Cast-like calcification in the superior vena cava in a young woman with lupus nephritis on hemodialysis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Cast-like calcification in the superior vena cava in a young woman with lupus nephritis on hemodialysis
Infectious complications are the main reason for medical consultations and hospital admissions1and are the second most frequent cause of mortality (next to cardiovascular events) in chronic kidney disease.2 Endocarditis is one of such complications, with a significantly higher prevalence and poorer prognosis in patients on hemodialysis compared with the general population.3
A 34‑year‑old woman with systemic lupus erythematosus, which led to chronic kidney disease stage 5 on chronic hemodialysis therapy with a 2‑year‑old tunneled catheter inserted into the right jugular vein, was admitted to the Department of Nephrology at the Jagiellonian University Medical College due to recurrent fever lasting 1 week. The patient had been hospitalized for the previous 2 months due to a catheter‑related infection confirmed by catheter tip cultures (Pseudomonas aeruginosa, Serratia marcescens). Transthoracic echocardiography did not reveal any significant abnormalities. The patient recovered after pharmacologic treatment and explantation of the infected catheter.
On admission, the patient was stable, afebrile, and complained of weakness and fatigue. Laboratory tests revealed moderate anemia, mild thrombocytopenia, and moderately elevated C‑reactive protein levels. Considering the fever episodes, recent recovery from the catheter‑related infection, and increased levels of inflammatory markers, blood cultures were obtained and an antibiotic treatment was administered according to the last antimicrobial resistance test results.
Transthoracic echocardiography raised a suspicion of a vegetation attached to the catheter. Transesophageal echocardiography confirmed a mobile, friable mass attached to the right atrium and catheter. Another such mass was found at the tip of the catheter (Figure 1A-1C).
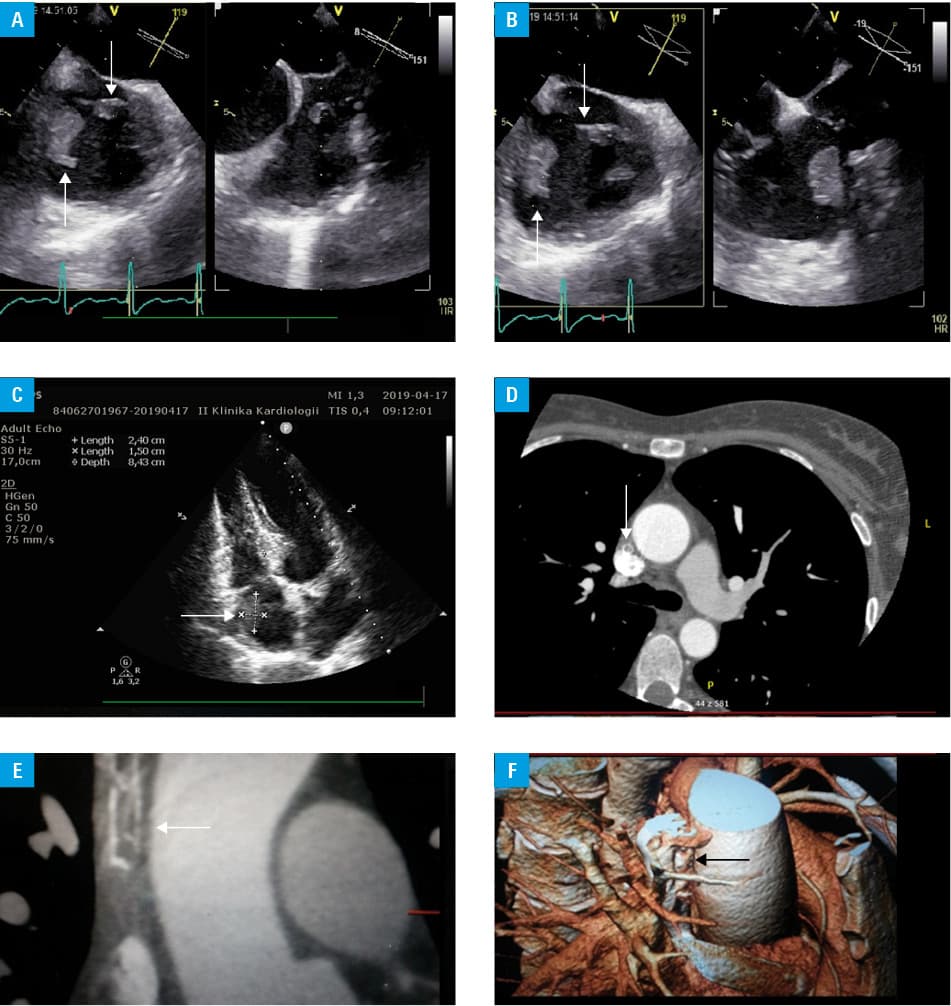
Infective endocarditis was diagnosed and the infected catheter was urgently removed. Antibiotic therapy was intensified and the dose of low‑molecular‑weight heparin was increased. Hemodialysis was continued using a temporary catheter inserted into the right femoral vein. Blood and catheter‑tip cultures were negative (probably due to the antibiotic treatment prior to admission); however, C‑reactive protein levels remained increased. The therapy was complicated by severe thrombocytopenia (probably induced by rifampicin administration), requiring several platelet transfusions and steroid pulses. The case was consulted twice during case conferences with cardiologists and cardiac surgeons. Owing to a high risk of intraoperative death, conservative management was recommended. Subsequently, magnetic resonance imaging was performed, which revealed an irregular mass with a lipomatous component in the right atrium (26 × 17 × 18 mm in size), tightly attached to its inferior wall. A tubular structure in the superior vena cava (8 mm in diameter), resembling a fragment of the catheter, was also described. This finding was confirmed by computed tomography angiography. The patient was consulted by a vascular surgeon, who concluded that the tubular structure was suggestive of a calcification within a thrombus and not of a broken part of the catheter (Figure 1D-1F). Surgery was not indicated and conservative treatment was implemented, resulting in normalization of inflammatory parameters. Echocardiography revealed that the lesion remained stationary.
In our case, recurrent infections were caused by an intravenous catheter, ultimately leading to a severe complication of infective endocarditis. As vascular calcifications are extremely rare, our finding is very uncommon. In our case, the calcification was misidentified as a fragment of the catheter. Similar misidentifications might have significant clinical implications; therefore, it is important to increase the awareness of such pathologies.4
- Reichert J. Hospital admissions and consultations in a dialysis population . Nefrologia. 2007; 27: 53‑61.
- Kumbar L, Yee J. Current concepts in hemodialysis vascular access infections. Adv Chronic Kidney Dis. 2019; 26: 16‑22. | Crossref
- Jones DA, McGill LA, Rathod KS, et al. Characteristics and outcomes of dialysis patients with infective endocarditis. Nephron Clin Pract. 2013; 123: 151‑156. | Crossref
- Capitanini A, Ricci E, Frosini P, Cupisti A. Massively calcified intravascular cast after removal of a tunneled central vein catheter for hemodialysis. J Vasc Access. 2013; 14: 196‑198. | Crossref
ARTICLE INFORMATION