Erythromelalgia is a rare microvascular disease characterized by recurrent, severe, burning pain and swelling accompanied by erythema of the extremities. It can be primary or, more frequently, secondary. Primary erythromelalgia, also known as Mitchell disease, may occur spontaneously at any age. In contrast, secondary erythromelalgia is predominantly associated with myeloproliferative syndromes, connective tissue disorders, or infectious diseases. Primary erythromelalgia is frequently caused by mutation of the SCN9A gene that encodes the voltage‑gated sodium channel α subunit.1
A 63‑year‑old woman presented with a 6‑year history of paroxysmal attacks of burning pain accompanied by erythema affecting both hands and feet. She was physically active but in order to avoid pain, she immersed her feet in cold water daily in the summer. She also reported a 40‑year history of Raynaud phenomenon with pallor involving all fingers on each hand.
Physical examination revealed erythema of the upper and lower extremities with no evidence of skin disease. The patient did not exhibit any clinical or biological signs of connective tissue disease. Peripheral pulses, capillary refill time, and the results of nailfold capillaroscopy were normal. Laboratory tests including full blood count and the measurement of rheumatoid factor, C‑reactive protein, and antinuclear antibody levels did not show any abnormalities. We diagnosed primary erythromelalgia associated with primary Raynaud phenomenon, but the patient was not willing to take any drugs.
Laser speckle contrast imaging (LSCI) is a technique that allows noninvasive and real‑time monitoring of peripheral microcirculatory blood flow in a large area of the body. It demonstrates very good reproducibility as well as excellent spatial and temporal resolutions.2 In clinical studies, LSCI coupled with reactivity tests enables the assessment of endothelial and neurovascular function. It is also an innovative tool to evaluate microvascular response to pharmacological treatment.3
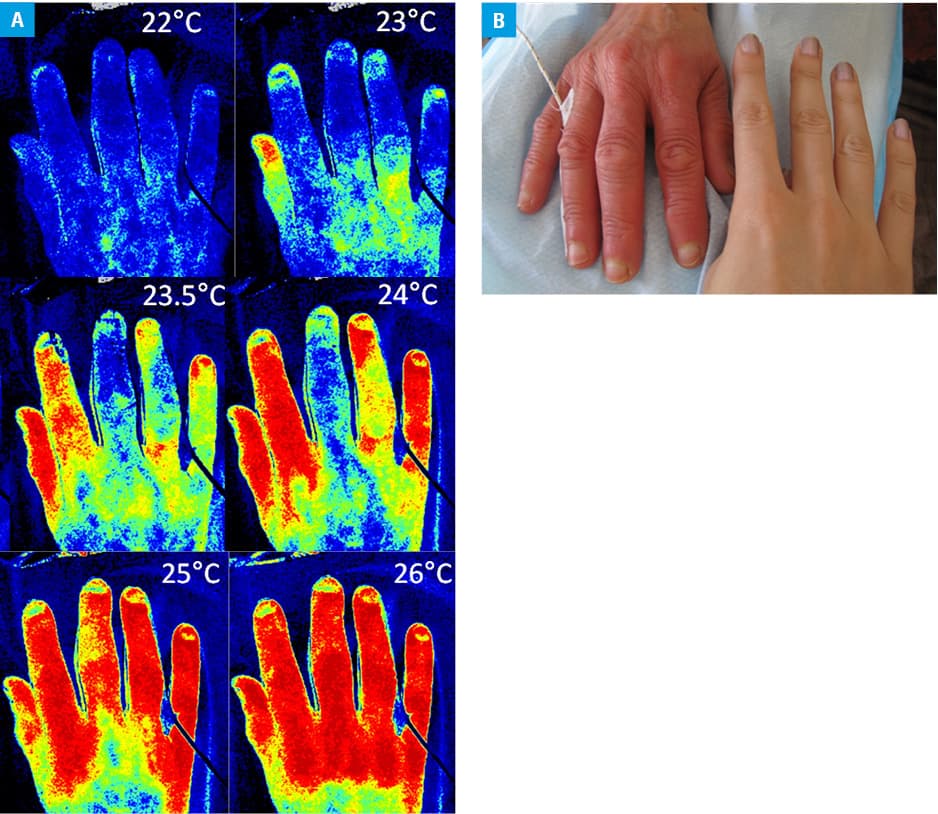
Laser speckle contrast imaging scans shown in Figure 1A illustrate skin microvascular perfusion with colors ranging from blue (low perfusion) to red (high perfusion). The LSCI method provides a perfusion index proportional to skin blood flow and allows the capture of up to 100 images per second.4 At a temperature of 22°C, the patient demonstrated peripheral vasoconstriction. We induced thermal hyperemia by raising the room temperature from 22°C to 26°C. The patient developed a paroxysm of erythromelalgia when the temperature exceeded 25°C (Figure 1B) and it was preceded by a rapid increase in microvascular blood flux.
In the present case, we observed the coexistence of erythromelalgia and Raynaud phenomenon, which is very rarely reported in the literature as both conditions present with distinctly different clinical symptoms.1 The measurements of skin blood flux coupled with reactivity tests enabled the observation of microvascular dysfunction.
- Berlin AL, Pehr K. Coexistence of erythromelalgia and Raynaud’s phenomenon. J Am Acad Dermatol. 2004; 50: 456‑460. | Crossref
- Roustit M, Millet C, Blaise S, et al. Excellent reproducibility of laser speckle contrast imaging to assess skin microvascular reactivity. Microvasc Res. 2010; 80: 505‑511. | Crossref
- Roustit M, Cracowski JL. Assessment of endothelial and neurovascular function in human skin microcirculation. Trends Pharmacol Sci. 2013; 34: 373‑384. | Crossref
- Hellmann M, Cracowski JL. Laser speckle contrast imaging of Raynaud phenomenon. Pol Arch Med Wewn. 2014; 124: 483‑484. | Crossref
ARTICLE INFORMATION