Assessment of patients with coronary artery disease who may benefit from the use of rivaroxaban in the real world: implementation of the COMPASS trial criteria in the TERCET registry population
Key words: COMPASS trial, coronary artery disease, external applicability, TERCET registry



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Assessment of patients with coronary artery disease who may benefit from the use of rivaroxaban in the real world: implementation of the COMPASS trial criteria in the TERCET registry population
Introduction: The positive outcomes of the COMPASS trial raise questions about the proportion of patients who could benefit from additional therapy with rivaroxaban in real‑world practice.
Objectives: We aimed to identify the proportion of patients from the TERCET registry with significant coronary artery disease (TERCET‑CAD) who could benefit from the use of rivaroxaban and to assess their clinical characteristics and long‑term prognosis in comparison with the corresponding measures in the COMPASS trial.
Patients and methods: The COMPASS criteria were applied in the TERCET‑CAD population. Patients who met the criteria of the COMPASS trial were included in the COMPASS‑like group. The baseline characteristics and long‑term outcomes of the COMPASS‑like group were compared with the corresponding measures in the acetylsalicylic acid (ASA)–alone arm from the COMPASS trial.
Results: The COMPASS‑like group included 3884 patients (31.6%) out of the 12286 patients constituting the TERCET‑CAD population. Patients in the COMPASS‑like group were characterized by older age (P <0.001) and a more frequent occurrence of risk factors for CAD than those in the ASA‑alone arm of the COMPASS trial. The rate of a composite endpoint in the COMPASS‑like group was 9%, and in the ASA‑alone arm of the COMPASS trial, it was 6% (P <0.001).
Conclusions: Less than one‑third of the TERCET‑CAD population met the COMPASS criteria and could potentially benefit from low‑dose rivaroxaban therapy. Unfavorable clinical profiles and higher rates of adverse events in the TERCET registry compared with those in the COMPASS trial may predict greater benefits from the implementation of low‑dose rivaroxaban in the real‑world population.
Introduction
Despite the introduction of novel pharmacotherapy and the widespread use of revascularization, stable coronary artery disease (CAD) is still the most common cause of mortality and morbidity in the general population.1-3 Patients with a diagnosis of stable CAD are at risk of adverse ischemic events and, as a consequence, cardiovascular death.4-6 Given the activation of platelets and the coagulation cascade in atherosclerosis,7 one of the directions of contemporary research in stable CAD is the evaluation of adding various antithrombotic therapies to acetylsalicylic acid (ASA) for tertiary prevention.8,9 Previous randomized controlled trials (RCTs) did not confirm that the additional use of clopidogrel,10 ticagrelor,11 vorapaxar,12 or vitamin K antagonists13 in patients with stable CAD was associated with measurable benefits as compared with antithrombotic therapy limited to ASA. Recently, the results of the international, multicenter, randomized COMPASS trial (Cardiovascular Outcomes for People using Anticoagulation Strategies; ClinicalTrials.gov number: NCT0177424) have indicated that adding low‑dose rivaroxaban (2.5 mg twice daily) to ASA improves long‑term outcomes in a selected population of patients with stable CAD.14-16
As with any RCT,17-19 strict inclusion and exclusion criteria may cause difficulties in implementing the results from the COMPASS trial across the full spectrum of patients with stable CAD.14 Patients enrolled in RCTs often have a lower cardiovascular risk than a real‑world population,20-22 which may also affect the benefits and risks of applying novel technologies or drugs.17,19 Therefore, the positive outcomes of the COMPASS trial raise questions about the proportion of patients who could benefit from additional therapy with low‑dose rivaroxaban in routine clinical practice. Current guidelines of the European Society of Cardiology (ESC) emphasize the necessity of obtaining evidence from unselected patients and validated registries in order to apply the results of RCTs to real‑world practice.23-25
Data from the TERCET registry (Hyperlipidemia Therapy in the Tertiary Cardiological Center),26 encompassing a population with CAD, allow an analysis of the proportion of patients who could benefit from the use of rivaroxaban as well as an assessment of their clinical characteristics and long‑term prognosis in comparison with patients included in the COMPASS trial.
Patients and methods
The COMPASS trial The design14 and outcomes15 of the COMPASS trial were described previously. In brief, the COMPASS trial was a double‑blind, placebo‑controlled, randomized trial of 27395 patients with stable CAD or peripheral vascular disease. The study population was randomly assigned into the following 3 arms of antithrombotic strategies: rivaroxaban (2.5 mg twice daily) plus ASA, rivaroxaban alone (5 mg twice daily), or ASA alone. Of the total number of patients enrolled in the COMPASS trial, 24824 (91%) had stable CAD (COMPASS‑CAD substudy).16 During the mean 23 months of follow‑up, the combination of rivaroxaban and ASA was associated with a significant 26% reduction of the primary endpoint in comparison with that in the control arms. Moreover, the regimen resulted in more frequent major bleeding compared with the ASA‑alone arm, but without a significant increase in the rates of intracranial or life‑threatening bleeding.
The TERCET registry
The design of the TERCET registry was described previously.26 Briefly, the registry is a prospective, observational study recruiting consecutive patients with ischemic heart disease (stable angina and acute coronary syndromes) hospitalized in a tertiary cardiology center with an on‑site cardiac surgery facility.
The primary outcome measure of the TERCET registry is the evaluation of the effect of treatment on the lipid profile and long‑term prognosis of patients with ischemic heart disease. The diagnosis of CAD was established on the basis of clinical presentation, coronary angiography, and additional test results, in accordance with current ESC guidelines.23-25 Patients with vasospastic or microvascular angina were also included in the registry. Diagnostic and therapeutic strategies, including pharmacologic and interventional treatment, were used in accordance with the current ESC guidelines.23-25 Each patient enrolled in the TERCET registry underwent coronary angiography. The data on long‑term follow‑up, including the cause of death and the exact date of death and cardiovascular events, were obtained from the official registry of the National Health Fund, which ensured complete data collection. According to the International Classification of Diseases, Tenth Revision, myocardial infarction (MI) was defined as the I21–I22 codes, whereas stroke was defined as the I60–I64 codes. Follow‑up was available for all patients. The TERCET registry has been approved by the institutional review board and has been conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The trial is registered at www.clinicaltrials.gov (ID: NCT0306543).
TERCET‑CAD population
For the purpose of the present study, of all patients enrolled in the TERCET registry and hospitalized between 2006 and 2016, only stable patients (with stable angina or 1 year after an acute coronary syndrome) with significant CAD were included. Significant CAD was defined as a history of MI, percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG); ≥50% stenosis of the left main (LM) branch or the proximal segment of the left anterior descending branch of the left coronary artery; or ≥70% stenosis in other segments of the coronary arteries. Patients for whom data on the parameters listed in the COMPASS criteria were unavailable (n = 1887) were not included in the present analysis (Supplementary Material, Table S1). The remaining patients constituted the TERCET‑CAD population.
Application of COMPASS criteria in the TERCET‑CAD population
First, we applied the COMPASS inclusion criteria14 to the TERCET‑CAD population (Figure 1): 1) CAD according to the COMPASS criteria was defined as the occurrence of one of the following: MI within the last 20 years; multivessel CAD with symptoms or with a history of stable or unstable angina; multivessel PCI; or multivessel CABG surgery; 2) patients who met the above criteria also had to meet at least 1 of the following criteria: age ≥65 years or age <65 years and documented atherosclerosis or revascularization involving at least 2 vascular beds (the aorta, arterial supply to the brain, gastrointestinal tract, lower limbs, upper limbs, kidneys) or at least 2 additional risk factors (current smoking, diabetes mellitus, renal dysfunction with estimated glomerular filtration rate <60 ml/min, heart failure, or ischemic stroke ≥1 month prior to inclusion). TERCET‑CAD patients who did not meet the above inclusion criteria of the COMPASS trial were assigned to the COMPASS‑not‑included group.
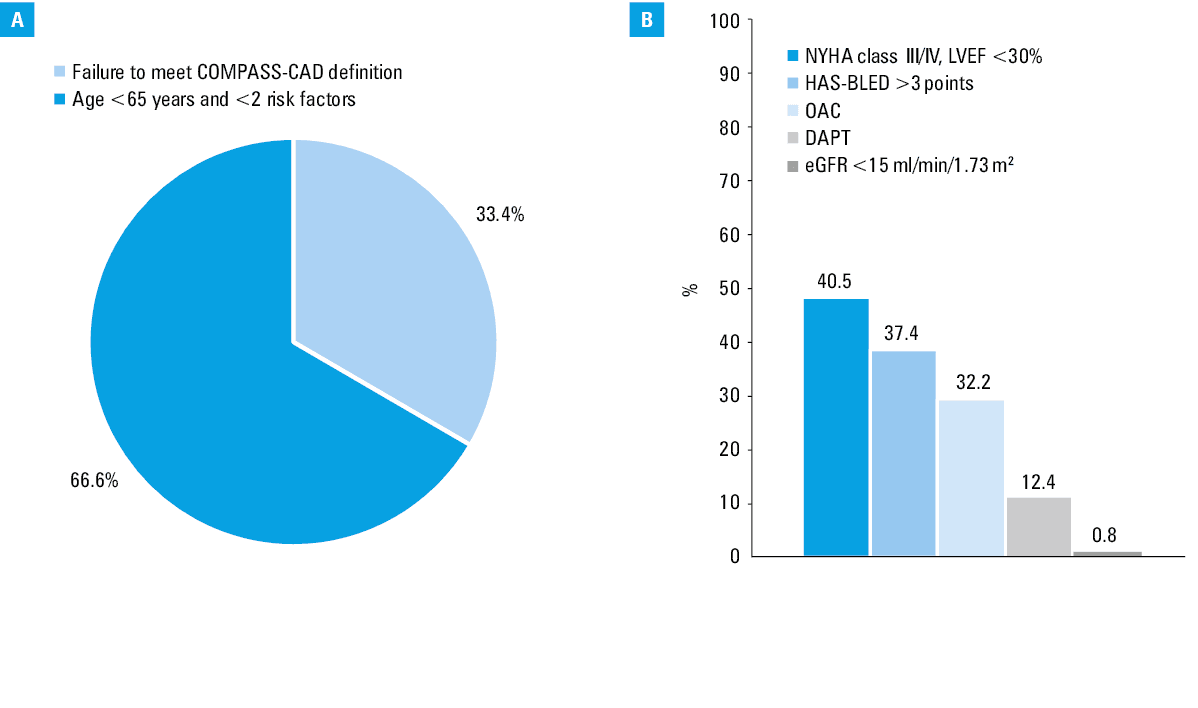
![Percentage of the TERCET-CAD population who did not fulfill the inclusion criteria (A; COMPASS-not-included group [n = 5177; 42.1%]) and who met the exclusion criteria of the COMPASS trial (B; COMPASS-excluded group [n = 3225; 26.2%])Abbreviations: HAS-BLED, hypertension, abnormal liver function, history of stroke or thromboembolism, history of bleeding, age >65 years, use of nonsteroidal anti-inflammatory drugs, and alcohol abuse; others, see Figure 1](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F14907%2FIMAGES%2FPAMW_WEB__PAMW-D-19-00132_orig__FIG_01__PAGE_462.png&w=3840&q=75)
Subsequently, among the remaining TERCET‑CAD population, the following exclusion criteria of the COMPASS trial14 were applied: 1) high risk of bleeding; 2) stroke within the previous month or a history of hemorrhagic or lacunar stroke; 3) severe heart failure with known ejection fraction of less than 30% or New York Heart Association (NYHA) class III or IV symptoms; 4) an estimated glomerular filtration rate of less than 15 ml/min; 5) a need for dual antiplatelet therapy, other non‑ASA antiplatelet therapy, or oral anticoagulant therapy; 6) known noncardiovascular disease that is associated with poor prognosis (eg, metastatic cancer); 7) history of hypersensitivity or a known contraindication to rivaroxaban, ASA, or excipients, if applicable; and 8) other exclusion criteria of the COMPASS trial.
The remaining TERCET‑CAD patients who met at least 1 of the above exclusion criteria of the COMPASS trial were assigned to the COMPASS‑excluded group.
Patients from the TERCET‑CAD population who met the inclusion criteria and did not meet the exclusion criteria of the COMPASS trial were the target study group, namely, the COMPASS‑like group.
The data available in the TERCET registry allow defining all the inclusion and exclusion criteria as in the COMPASS trial, with a few exceptions. First, chronic heart failure in the TERCET registry was defined as the presence of left ventricular dysfunction with a left ventricular ejection fraction of 35% or lower or a previous implantation of an implantable cardioverter‑defibrillator as part of the primary prevention of sudden cardiac death (except for patients with a documented diagnosis of hypertrophic cardiomyopathy). In the COMPASS trial, chronic heart failure was determined based on a clinical diagnosis in the patient’s medical history.14,15 Additionally, in the TERCET registry, the high risk of bleeding was based on the HAS‑BLED score (hypertension, abnormal liver function, history of stroke or thromboembolism, history of bleeding, age >65 years, use of nonsteroidal anti‑inflammatory drugs, and alcohol abuse) (high risk of bleeding ≥3 points).27 In the COMPASS trial, the assessment of the high risk of bleeding was at the discretion of the investigator. The exclusion criterion of hypersensitivity or known contraindications to the use of drugs was limited either to rivaroxaban or ASA, without considering pantoprazole (whose administration in the COMPASS trial was also assessed).14
Primary outcome measure
The primary endpoint in the COMPASS trial was a composite of cardiovascular death, stroke, or MI.14 The study was stopped because of the superiority of the rivaroxaban‑plus‑ASA group after a mean follow‑up of 23 months.15,16 In the TERCET registry, due to the lack of information on the cause of death, all‑cause death in the composite endpoint at the 24‑month follow‑up was used.
Statistical analysis
To compare the baseline characteristics and long‑term outcomes between the COMPASS‑like group from the TERCET‑CAD population and the ASA‑alone arm from the COMPASS‑CAD substudy, the t test for continuous variables and the χ2 test for categorical variables were used. Continuous variables were presented using the arithmetic mean with SD or median with the first and third quartiles. A 2‑sided P value of less than 0.05 was considered significant. The STATISTICA 10 software (StatSoft, Inc., Tulsa, Oklahoma, United States) was used for all calculations.
Results
Identification of the COMPASS‑like group
A flow chart for the identification of patients meeting the COMPASS criteria in the TERCET‑CAD population (the COMPASS‑like group) is presented in Figure 1. Among the 12286 patients of the TERCET‑CAD population, 7109 patients (57.9% of the entire population) met the inclusion criteria of the COMPASS trial. The remaining 5177 patients (42.1% of the entire population) did not meet the COMPASS inclusion criteria (the COMPASS‑not‑included group).
As the next step, the exclusion criteria of the COMPASS study were applied across the 7109 patients in the TERCET‑CAD population who met the inclusion criteria. Based on these criteria, 3225 patients (26.2% of the entire population) excluded from further analysis were assigned to the COMPASS‑excluded group. After implementation of the inclusion and exclusion criteria, the remaining 3884 patients (31.6% of the entire population) constituted a study group that would potentially meet the COMPASS criteria in the TERCET‑CAD population (the COMPASS‑like group).
COMPASS criteria in the TERCET‑CAD population
The percentage of the TERCET‑CAD population who did not fulfill the inclusion criteria and who met the exclusion criteria of the COMPASS trial depending on the reasons is presented in Figure 2.
COMPASS‑like group in the TERCET‑CAD population vs the ASA‑alone arm of the COMPASS trial A comparison of the COMPASS‑like group in the TERCET‑CAD population with the ASA‑alone arm of the COMPASS trial is presented in Tables 1 and 2. Patients in the COMPASS‑like group were older and were more often male than those in the ASA‑alone arm. Moreover, they more often had diabetes mellitus, arterial hypertension, and prior PCI. On the other hand, peripheral vascular disease and chronic heart failure were less prevalent in this group. Regarding medical therapy, angiotensin‑converting enzyme inhibitors, angiotensin II receptor antagonists, statins, and β-blockers were used more frequently in the COMPASS‑like group in comparison with the ASA‑alone arm of the COMPASS trial.
Variable | COMPASS‑like group (n = 3884) | ASA‑alone arm (n = 8261) | P value | ||
Data are presented as number (percentage) of patients unless otherwise indicated.
a For the COMPASS‑like group, chronic heart failure was defined as left ventricular ejection fraction ≤35% or a history of implantation of an implantable cardioverter-defibrillator for primary prevention of sudden cardiac death (excluding hypertrophic cardiomyopathy).
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; ASA, acetylsalicylic acid; others see Figure 1 | |||||
Age, y, median (Q1–Q3) | 70 (65–75) | 69 (65–73) | <0.001 | ||
Sex | Female | 1252 (32) | 1646 (20) | <0.001 | |
Male | 2632 (68) | 6615 (80) | <0.001 | ||
Body mass index, kg/m2, mean (SD) | 28.4 (4.4) | 28.5 (4.7) | 0.26 | ||
eGFR, ml/min/1.73 m2, mean (SD) | 79.7 (23.8) | 73.7 (17.9) | <0.001 | ||
Systolic blood pressure, mm Hg, mean (SD) | 133 (18) | 135 (17) | <0.001 | ||
Diastolic blood pressure, mm Hg, mean (SD) | 78 (11) | 78 (10) | 0.92 | ||
Risk factors | Current smoking | 956 (25) | 1687 (20) | <0.001 | |
Former smoking | 1762 (45) | 3908 (47) | 0.046 | ||
Diabetes mellitus | 1629 (42) | 3040 (37) | <0.001 | ||
Arterial hypertension | 3057 (79) | 6218 (75) | <0.001 | ||
Peripheral artery disease | 654 (17) | 1641 (20) | <0.001 | ||
Previous MI | 2673 (69) | 5721 (69) | 0.64 | ||
PCI | 3168 (82) | 4905 (59) | <0.001 | ||
Previous CABG | 1231 (32) | 2586 (31) | 0.67 | ||
Multivessel CAD | 2423 (62) | 5043 (61) | 0.16 | ||
Chronic heart failurea | 437 (11) | 1,912 (23) | <0.001 | ||
Stroke | 109 (3) | 268 (3) | 0.19 | ||
Previous treatment | ACEI or ARB | 3452 (89) | 5939 (72) | <0.001 | |
Lipid‑lowering drug | 3548 (93) | 7573 (92) | 0.045 | ||
β-Blocker | 3641 (94) | 6154 (75) | <0.001 | ||
Eastern European ethnicity | 3884 (100) | 1487 (18) | <0.001 | ||
Variable | COMPASS‑like group (n = 3884) | ASA‑alone arm (n = 8261) | P value |
Data are presented as number (percentage) of patients.
a For the COMPASS‑like group, owing to the lack of information about the cause of death, all‑cause death was used.
| |||
MI, stroke, or cardiovascular deatha | 360 (9) | 460 (6) | <0.001 |
Death | 217 (6) | 339 (4) | <0.001 |
MI | 125 (3) | 195 (2) | 0.01 |
Stroke | 62 (2) | 130 (2) | 0.93 |
Coronary revascularization | 262 (7) | 553 (7) | 0.92 |
In the TERCET‑CAD registry, the follow‑up was 24 months and was completed for all patients, whereas in the COMPASS trial, the mean follow‑up was 23 months. The rate of the composite endpoint in the COMPASS‑like group was 9% (all‑cause death, MI, or stroke), and in the ASA‑alone arm of the COMPASS trial, it was 6% (cardiovascular death, MI, or stroke; P <0.0001). In addition, in the COMPASS‑like group, all‑cause death (6% vs 4%; P <0.0001) and incidence of MI (3% vs 2%; P = 0.01) were more frequent than in the ASA‑alone arm of the COMPASS trial. There were no differences between groups in other adverse cardiovascular events, such as stroke (2% vs 2%; P = 0.93) or revascularization (7% vs 7%; P = 0.92).
Comparison of the COMPASS‑like, COMPASS‑not‑included, and COMPASS‑excluded groups
The baseline characteristics and long‑term outcomes of the COMPASS‑like, the COMPASS‑not‑included, and the COMPASS‑excluded groups are shown in Table 3. In general, the COMPASS‑not‑included group was characterized by a lower incidence of risk factors for CAD and comorbidities as well as the most favorable long‑term prognosis than the remaining groups. Conversely, patients in the COMPASS‑excluded group had the highest rate of risk factors and worse long‑term outcomes in comparison with the other groups.
Variable | COMPASS‑not‑included group (n = 5177; 42.1%) | COMPASS‑like group (n = 3884; 31.6%) | COMPASS‑excluded group (n = 3225; 26.2%) | ||
Data are presented as number (percentage) of patients unless otherwise indicated.
| |||||
Age, y, median (Q1–Q3) | 59 (55–64) | 70 (65–75) | 72 (67–77) | ||
Sex | Female, n (%) | 1407 (27) | 1252 (32) | 1070 (33) | |
Male, n (%) | 5177 (73) | 2632 (68) | 2155 (67) | ||
Body mass index, kg/m2, mean (SD) | 28.7 (4.5) | 28.4 (4.4) | 28.7 (4.7) | ||
eGFR, ml/min/1.73 m2, mean (SD) | 91.3 (23.6) | 79.7 (23.8) | 71.2 (24.7) | ||
Systolic blood pressure, mm Hg, mean (SD) | 136 (22) | 133 (18) | 141 (28) | ||
Diastolic blood pressure, mm Hg, mean (SD) | 81 (13) | 78 (11) | 81 (14) | ||
Risk factors | Current smoking | 1278 (25) | 956 (25) | 526 (16) | |
Former smoking | 2541 (49) | 1762 (45) | 1382 (43) | ||
Diabetes mellitus | 1236 (24) | 1629 (42) | 1526 (47) | ||
Arterial hypertension | 3772 (73) | 3057 (79) | 2691 (83) | ||
Peripheral artery disease | 223 (4) | 654 (17) | 865 (27) | ||
Previous MI | 2652 (51) | 2673 (69) | 2429 (75) | ||
PCI | 4332 (84) | 3168 (82) | 2677 (83) | ||
Previous CABG | 827 (16) | 1231 (32) | 949 (29) | ||
Multivessel CAD | 1627 (32) | 2423 (62) | 1941 (60) | ||
Chronic heart failure | 378 (7) | 437 (11) | 1169 (36) | ||
LVEF, % (SD) | 48.6 (9.2) | 46.9 (8.2) | 39.6 (12.5) | ||
Stroke | 110 (2) | 109 (3) | 542 (17) | ||
Previous treatment | ACEI or ARB | 4584 (89) | 3452 (89) | 2731 (85) | |
Lipid‑lowering drug | 4762 (93) | 3548 (93) | 2870 (91) | ||
β-Blocker | 4800 (93) | 3641 (94) | 3021 (94) | ||
MI, stroke, or cardiovascular death | 318 (6) | 360 (9) | 519 (16) | ||
Death | 189 (4) | 217 (6) | 373 (11) | ||
MI | 113 (2) | 125 (3) | 130 (4) | ||
Stroke | 38 (1) | 62 (2) | 85 (3) | ||
Coronary revascularization | 293 (6) | 262 (7) | 208 (6) | ||
Discussion
The results of our study showed that 31.6% of patients included in the large‑scale prospective TERCET registry of a real‑world population with CAD met the COMPASS trial criteria. The remaining patients were ineligible for further analysis as they did not meet the inclusion criteria or they fulfilled the exclusion criteria of the COMPASS trial.
The possibility of external applicability of the COMPASS trial criteria in 2 large‑scale international registries was analyzed previously.28,29 The first one, the REACH registry (Reduction of Atherothrombosis for Continued Health), included patients over 45 years of age with diagnosed atherosclerosis (CAD, peripheral or cerebral artery disease) or at least 3 risk factors for atherosclerosis.28 The COMPASS criteria were met by 53% of the analyzed population. The discrepancy in the result between the REACH registry and our study may be due to differences in the applied methodology. Firstly, the REACH registry used a less rigorous definition of CAD owing to the lack of accurate information on the number of treated vessels and the degree of atherosclerosis progression in the coronary arteries. In addition, the REACH registry lacked data on 7 exclusion criteria from the COMPASS trial, including severe heart failure (left ventricular ejection fraction <30%, NYHA functional class III or IV), history of cancer, or hypersensitivity to rivaroxaban and ASA. Finally, because of the lack of detailed recommendations in the COMPASS trial protocol on the definition of high risk of bleeding,14 the REACH bleeding risk score was used.30 The authors admit that the above limitations could lead to an overestimation of the percentage of patients that met the COMPASS criteria in the REACH registry.
External applicability of the COMPASS criteria to the real‑world population was also investigated in the FAST‑MI 2005, 2010, and 2015 registries, which included patients with a recent MI.29 For the purpose of adapting the methodology of the COMPASS trial, the FAST‑MI population was included for analysis 1 year (entry point) after MI. The COMPASS criteria applied in the FAST‑MI registries were met in 44% of the population. Notably, all patients had a previous MI, and as a consequence, they fulfilled the CAD definition according to the COMPASS trial.14 However, this (as well as the exclusion of patients with stable CAD in the FAST‑MI registries) may also have resulted in an overestimation of the percentage of patients who met the COMPASS criteria in the real‑world population. In contrast to the REACH and FAST‑MI registries, in the present study, we were able to precisely define the inclusion and exclusion criteria in an unselected population of patients with stable CAD confirmed by coronary angiography. Furthermore, due to the implementation of the widely used HAS‑BLED score, a high risk of bleeding was standardized.27
Despite a high level of evidence, results from RCTs are implemented into routine clinical practice with appropriate caution.17-19 Patients strictly recruited for RCTs are usually characterized by a lower cardiovascular risk than the real‑world population.20-22 Our study confirms this fact despite the use of comparable inclusion and exclusion criteria. The COMPASS‑like group in the TERCET‑CAD population was characterized by older age, a more frequent occurrence of risk factors for CAD, and a less favorable long‑term prognosis. Similar results were observed in the REACH and FAST‑MI registries.28,29 Differences in the baseline characteristics and long‑term outcomes between the real‑world population and participants of the COMPASS trial may suggest that the addition of rivaroxaban to tertiary prevention in routine clinical practice will result in even better treatment effects.
After discharge, TERCET‑CAD patients meeting the COMPASS criteria were characterized by a higher rate of the composite endpoint than those in the ASA‑alone arm of the COMPASS trial.16 There may be several reasons for the observed difference. First of all, as we had no information on the causes of death in our study, we applied the definition of all‑cause mortality. This is in contrast to the COMPASS trial, in which cardiovascular mortality was included in the composite endpoint. Moreover, the long‑term outcomes should be considered in the context of a worse clinical profile of the TERCET‑CAD population. The differences may also be caused by the fact that the participants of the COMPASS trial were closely followed after discharge from the hospital,14 which may have resulted in better compliance with medical recommendations and immediate medical care in the case of new symptoms.
In RCTs, the clinical profile and outcomes of patients meeting the inclusion and not meeting the exclusion criteria are usually not presented.17-19 In addition to the evaluation of eligibility in the real‑world population, the results of observational studies can often lead to formulation of new research hypotheses. Therefore, future research should focus on populations not included in clinical trials. In the context of the present study, the COMPASS‑not‑included group might have been expected to have the most favorable and the COMPASS‑excluded group to have the worst clinical profile and long‑term outcomes. It is also worth noting that, despite the more favorable characteristics of the COMPASS‑not‑included group, long‑term outcomes were similar to those in the ASA‑alone arm of the COMPASS trial.16 Considering the relatively rigorous CAD definition adopted in the COMPASS trial,14 it seems reasonable to conduct RCTs evaluating the benefits of using additional rivaroxaban therapy in a population with any significant CAD.
Study strengths and limitations
TERCET is a large‑scale, prospective registry of unselected patients with CAD confirmed by coronary angiography and with available follow‑up obtained from the National Health Fund (the only payer in Poland). In addition to the typical advantages and limitations associated with the registry design of the study, a few more comments should be made. The adopted definition of chronic heart failure was more detailed and the bleeding risk was higher in the TERCET registry than in the COMPASS trial.14 For the COMPASS trial, the recruitment was conducted from February 2013 to May 2016, while the TERCET registry included patients hospitalized between January 2006 and December 2016. The differences in the enrollment period and, in consequence, the implementation of different ESC recommendations, may have translated into differences in the distribution of risk factors, management, tertiary prevention, and outcomes.31 Therefore, the results of the present study should be interpreted with caution.
Conclusions
In summary, less than one‑third of the TERCET registry population with significant CAD met the COMPASS criteria and could potentially benefit from low‑dose rivaroxaban therapy. Unfavorable clinical profiles and the higher rate of adverse events in the TERCET registry compared with those in the COMPASS trial may result in greater benefits from the implementation of low‑dose rivaroxaban in the real‑world population. Therefore, there is a need for further clinical trials assessing the CAD population in routine clinical practice.
- Townsend N, Wilson L, Bhatnagar P, et al. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016; 37: 3232‑3245. | Crossref
- Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics‑2019 update: A report from the American Heart Association. Circulation. 2019; 139: e56‑e528.
- Top 10 causes of Death. World Health Organization. http://www.who.int/gho/mortality_burden_disease/causes_death/top_10/en/. Accessed April 13, 2019.
- Bhatt DL, Eagle KA, Ohman EM, et al. Comparative determinants of 4‑year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010; 304: 1350‑1357. | Crossref
- Parma Z, Steg PG, Greenlaw N, et al. Differences in outcomes in patients with stable coronary artery disease managed by cardiologists versus noncardiologists. Results from the international prospective CLARIFY registry. Pol Arch Intern Med. 2017; 127: 107‑114.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION