Innominate arteriovenous fistula following laser lead extraction: endovascular treatment of a potentially fatal complication



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Innominate arteriovenous fistula following laser lead extraction: endovascular treatment of a potentially fatal complication
The increased use of cardiovascular implantable electronic devices over recent years is associated with a higher rate of distinctive complications and, as a result, an increasing number of lead extraction procedures. In most cases, transvenous lead extraction (TLE) is performed, which is less invasive than surgical removal. However, it can be complicated by several conditions, including an arteriovenous fistula (AVF), which is rare but potentially fatal.1 To date, 5 cases of an innominate arteriovenous fistula (IAVF) following laser lead extraction have been reported, with an overall mortality rate of 40%.2-4 We describe an effective endovascular treatment of IAVF with a balloon‑expandable peripheral stentgraft.
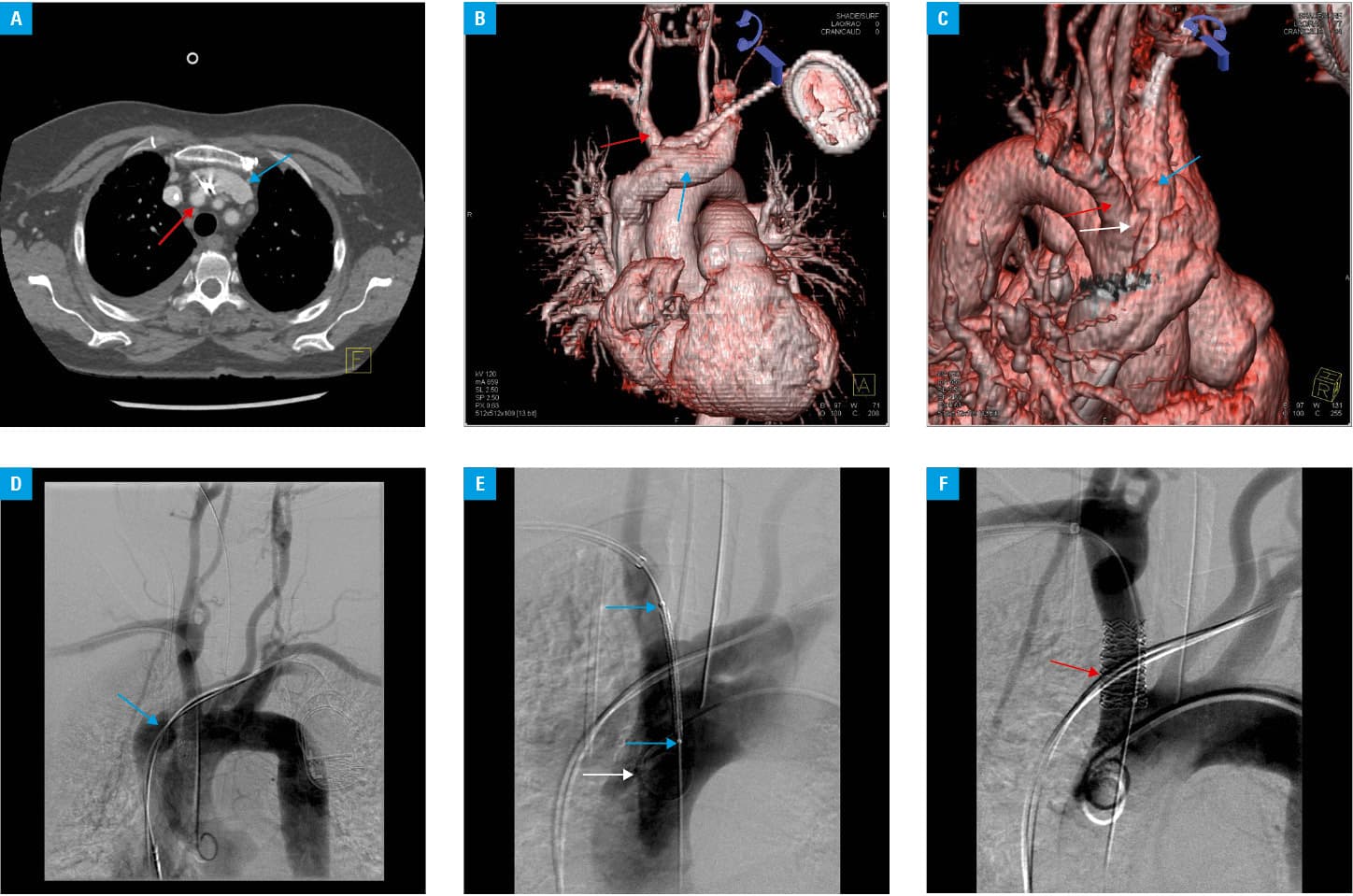
A 75‑year‑old woman with a history of 3 myocardial infarctions, sick sinus syndrome, left ventricular ejection fraction of 55%, and a pacemaker implantation 15 years earlier underwent a percutaneous laser extraction of a fractured atrial lead with a simultaneous insertion of a new DDDR pacemaker (Etrinsa 6 DR‑T, Biotronik, Berlin, Germany) with 2 leads (right atrium and ventricle). The procedure was complicated by a hemorrhagic shock, which occurred immediately after lead extraction. A decrease in blood pressure from 118/53 mm Hg to 48/27 mm Hg, a heart rate of 141 bpm, and excessive sweating were noted. The patient required an intravenous infusion of norepinephrine (8 µg/min) and blood transfusion (2 units of packed red blood cells). Computed tomography angiography, performed due to circulatory instability, revealed the presence of IAVF (Figure 1A–1C). She was immediately referred for an endovascular treatment in a hybrid operating room. A peripheral stent graft (BeGraft Peripheral 10 × 37 mm, Bentley, Hechingen, Germany) was successfully implanted to the affected innominate artery (Figure 1D–1F) under general anesthesia. After 2 weeks, the patient was discharged in stable good condition. Her left ventricular ejection fraction was 55% and remained unchanged at follow‑up visits during the next 1.5 years.
Lead dysfunction is the second (after infection) most frequent indication for lead extraction.5 In TLE, non‑powered telescoping and powered sheaths (including laser systems) are commonly used; however, both can result in AVF formation.1,4 Of the 5 previously reported cases of the IAVF following laser lead extraction, 2 were fatal without an attempt at endovascular treatment.2,3 In 2014, Cronin et al4 reported a successful treatment of 2 patients with a balloon‑expandable stent graft implantation and a spontaneous closure of the fistula in 1 patient. Although every patient with IAVF was diagnosed during the TLE or postmortem, cases of AVF in different vascular locations were recognized even 586 days after the procedure.
Complete fistula formation is not always simultaneous with vessel injury and may even last for weeks. Therefore, due to a growing number of patients after TLE, one should keep in mind that potentially fatal complications might become symptomatic days or even weeks after the procedure. Late signs of AVF include continuous bruit with systolic accentuation over the anterior chest, upper extremity and facial swelling, and dilated veins. As continuous bruit is most consistent with the diagnosis, every physical examination of patients after TLE should include auscultation of the anterior chest area, as it may aid the proper diagnosis.4 Moreover, because an AVF is rarely found during TLE, the awareness of this potentially fatal complication is critically important in terms of appropriate diagnosis and patient management.
- Kang P, Nunez DB Jr. Arteriovenous fistula following pacemaker lead removal: CT diagnosis. Emerg Radiol. 2003; 10: 40‑42.
- Cirillo RL Jr, Fontaine AB. Iatrogenic brachiocephalic arteriovenous fistula: description of a fatal complication after cardiac pacemaker lead extraction. J Vasc Interv Radiol. 1998; 9: 1029‑1030. | Crossref
- Chen PC, Greenberg S, Mathuria N, Livesay JJ. Operative repair of iatrogenic innominate artery to left innominate vein arteriovenous fistula after pacemaker laser lead extraction. J Thorac Cardiovasc Surg. 2016; 152: 85‑87. | Crossref
- Cronin EM, Brunner MP, Tan CD, et al. Incidence, management, and outcomes of the arteriovenous fistula complicating transvenous lead extraction. Heart Rhythm. 2014; 11: 404‑411. | Crossref
- Polewczyk A, Jacheć W, Polewczyk AM, et al. Infectious complications in patients with cardiac implantable electronic devices: risk factors, prevention, and prognosis. Pol Arch Intern Med. 2017; 127: 597‑607. | Crossref
ARTICLE INFORMATION