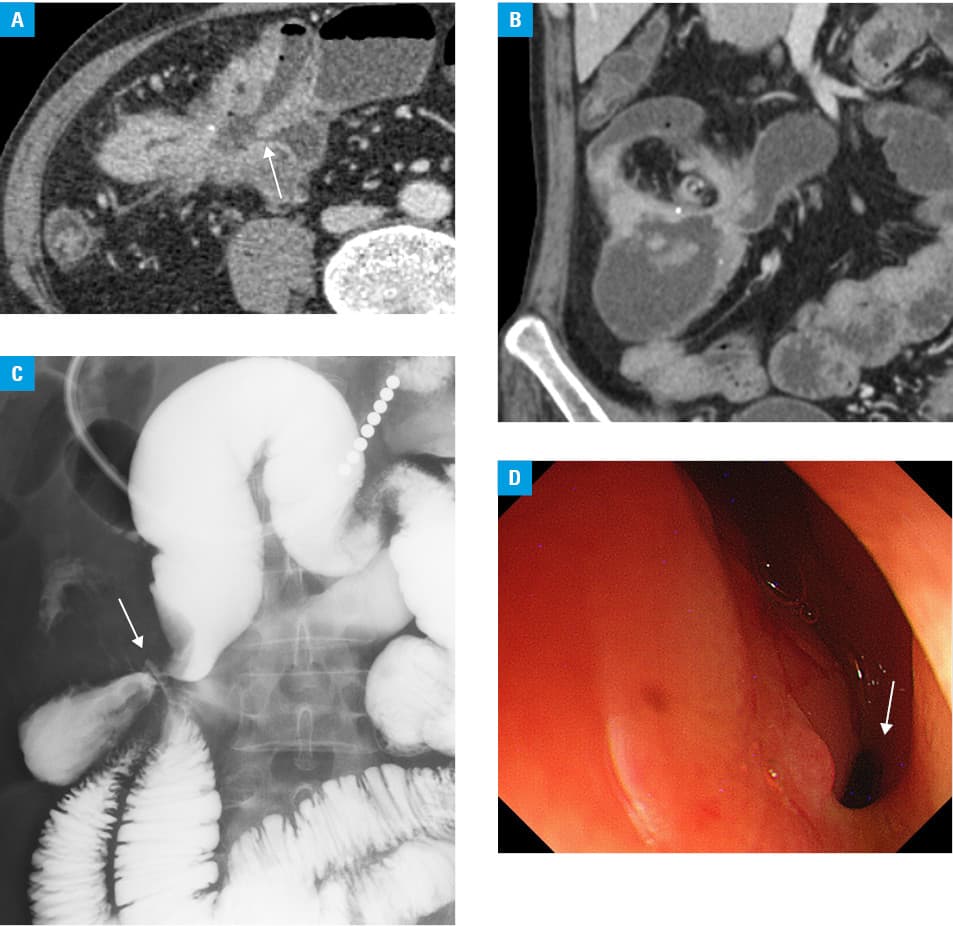
A 51‑year‑old man with a 10‑year history of ileocolonic Crohn disease (CD) presented with general fatigue and body weight loss. Past history included partial resection of the ileum and sigmoid colon due to an ileosigmoid fistula at the age of 42 years. He had been treated with infliximab for 6 years until its adverse effect, peripheral neuritis, occurred at the age of 49 years. Physical examination revealed a decreased body mass index of 16 kg/m2 and leg edema. The abdomen was not tender, with increased bowel sounds. Complete blood cell count showed a white blood cell count of 9100/mm3 and hemoglobin levels of 9.5 g/dl. Biochemical tests revealed elevated levels of C‑reactive protein (5.93 mg/dl; reference range, <0.14 mg/dl), erythrocyte sedimentation rate (97 mm/h; reference range, 2–10 mm/h), and markedly reduced albumin levels (1.8 g/dl; reference range, 4.1–5.1 g/dl). An axial computed tomography (CT) scan showed enteroenteric fistulas and marked thickening of the bowel wall (Figure 1A). A coronal CT scan disclosed complex fistulas with a star‑like configuration of dilated bowel loops (Figure 1B). Small‑bowel follow-through examination with diatrizoate meglumine (Gastrografin) revealed multiple ileocolic and ileoileal fistulas with markedly dilated bowel loops, resembling clover leaves (Figure 1C). Colonoscopy confirmed the opening of the fistula at the stricture site of the transverse colon (Figure 1D). The patient underwent right hemicolectomy and partial ileostomy. His symptoms and nutritional status improved, and ustekinumab was administered, resulting in clinical remission for 2 years.
Crohn disease causes deep transmural ulcerations. Small‑bowel fistulas occur in 10% to 20% of patients and are due to the extension of the deep ulcers beyond the bowel wall to bypass a distal luminal obstruction.1 The European guidelines have indicated that cross‑sectional imaging, such as CT and magnetic resonance imaging, has a pivotal role in the assessment of penetrating complications of CD.2 Magnetic resonance enterography and magnetic resonance enteroclysis have been proved effective in the depiction of internal fistulas with the characteristic star sign in CD.3,4 Although small‑bowel follow‑through examination is associated with radiation exposure, it can be useful in the clear detection of whole fistulas in a single image, as in this case. The typical radiologic signs of CD include a linear ulceration, cobblestone pattern, string sign, comb sign, and target sign.1 With the characteristic features detected by the small‑bowel follow‑through examination in this case, we propose the concept of the “clover sign”, that is, the clover leaf–like arrangement of bowel loops that converge to the central point of a fistula. The “clover sign” observed upon the small‑bowel follow‑through examination may be synonymous to the star sign and indicative of internal fistulas in patients with CD. Finally, this sign may aid the diagnosis of internal fistulas, one of the troublesome complications in CD.
- Carbo AI, Reddy T, Gates T, et al. The most characteristic lesions and radiologic signs of Crohn disease of the small bowel: air enteroclysis, MDCT, endoscopy, and pathology. Abdom Imaging. 2014; 39: 215‑234. | Crossref
- Maaser C, Sturm A, Vavricka SR, et al. ECCO‑ESGAR Guideline for diagnostic assessment in IBD Part 1: initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019; 13: 144‑164. | Crossref
- Herrmann KA, Michaely HJ, Zech CJ, et al. Internal fistulas in Crohn disease: magnetic resonance enteroclysis. Abdom Imaging. 2006; 31: 675‑687. | Crossref
- Tolan DJ, Greenhalgh R, Zealley IA, et al. MR enterographic manifestations of small bowel Crohn disease. Radiographics. 2010; 30: 367‑384. | Crossref
ARTICLE INFORMATION