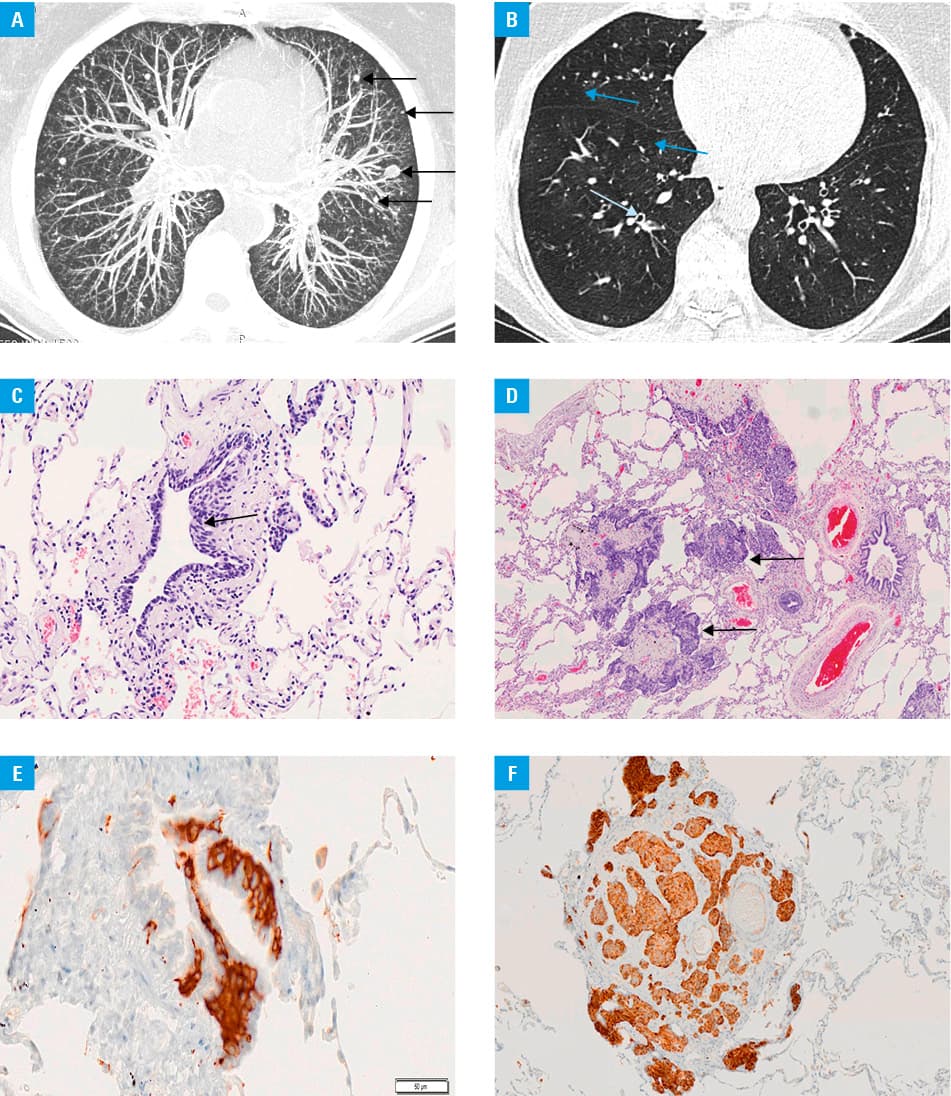
A 63‑year‑old woman, an ex‑smoker (15 pack‑years) with a 30‑year history of a dry cough diagnosed as bronchial asthma, was admitted in good general condition to our hospital because of multiple lung nodules on a chest X‑ray. Computed tomography of the chest (Figure 1A and 1B) revealed multiple, small, randomly distributed, bilateral nodules, and a diffuse, mosaic lung pattern featuring air‑trapping and bronchial wall thickening but without enlargement of the hilar or mediastinal lymph nodes. Routine laboratory test results, serum concentrations of cancer antigens CA72–4 and CA19–9, and neuron‑specific enolase levels were within normal limits. Pulmonary function tests demonstrated mild reversible obturation. Bronchoscopy revealed a normal bronchial tree. Microbiological cultures of bronchial washings were negative, and no Mycobacterium tuberculosis DNA was found. Cytological assessments were also negative. Transbronchial lung biopsy was not preformed because of the patient’s continuous cough. She underwent video‑assisted thoracoscopy. Histological examination of lung specimens revealed multiple foci of neuroendocrine cell hyperplasia, tumorlets, and typical carcinoid nodules of up to 8 mm in diameter, but these lacked necrosis and exhibited a low mitotic rate (2 FP/10 high‑power fields) (Figure 1C and 1D). Immunohistochemical staining revealed areas focally positive for cytokeratin, and diffuse positive reaction for synaptophysin (Figure 1E and 1F), chromogranin A, and TTF‑1. The Ki‑67 antigen index was 2%. We diagnosed diffuse, idiopathic, pulmonary neuroendocrine cell hyperplasia (DIPNECH). Inhaler therapy featuring long‑acting β-agonists and steroids was recommended. No disease progression has been observed during 3 years of follow‑up.
DIPNECH is extremely rare.1-5 Pulmonary neuroendocrine cell hyperplasia can be either primary or reactive. The reactive form is a nonneoplastic condition caused by chronic hypoxia‑associated disorders such as chronic obstructive pulmonary disease and interstitial pulmonary fibrosis. The term DIPNECH is used when diffuse pulmonary neuroendocrine cell hyperplasia occurs without any underlying disease. The World Health Organization defines DIPNECH as a generalized proliferation of pulmonary neuroendocrine cells confined to the airway epithelium or invading beyond the basement membrane, with formation of tumorlets (diameter <5 mm) or carcinoid tumors (diameter >5 mm); it is a preinvasive neoplastic lesion.1Two types of clinical presentation have been described.2 The first encompasses incidental pathologic findings in asymptomatic patients undergoing lobectomy or wedge lung resection, especially those with peripheral carcinoid tumors. The second is DIPNECH syndrome3 patients are symptomatic, usually over 50 years of age, commonly female (~90%), and usually nonsmokers (~70%) with a chronic nonproductive cough and dyspnea and (less commonly) wheezing, a productive cough, hemoptysis, and chest pain.4Pulmonary function tests reveal mild or moderate airflow obstruction. Chest computed tomography images reveal multiple nodules that vary in size and exhibit a random or centrilobular distribution, a diffuse mosaic lung pattern with air‑trapping, and (less commonly) bronchiectases, bronchial wall thickening, and atelectasis.4 Lung biopsy remains the gold standard for the diagnosis of DIPNECH. No evidence‑based management guidelines are available. Oral and inhaled steroids, azithromycin, somatostatin analogs, inhibitors of the mechanistic target of rapamycin, surgical lung resection, and lung transplantation have all been employed.5
- Gosney JR, Austin JHM, Jett J. Diffuse pulmonary neuroendocrine cell hyperplasia. In: Travis WD, Brambilla E, Burke AP, et al, eds. WHO classification of tumours of the lung, pleura, thymus and heart. Lyon, France: IARC Press; 2015: 78‑79.
- Mengoli MC, Rossi G, Cavazza A, et al. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) syndrome and carcinoid tumors with/without NECH: a clinicopathologic, radiologic, and immunomolecular comparison study. Am J Surg Pathol. 2018; 42: 646‑655. | Crossref
- Rossi G, Cavazza A, Spagnolo P, et al. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J. 2016; 47: 1829‑1841. | Crossref
- Chassagnon G, Favelle O, Marchand‑Adam S, et al. DIPNECH: when to suggest this diagnosis on CT. Clin Radiol. 2015; 70: 317‑325. | Crossref
- Myint ZW, McCormick J, Chauhan A, et al. Management of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: review and a single center experience. Lung. 2018; 196: 577‑581. | Crossref
ARTICLE INFORMATION