Coffee bean sign, beak-shaped transition point, and endoscopic whirl sign of huge sigmoid volvulus in intestinal neuronal dysplasia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Coffee bean sign, beak-shaped transition point, and endoscopic whirl sign of huge sigmoid volvulus in intestinal neuronal dysplasia
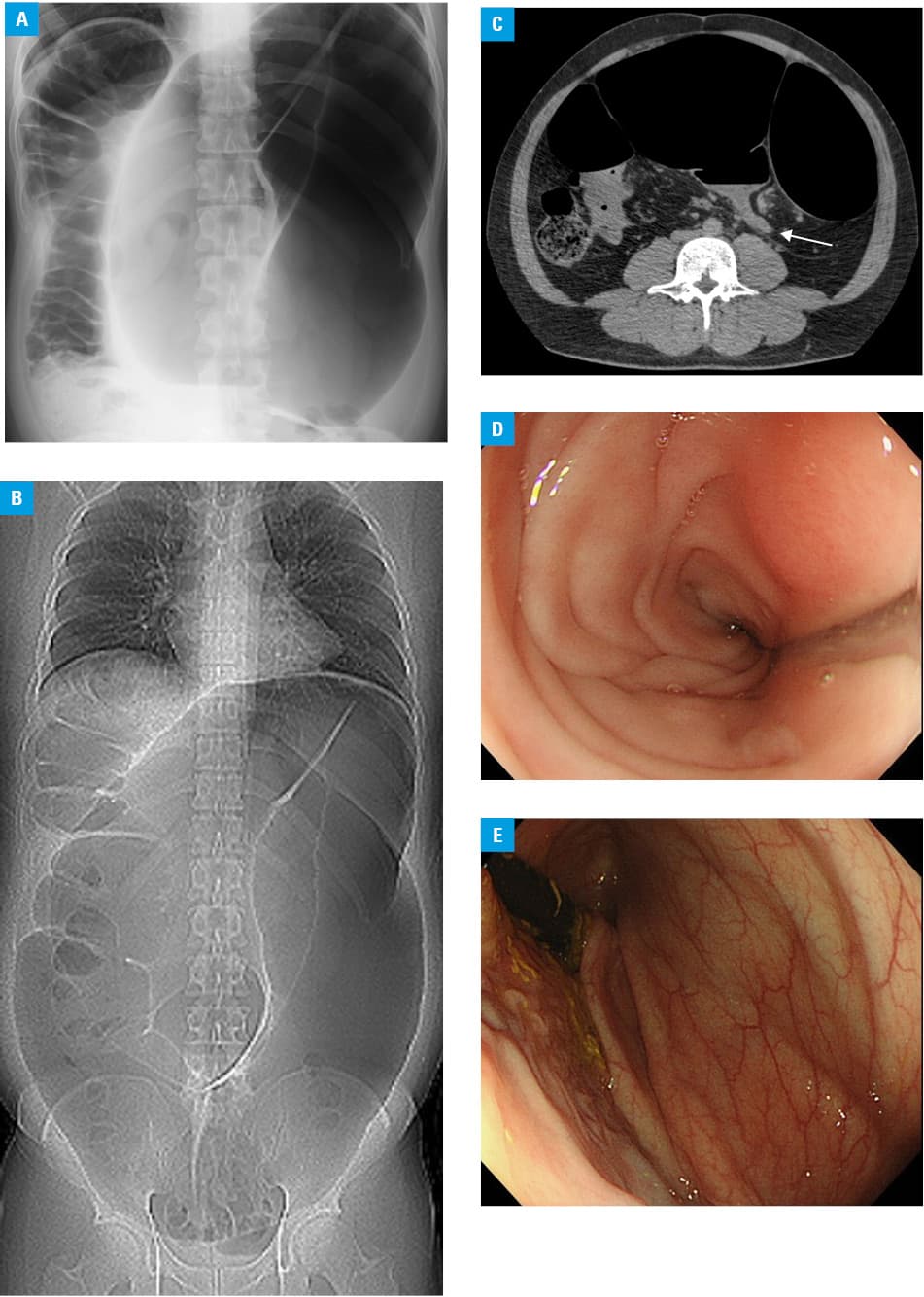
A 27‑year‑old man presented with a 6‑year history of chronic abdominal distension and constipation. Vital signs were stable and abdominal examination revealed generalized distension and nontenderness with decreased bowel sounds. Plain spine radiography showed the dilated loop of sigmoid colon with an inverted U shape and an air‑fluid level, suggesting sigmoid volvulus (SV) (Figure 1A). The abdominal computed tomography (CT) scout view confirmed a huge coffee bean sign1 of SV extending into the subphrenic region (Figure 1B). The CT scan showed the steel pan sign2 of SV and a beak‑shaped transition point, which was the stenotic point due to a fusiform tapering of the bowel loop (Figure 1C). Subsequent endoscopy disclosed a whirl‑like appearance at the luminal narrowing twisted due to torsion (Figure 1D). The scope was then inserted through this point into the dilated sigmoid colon (Figure 1E) and decompressed the lumen. After that, frequent colonoscopic decompression and detorsion were needed for recurrent refractory SV. The patient eventually underwent elective colectomy and ileorectal anastomosis. The diagnosis of intestinal neuronal dysplasia was made after pathologic examination. Postoperative course was uneventful and the patient reported a favorable improvement in his intestinal function and quality of life.
Sigmoid volvulus is a common cause of colonic obstruction and a potentially life‑threatening condition. It was described in a papyrus from ancient Egypt, and later Hippocrates advocated the treatment.3 Predisposing factors include congenital or acquired anatomical variations, such as a long, redundant sigmoid colon and megacolon, previous abdominal surgery, chronic constipation, and neurologic disease.3 Various names have been given to its radiological appearance.1-5 Although plain radiographic features seem to be of diagnostic value, CT scan signs can be useful in identifying the etiology and disclosing ischemic change. Conservative treatment by endoscopic decompression is acceptable and surgery may be required for emergencies including infarction and perforation, and refractory SV, as in this case.3,4
- Feldman D. The coffee bean sign. Radiology. 2000; 216: 178‑179. | Crossref
- Singh Y, Islam S, Arra A, et al. The steel pan sign of sigmoid volvulus – a case series. Int J Surg Case Rep. 2017; 41: 332‑335. | Crossref
- Gingold D, Murrell Z. Management of colonic volvulus. Clin Colon Rectal Surg. 2012; 25: 236‑244. | Crossref
- Vandendries C, Jullès MC, Boulay‑Coletta I, et al. Diagnosis of colonic volvulus: findings on multidetector CT with three‑dimensional reconstructions. Br J Radiol. 2010; 83: 983‑990. | Crossref
- Levsky JM, Den EI, DuBrow RA, et al. CT findings of sigmoid volvulus. AJR Am J Roentgenol. 2010; 194: 136‑143. | Crossref
ARTICLE INFORMATION