A 42‑year‑old man with skin melanoma was admitted to the Department of Endocrinology and Internal Medicine of the Medical University of Gdańsk due to a focal lesion in the left adrenal gland (most likely a metastasis) found on computed tomography (CT) (Figure 1A and 1B).
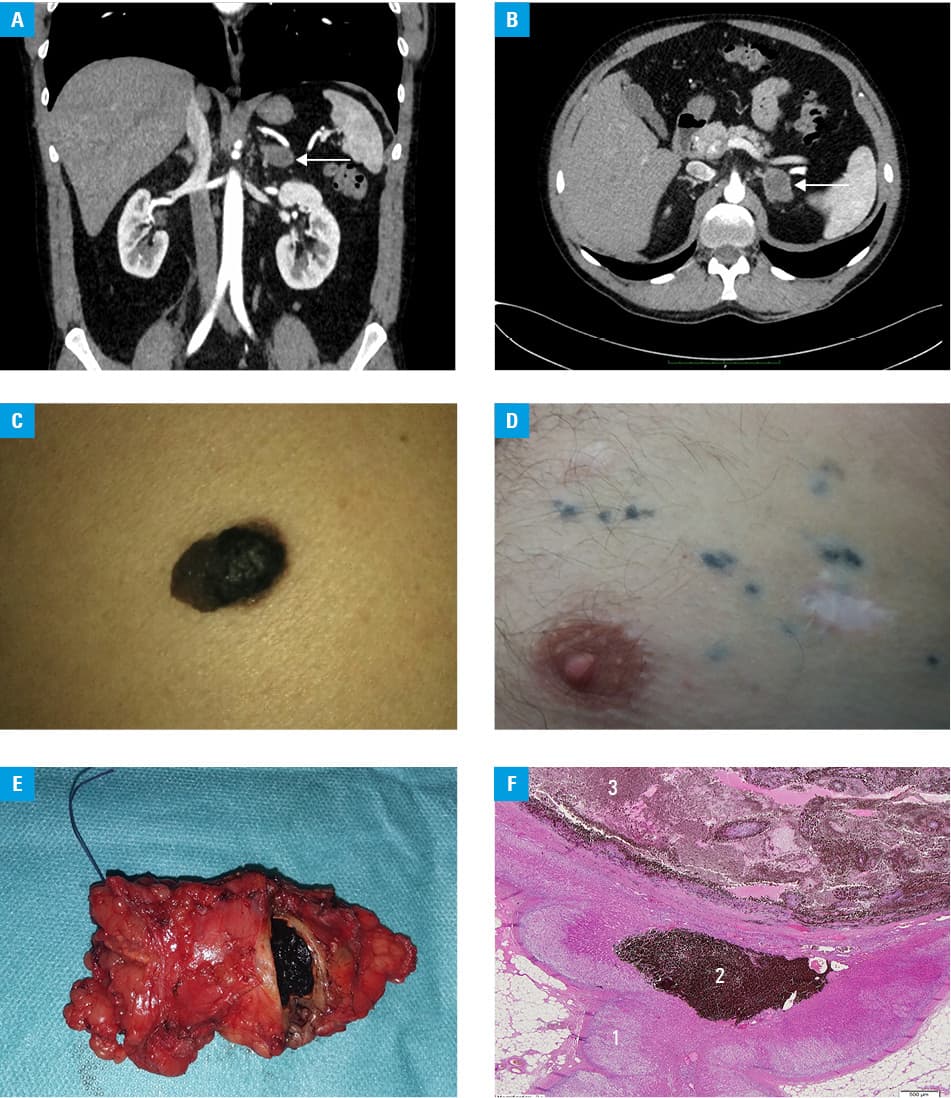
The primary skin lesion was completely removed from the left lumbar region in December 2016 (Figure 1C). Histopathologic examination revealed superficial spreading melanoma with several lymph vessel tumor emboli with no features of infiltration of blood vessels and nerves, without microscopic satellite foci (pathological stage pT3bNxMx, Tumor‑Node‑Metastasis classification). In March 2017, a metastasis to the sentinel lymph node was found. Axillary lymph nodes were surgically excised. All removed lymph nodes (n = 26) showed no metastatic features. In September 2017, the whole body CT scan revealed metastases to the skin, subcutaneous tissue of the chest (Figure 1D), and lymph nodes of the left axilla. Genetic testing showed the BRAFV600E mutation in a tissue sample from the metastases. The patient was enrolled into a clinical trial with placebo versus talimogene laherparepvec (T‑VEC, a drug used in viral immunotherapy, administered directly into the tumor) with pembrolizumab (a humanized monoclonal antibody directed against programmed cell death 1 administered intravenously). The clinical trial protocol involved a whole body CT scan every 3 months. In January and April 2018, radiological assessment revealed a small decrease in the size of both metastatic lymph nodes and metastases to the subcutaneous tissue. The CT scan performed in July 2018 revealed 2 lesions (19 × 14 mm and 12 × 8 mm) in the left adrenal gland. They had heterogeneous structure and displayed contrast enhancement. Numerous but not significantly enlarged retroperitoneal lymph nodes were present. Subsequent imaging performed in November 2018 revealed the enlargement of the adrenal lesion to 36 × 25 mm. Due to the progression of the disease, the patient was excluded from the clinical trial and combination therapy with tyrosine kinase inhibitors (dabrafenib and trametinib) was introduced. Additionally, left‑sided adrenalectomy was scheduled. Hormonal assessment carried out in accordance with the guidelines of the Polish Society of Endocrinology revealed normal activity of adrenal hormones.1 In January 2019, a left‑sided laparoscopic adrenalectomy with lymphadenectomy was performed (Figure 1E). Histopathologic examination revealed melanoma metastases to the adrenal parenchyma, a single lymph node, and the adipose tissue (Figure 1F). No features of vascular invasion were found.
There has been a steady increase in the incidence of cutaneous melanoma for several decades.2 According to the World Health Organization, the incidence in Europe is around 11.5 per 100000 inhabitants.3 Melanoma metastases are most often found in distant lymph nodes, the lung, liver, and brain.4 Adrenal gland metastases are very rare.5 The reported case demonstrates that they should be considered, especially in the presence of any alarming symptoms that might suggest deficiency of hormones produced by the adrenal glands.
- Bednarczuk T, Bolanowski M, Sworczak K, et al. Adrenal incidentaloma in adults – management recommendations by the Polish Society of Endocrinology. Endokrynol Pol. 2016; 67: 234‑258. | Crossref
- Karimkhani C, Green AC, Nijsten T, et al. The global burden of melanoma: results from the Global Burden of Disease Study 2015. Br J Dermatol. 2017; 177: 134‑140. | Crossref
- The Global Cancer Observatory. International Agency for Research on Cancer website. http://gco.iarc.fr/. Accessed May 1–2, 2019.
- Duncan LM. The classification of cutaneous melanoma. Hematol Oncol Clin North Am. 2009; 23: 501‑513. | Crossref
- Xu B, Hong Y, Jin M, et al. Primary adrenal malignant melanoma: a case report and review of literature. Medicine (Baltimore). 2017; 96: e8956. | Crossref
ARTICLE INFORMATION