Pericardial empyema due to Actinomyces israelii, Aggregatibacter actinomycetemcomitans, and Fusobacterium nucleatum



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Pericardial empyema due to Actinomyces israelii, Aggregatibacter actinomycetemcomitans, and Fusobacterium nucleatum
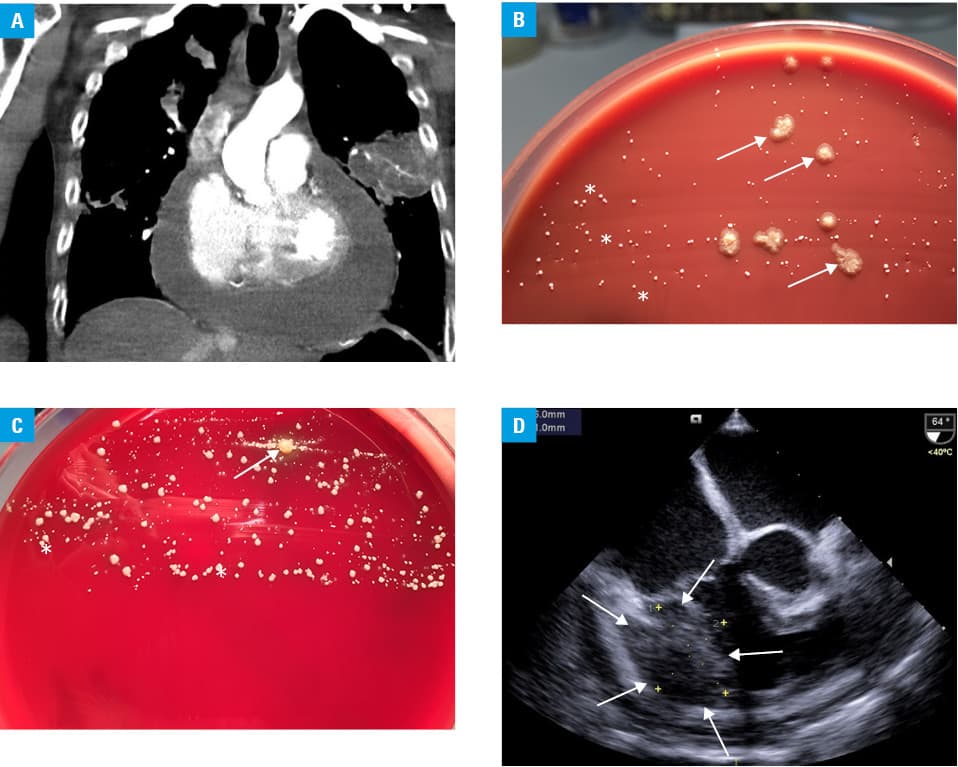
Pericardial empyema is observed in about 1% of all cases of pericarditis. Staphylococci and streptococci are the most relevant pathogens, but anaerobic bacteria may also be present in dental or esophageal diseases.1 A 52‑year‑old man was admitted to our hospital after he had collapsed at home. He presented with dyspnea, blood pressure of 86/44 mm Hg, and oxygen saturation of 80% on supplemental oxygen delivered at a flow rate of 15 l/min via a nonrebreather mask, and thus required immediate endotracheal intubation, mechanical ventilation, and catecholamine therapy. Clinical examination showed extensive dental caries, jugular vein distention, and several injection marks on both arms, indicative of intravenous drug abuse. The medical history indicated that he was on opioid substitution treatment and suffered from recurring epileptic seizures. Computed tomography revealed caverns in both lungs and massive pericardial effusion (Figure 1A). Pericardiotomy and external drainage were performed and 1 l of pus was removed. Laboratory analysis showed a serum lactate level of 19 mmol/l (normal range, 0.5–2.2 mmol/l), a white blood cell count of 20.2 G/l (normal range, 4.4–11.3 G/l), a C‑reactive protein level of 132 mg/l (normal range, <5.0 mg/l), and a procalcitonin level of 0.27 ng/l (normal range, 0.00–0.50 ng/l). Initially, the patient scored 12 points on the Sequential Organ Failure Assessment (previously Sepsis‑related Organ Failure Assessment) score and received imipenem/cilastatin (1 g 4 times a day) and fosfomycin (4 g 3 times a day). Extensive microbiological examinations for mycobacteria, the polymerase chain reaction test for hepatitis B and HIV, urine and blood cultures, Ziehl–Neelsen‑stain, galactomannan test, and (1,3)-ß-D‑glucan assay were negative, whereas the polymerase chain reaction test for hepatitis C was positive. After 10 days of incubation, pericardial cultures ultimately revealed Actinomyces israelii, Aggregatibacter actinomycetemcomitans, and Fusobacterium nucleatum identified by the MALDI TOF mass spectrometer (VITEK MS, bioMérieux, Marcy l’ Étoile, France) (Figure 1B and 1C). Transesophageal echocardiography showed a large hypoechoic mass in the right ventricular wall, which was suggestive of myocardial abscess (Figure 1D). After multidisciplinary discussion, a conservative therapeutic strategy was chosen, as a surgery would have required use of prosthetic material that posed imminent risk of reinfection in the active intravenous drug user. Targeted antibiotic treatment including piperacillin/tazobactam (4.5 g 4 times a day) against the bacteria mentioned above and linezolid (600 mg 3 times a day) for a possible Enterococcus faecium infection in our critically ill patient with several vascular catheters in place led to clinical improvement and the patient was successfully weaned from the ventilator after 38 days. He was mobilized and discharged from the cardiac intensive care unit on day 43. However, the patient died on day 50 due to an intractable epileptic seizure. Cranial computed tomography scans on days 8 and 48 showed no signs of territorial ischemia, masses or intracranial hemorrhage and no signs of intracranial abscesses, epidural or subdural infections, respectively. To our knowledge, this is the first published report of a severe cardiac infection with A. israelii, A. actinomycetemcomitans, and F. nucleatum. The source of infection remains unclear, but our patient had poor dental hygiene, and the 3 cultivated bacteria resembled components of the oral microbial flora. F. nucleatum can be found in periodontal plaque and A. actinomycetemcomitans is associated with aggressive periodontitis.2,3 In a systemic infection, symptoms can initially be subtle, but a coinfection with multiple anaerobic bacteria increases virulence.3,4 Notably, A. actinomycetemcomitans and A. israelii are difficult to cultivate and up to 4 weeks of incubation may be necessary.5 As our patient had a history of intravenous drug abuse, it should be considered that some drug users lick their needles before injection, allowing the mouth‑to‑vein transmission of bacteria. In summary, rare causes of a cardiac infection should be considered in intravenous drug users and patients with severe dental diseases. Multimodal imaging and extensive microbiological diagnostics with prolonged cultivation periods should be pursued in those patients—especially in the presence of septic shock—to allow for targeted antibiotic treatment.
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by: The European Association for Cardio‑Thoracic Surgery (EACTS). Eur Heart J. 2015; 36: 2921‑2964. | Crossref
- Nohrström E, Mattila T, Pettilä V, et al. Clinical spectrum of bacteraemic Fusobacterium infections: from septic shock to nosocomial bacteraemia. Scand J Infect Dis. 2011; 43: 463‑470. | Crossref
- Zijlstra EE, Swart GR, Godfroy FJ, Degener JE. Pericarditis, pneumonia and brain abscess due to a combined Actinomyces ‑ Actinobacillus actinomycetemcomitans infection. J Infect. 1992; 25: 83‑87. | Crossref
- Yang CC, Ye JJ, Hsu PC, et al. Characteristics and outcomes of Fusobacterium nucleatum bacteremia ‑ a 6‑year experience at a tertiary care hospital in northern Taiwan. Diagn Microbiol Infect Dis. 2011; 70: 167‑174. | Crossref
- Julian KG, de Flesco L, Clarke LE, Parent LJ. Actinomyces viscosus endocarditis requiring aortic valve replacement. J Infect. 2005; 50: 359‑362. | Crossref
ARTICLE INFORMATION