Bilateral Warthin tumor with a fibrous variant of chronic lymphocytic thyroiditis misdiagnosed as well-differentiated thyroid cancer with lymph node metastasis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Bilateral Warthin tumor with a fibrous variant of chronic lymphocytic thyroiditis misdiagnosed as well-differentiated thyroid cancer with lymph node metastasis
Warthin tumor (WT) is the second most common benign neoplasm among all parotid epithelial lesions.1 Approximately 15% to 20% of these tumors may be multifocal or bilateral and can thus be misinterpreted as metastasis to the neck lymph node.2 WT might be rarely located in the minor salivary and submandibular glands or even in the lymph nodes.3 When WT coexists with anatomical abnormalities of the head and neck, such as thyroid tumors, it may be misinterpreted as a metastatic disease.4
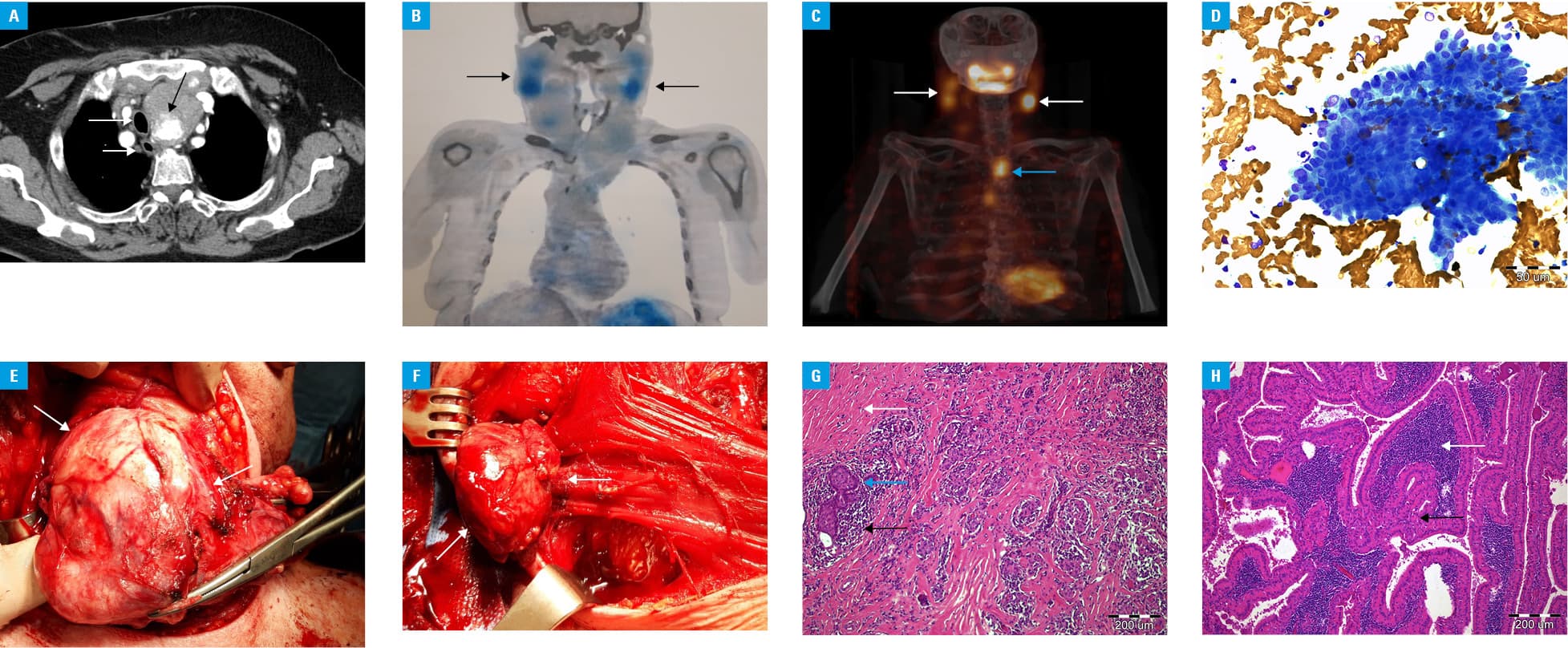
An 80‑year‑old woman, a heavy smoker, was admitted to the department of endocrinology due to suspected locally advanced thyroid cancer. She complained of rapid growth of the thyroid tumor, dyspnea, dysphagia, and weight loss. Physical examination revealed a large thyroid tumor, enlarged submandibular lymph nodes, and pain on the right side of the neck. Computed tomography revealed retrosternal thyroid tumors, as well as esophageal and tracheal compression with stenosis and lateral displacement (Figure 1A). Bilateral enlargement of the submandibular lymph nodes was also detected. Ultrasound of the neck confirmed thyroid tumors with heterogeneous, hypoechoic echotexture, ill‑defined margins, and an irregular contour with enlarged, hypoechoic submandibular lymph nodes. Laboratory tests revealed hypothyroidism, and treatment with levothyroxine was initiated. The serum calcitonin concentration was in the reference range, and antithyroid peroxidase and antithyroglobulin antibodies were positive, while antithyroid‑stimulating hormone receptor antibodies were negative. Single‑photon emission computed tomography confirmed significantly enlarged thyroid glands with submandibular metastatic nodules (Figure 1B). The right lobe was 2 cm below the suprasternal notch, and the left lobe reached the posterior mediastinum (Figure 1C). The ultrasound‑guided fine‑needle aspiration biopsy (UG‑FNAB) of the thyroid and submandibular tumors was performed but no sufficient material was obtained for examination. The clinical presentation and radiological findings suggested thyroid lymphoma; however, the results of bone marrow biopsy and needle aspiration were negative. The UG‑FNAB of the primary tumor and nodules in the upper neck was performed again. Based on cytology, the thyroid tumor was classified as category III according to the Bethesda System for Reporting Thyroid Cytopathology, and follicular cells resembling metastases were found in specimens from the neck lesions. To confirm the results of the cytological analysis,5 the final UG‑FNAB was performed and, in the end, category V was established. The smears of samples from the thyroid and lymph node showed a sparse and moderate number of cancer cells, respectively. Both smears displayed similar cytomorphologic characteristics of cancer cells, which raised suspicion of papillary thyroid carcinoma but were not sufficient for a conclusive diagnosis (Figure 1D). The patient was transferred to the department of surgery and underwent total thyroidectomy (Figure 1E) with bilateral selective lymphadenectomy (Figure 1F). The surgical specimen from the thyroid showed a nodular pattern of growth with associated fibrosis, chronic inflammatory cells, and follicular epithelial cells with oncocytic and focal squamous metaplasia. These signs were consistent with the fibrous variant of chronic lymphocytic thyroiditis (Figure 1G). The surgical specimen from the lymph nodes exhibited the classic appearance of WT with oncocytic epithelial cells and lymphoid stroma (Figure 1H). The patient was discharged home on the third day after surgery and recommended to take oral supplementation of levothyroxine. She is followed at an outpatient clinic.
- Chulam TC, Noronha Francisco AL, Goncalves Filho J, et al. Warthin’s tumour of the parotid gland: our experience. Acta Otorhinolaryngol Ital. 2013; 33: 393‑397.
- Haberal MA, Akar E, Dikis OS. Metastatic lung cancer associated with Warthin’s tumour. Niger J Clin Pract. 2019; 22: 585‑587. | Crossref
- Kızıl Y, Aydil U, Ekinci O, et al. Salivary gland tumors in Turkey: demographic features and histopathological distribution of 510 patients. Indian J Otolaryngol Head Neck Surg. 2013; 65 (suppl 1): 112‑120. | Crossref
- Teymoortash A, Krasnewicz Y, Werner JA. Clinical features of cystadenolymphoma (Warthin’s tumor) of the parotid gland: a retrospective comparative study of 96 cases. Oral Oncol. 2006; 42: 569‑573. | Crossref
- Kaliszewski K, Diakowska D, Wojtczak B, Forkasiewicz Z. Evaluation of selected ultrasound features of thyroid nodules with atypia of undetermined significance/follicular lesion of undetermined significance for the Bethesda reporting system for thyroid cytology. Cancer Manag Res. 2018; 10: 2223‑2229. | Crossref
ARTICLE INFORMATION