias for the CKD‑EPI equation was –0.01 g/d, and the P30 value was 79%, while for the other 4 evaluated equations (Cockcroft–Gault, Walser, Goldwasser, and Rule), the mean bias ranged from –0.028 g/d to 0.063 g/d, and P30 values ranged from 76% to 81%. All these results are generally similar to our estimates. Of note, we were unable to identify any previous comparative studies that would include both the Gerber–Mann equation and the Asian formulas (Kawasaki and Tanaka).
Estimates based on spot urine measurements only
In our previous study,44 the actual measured 24hUCr excretion was used in a comparative assessment of the 3 formulas for sodium and potassium, similarly to the approach used in other studies.14,15 However, 24hUCr excretion must also be derived indirectly to truly eliminate the need for a 24‑hour urine collection, and identification of the best formula for creatinine was the purpose of our subsequent study.40 In these studies, we found that the PAHO formula was overall the best for sodium and potassium (considering the mean bias, presence or absence of under- or overestimation at the extreme ends of the urinary excretion range, and parameters describing individual precision of the formulas). Moreover, the CKD‑EPI equation was one of the 2 best formulas for creatinine. Therefore, the next step was to combine the best 24hUNa- and 24hUK‑estimating formula and a superior 24hUCr‑estimating formula to allow a “spot‑urine‑only” approach to estimating 24hUNa and 24hUK excretion in patients with hypertension. The resulting combination of the PAHO and CKD‑EPI equations was compared against the existing reference for spot urine–based estimates, namely, the Tanaka and Kawasaki equations for sodium and potassium.
This analysis included 293 patients from a previous dataset (170 women and 123 men; mean [SD] age, 54 [16] years) who underwent clinical evaluation and diagnostic tests for hypertension in our tertiary care unit, and for whom the results of sodium, potassium, and creatinine measurements in spot urine and 24‑hour urine collection as well as necessary demographic and anthropometric data were available. Details regarding the study protocol and patient characteristics are available in the previously published papers.40,55 A noninterventional design of the study was formally confirmed by the local ethics committee at our institution.
Similarly to the approach used in our previous study on equations for creatinine, in order to reduce bias related to potential 24‑hour urine under- or overcollection, affecting the accuracy of reference measurements in 24‑hour urine collection, for the main analysis we only included patients in whom the measured 24hUCr excretion expressed in mg/kg/d was within the expected or reference range, serving as a measure of completeness of individual 24‑hour urine collections. However, various reference ranges for the measured 24hUCr excretion were reported in the literature,56,57 and to include the largest number of patients, we used the most liberal inclusion criteria, based on the reference ranges reported by Mayo Clinic (men, 13–29 mg/kg/d; women, 9–26 mg/kg/d).56 As a sensitivity analysis, we repeated our analysis in the overall study population.
The results of these analyses are shown in Table 2 and Figure 1. In the main analysis for sodium, the combined PAHO/CKD‑EPI formula was shown to be somewhat worse than the Tanaka formula in terms of the mean bias (5.5 vs 14.4 mmol/d), 95% LoA, and P30 values (45% vs 60%), while the Kawasaki formula had the highest mean bias (–34.7 mmol/d), with similar 95% LoA and P30 values as the combined PAHO/CKD‑EPI formula. However, the Tanaka formula clearly underestimated high 24hUNa excretion, unlike the Kawasaki and combined PAHO/CKD‑EPI formulas.
Formula | Mean biasa, mmol/d | 95% limits of agreement | P15 | P30 | P50 |
a Measured minus estimated 24‑hour urinary sodium/potassium excretion
b Measured 24‑hour urinary creatinine excretion 13–29 mg/kg/d in men, 9–26 mg/kg/d in women56
Abbreviations: P15, P30, P50, percentage of estimated values within ±15%, 30%, 50% of the actual measured values; others, see Table 1 | |||||
Main analysis: Mayo Clinic inclusion criteriab (n = 248) | |||||
24‑hour urinary sodium excretion | |||||
PAHO/CKD‑EPI | 14.4 | –149 to 178 | 29 | 45 | 69 |
Tanaka | 5.5 | –124 to 135 | 32 | 60 | 81 |
Kawasaki | – 34.7 | –179 to 110 | 27 | 46 | 69 |
24‑hour urinary potassium excretion | |||||
PAHO/CKD‑EPI | 7.8 | –34 to 50 | 29 | 53 | 82 |
Tanaka | 15.1 | –24 to 54 | 26 | 57 | 85 |
Kawasaki | 6.4 | –31 to 43 | 39 | 64 | 90 |
All patients (n = 293) | |||||
24‑hour urinary sodium excretion | |||||
PAHO/CKD‑EPI | 1.9 | –180 to 180 | 26 | 40 | 62 |
Tanaka | –3.6 | –141 to 134 | 29 | 54 | 75 |
Kawasaki | –44.7 | –200 to 111 | 25 | 42 | 63 |
24‑hour urinary potassium excretion | |||||
PAHO/CKD‑EPI | 2.8 | –49 to 54 | 27 | 50 | 76 |
Tanaka | 12.1 | –30 to 54 | 24 | 55 | 81 |
Kawasaki | 3.1 | –38 to 44 | 36 | 60 | 84 |
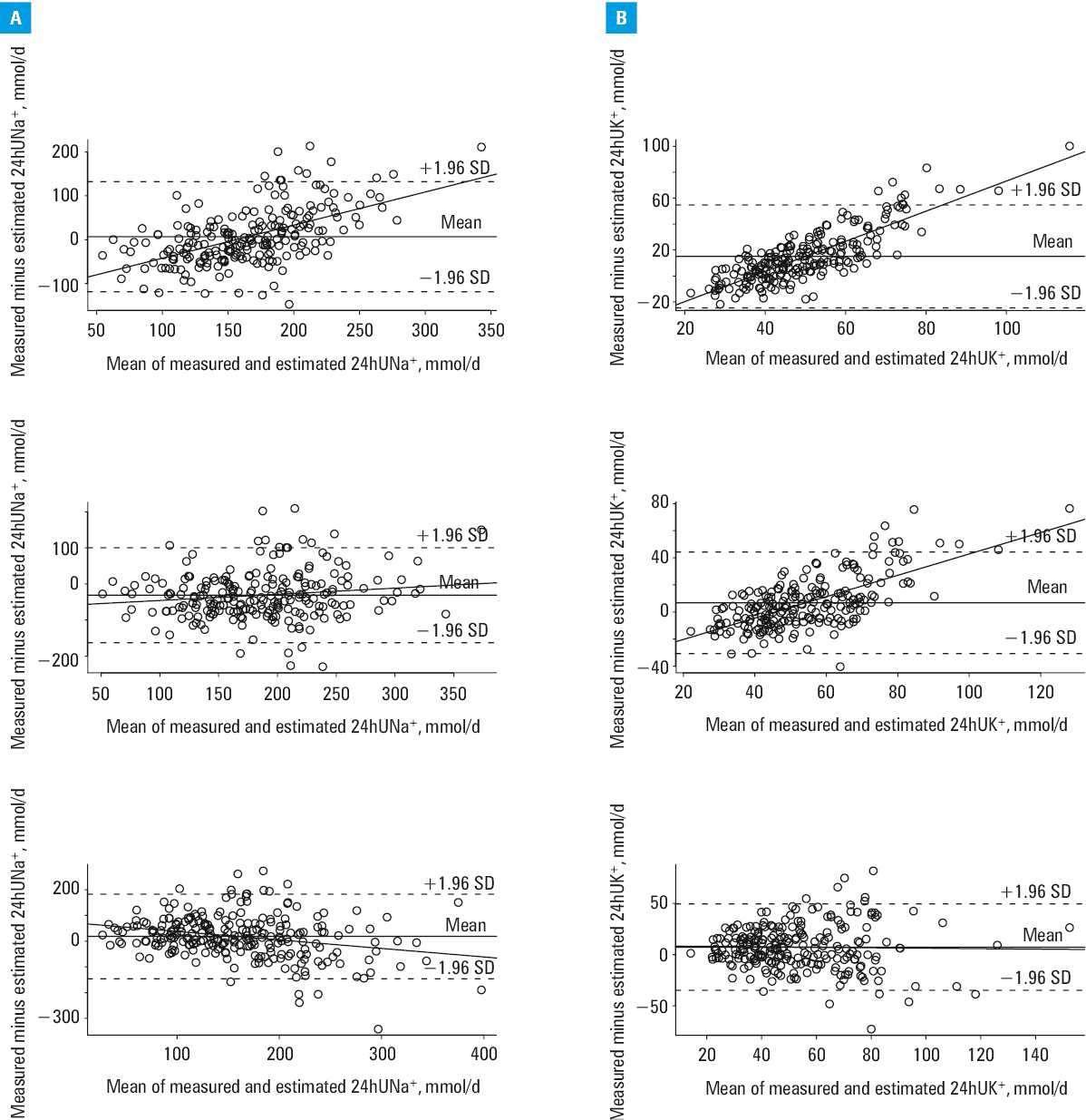
In the main analysis for potassium, the combined PAHO/CKD‑EPI formula was characterized by a similar mean bias compared with the Kawasaki formula (7.8 vs 6.4 mmol/d) but had a somewhat wider 95% LoA and lower P30 value (53% vs 64%). The Tanaka formula had the highest mean bias (15.1 mmol/d), with similar 95% LoA and P30 values as the combined PAHO/CKD‑EPI formula. However, both Kawasaki and Tanaka formulas clearly underestimated high 24hUK excretion, unlike the combined PAHO/CKD‑EPI formula. Overall differences between the formulas both for sodium and potassium were significant by the Friedman rank sum test (P <0.001).
P30 values were rather low even for the best formulas both for sodium and potassium. This, together with wide 95% LoAs, indicates that the individual precision of the combined PAHO/CKD‑EPI formula and the comparator formulas is clearly suboptimal for the purpose of individual clinical decision‑making. However, the accuracy of both the combined PAHO/CKD‑EPI and the Kawasaki formulas for potassium was somewhat higher than that for sodium. All the above results were generally similar when these analyses were performed in the overall study population (all patients, Table 2).
In summary, we were unable to show a clear superiority of the combined PAHO/CKD‑EPI formula over the Tanaka formula for sodium and the Kawasaki formula for potassium in patients with hypertension. However, these Asian population–derived formulas underestimated 24hUNa or 24hUK excretion (or both) when it was increased in our hypertensive population. Thus, for the 2 purposes identified as the main rationale for measuring 24hUNa and 24hUK excretion in patients with hypertension, that is, identification of increased urinary potassium loss in patients with primary aldosteronism and identification of high dietary sodium intake in patients with resistant hypertension, the combined PAHO/CKD‑EPI formula might be actually the best.
Regarding generalizability of our findings, this issue was discussed in more detail in our previous paper.44 In brief, we studied patients admitted to a specialist hypertension unit, and our study was performed in a typical in‑hospital clinical setting, using standard laboratory methods in patients undergoing routine clinical and diagnostic evaluation, without any special oversight over the quality of urine collection. Thus, our findings are likely to represent the accuracy of estimating 24hUNa and 24hUK excretion that may be expected in routine inpatient clinical practice and not in the research setting. In addition, based on the patient characteristics, our findings are likely generalizable to a white population with hypertension that is seen by hypertension specialists or admitted to specialized hypertension units due to such problems as difficult‑to‑control hypertension or suspected secondary hypertension.44 However, owing to the fact that all our patients were white, our results are not necessarily valid for populations of other races or ethnicities.
Factors responsible for imprecision of the spot urine–based formulas to estimate 24‑hour urinary excretion
A perfect agreement between the measured 24‑hour urinary excretion of an analyte and any estimates of 24‑hour urinary excretion based on spot urine measurements cannot be expected for several reasons, regardless of which formula is used. These include inherent imprecision of the equations, inherent variation in spot urine levels of the analyte and its 24‑hour urinary excretion, and errors in urine collection for the determination of actual 24‑hour urinary excretion.40For example, the estimates of 24hUNa or 24hUK excretion based on spot urine measurements cannot be expected to match the actual 24‑hour urinary excretion with a very high degree of precision. This is because spot urine measurements reflect urinary excretion over a shorter time period of only a few hours, and urinary sodium and potassium excretion is not constant throughout 24 hours.55 It may fluctuate depending on a number of factors such as dietary intake, patient activity and posture, kidney and urinary system function, and the effect of neurohormonal factors.1,58In addition, validity of a single 24‑hour urinary collection for estimation of the individual sodium and potassium intake has been questioned by the evidence of intrinsic long‑term fluctuation in urinary sodium and potassium excretion at constant dietary intakes, which depended on hormonal factors (mostly aldosterone).59,60
Urinary creatinine excretion is considered relatively stable when serum creatinine is maintained at steady levels, and in these conditions, 24hUCr excretion depends mainly on endogenous creatinine generation. The latter is largely a function of muscle mass35 and varies by such factors as age, sex, body weight, and race.28-31 The equations to estimate 24hUCr excretion are based on demographic and anthropometric variables, because they are readily available in clinical practice and correlate with muscle mass, which is the primary source of creatinine generation, but this correlation is imperfect (although, as shown in this review, the formulas for creatinine are generally more precise than those for sodium and potassium). In addition, 24hUCr excretion may also show some variation in relation to other factors that are not accounted for in the formulas, such as day‑to‑day variation in protein intake, physical activity, and emotional stress.32,33
Summary and conclusions
Obtaining a spot urine sample is clearly more convenient compared with 24‑hour urine collection. Thus, spot urine measurements, despite their potentially lower accuracy, are preferred in large population studies.16-18 However, individual precision of these formulas has been consistently shown to be suboptimal. Despite this, some clinical utility at the individual level is still foreseeable. For example, we have previously showed that the PAHO formula may be useful for identification of increased urinary potassium excretion, as indicated by the area under the curve of 0.84 for identifying 24hUK excretion of 40 mmol/d or higher in patients with hypertension in our study.55
Our attempts to identify a single and simple formula that would be superior to the Tanaka and Kawasaki equations for sodium and potassium brought mixed results. In our studies discussed in the current review, we were unable to show a clear superiority of the combined PAHO/CKD‑EPI formula in hypertensive patients, especially over the Tanaka formula for sodium and the Kawasaki formula for potassium. However, we found that the Tanaka formulas for sodium and potassium and the Kawasaki formula for potassium underestimated high 24hUNa and 24hUK excretion, respectively.
Several previous studies also demonstrated a systematic bias at extremes of urinary sodium excretion when comparing spot urine–based estimates and 24‑hour urine measurements.19,34 Of note, whether the bias of a formula is stable across the range of urinary excretion of the evaluated analyte (ie, whether a formula under- or overestimates at extreme ends of this range) may be very important even at the population level. This varying bias of the Kawasaki formula over the range of urinary sodium excretion was suggested as one possible explanation of the observed discrepancies between studies based on 24‑hour urine collection, showing a linear association between higher sodium excretion and cardiovascular events, and studies using spot urine specimens, which consistently demonstrated J‑shaped or U‑shaped relationships with cardiovascular disease and mortality.61
Thus, we showed that for the 2 purposes identified in this review as the main rationale for measuring 24hUNa and 24hUK excretion in patients with hypertension (ie, identification of increased urinary potassium excretion in patients with primary aldosteronism and identification of high dietary sodium intake in patients with resistant hypertension), the combined PAHO/CKD‑EPI formula both for sodium and potassium might still prove the best approach for spot urine–based estimates, perhaps even superior to the Kawasaki equations for sodium and potassium that were previously used in large international population studies with hard cardiovascular endpoints.
Finally, if we consider that a single 24‑hour urine collection may be not sufficient for precise evaluation of sodium and potassium intake/urinary excretion, then reasonably precise multiple spot urine–based estimates would become even more convenient and feasible in comparison to multiple 24‑hour urine collections. This might have obvious implications not only for clinical practice but also for research on newly identified regulatory mechanisms of sodium balance related to tissue sodium storage, which may prove equally important for the pathophysiology of hypertension as other recent advances that were elegantly reviewed by Hering et al.62
- Ji C, Sykes L, Paul C, et al. Systematic review of studies comparing 24‑hour and spot urine collections for estimating population salt intake. Rev Panam Salud Publica. 2012; 32: 307‑315. | Crossref
- Agarwal R. Resistant hypertension and the neglected antihypertensive: sodium restriction. Nephrol Dial Transplant. 2012; 27: 4041‑4045. | Crossref
- Funder JW, Carey RM, Mantero F, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016; 101: 1889‑1916. | Crossref
- Mulatero P, Stowasser M, Loh KC, et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004; 89: 1045‑1050. | Crossref
- Rossi GP, Bernini G, Caliumi C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006; 48: 2293‑2300. | Crossref
ARTICLE INFORMATION