Sarcoidosis among hospitalized patients in Poland: a study based on a national hospital registry
Key words: hospitalization, national registries, risk factors, seasonal variation, systemic granulomatosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Sarcoidosis among hospitalized patients in Poland: a study based on a national hospital registry
Introduction: Sarcoidosis is a systemic granulomatous disease mainly affecting the lungs, although granulomas can also involve any other organ.
Objectives: We sought to describe patients during their first hospitalization for sarcoidosis in Poland from 2008 to 2015. To our knowledge, this is the first evaluation of the disease in Poland based on a hospital morbidity database.
Patients and methods: We conducted a retrospective, population‑based study, using hospital discharge records compiled by the National Institute of Public Health in the years 2008 to 2015.
Results: Among the 23097 patients included in the study, men were predominant (54.7%). The mean and median ages at hospitalization were 44.7 years (95% CI, 44.5–44.9) and 42 years, respectively. Most patients (65%) resided in urban areas. The average annual incidence rate of sarcoidosis was 7.5 per 100000 (95% CI, 7.1–7.9). The lungs were the most commonly affected organ (57.9%), while the remaining cases included sarcoidosis of lymph nodes and no lung involvement (18%), the skin (1.4%), and other or unspecified sites (22.7%). Skin sarcoidosis occurred significantly more frequently in women, while sarcoidosis of the lungs with coexisting sarcoidosis of lymph nodes was significantly more prevalent in men. Seasonal variability in sarcoidosis incidence was observed.
Conclusions: Sex and age may have a significant impact on the occurrence of sarcoidosis in Poland. Changes in seasonality may suggest the role of environmental factors. These data on sarcoidosis in Poland may be helpful in comparative analyses with other European countries.
Introduction
Sarcoidosis is a systemic granulomatous disease, which can involve any organ but predominantly affects the lungs.1 The diagnosis is established when characteristic clinical and radiological features are supported by compatible histopathology of epithelioid cell granulomas and after other known causes of granulomatous inflammation are excluded.2 The World Association of Sarcoidosis and Other Granulomatous disease recently developed criteria for organ involvement in sarcoidosis.3 Investigators are still looking for the most sensitive and accurate diagnostic methods.4
Sarcoidosis was reported to constitute a significant burden for the society, mostly due to treatment costs and work disability among patients in Poland.5 Moreover, the disease was shown to impose a significant economic burden for payers in the first year following diagnosis in a commercially insured population in the United States.6 To fully assess the burden and better understand the incidence patterns of sarcoidosis, population‑based data should be used. Integration of data from numerous sources might help fill the numerous gaps in our knowledge on the disease.
While sarcoidosis is diagnosed worldwide, there is a considerable disparity in its incidence, prevalence, and disease course between regions and populations. In the United States, the incidence and prevalence rates were higher for African Americans (17.8 and 141.4 per 100000, respectively) than for whites (8.1 and 49.8), Hispanics (4.3 and 21.7), or Asians (3.2 and 18.9). Women were 2‑fold more likely to have sarcoidosis (highest incidence in African Americans).6 The annual incidence of sarcoidosis was 10 per 100000 population in a cohort of mostly Caucasian adults in Minnesota, United States, in the years 1946 to 2013.7
The rates of sarcoidosis also range widely in Eurasia. Based on data from 1984, the crude prevalence of sarcoidosis was 28.2 per 100000 (women, 63%; annual incidence, 11.4 per 100000) in Finland and 3.7 per 100000 (women, 67%; annual incidence, 1 per 100000) in Hokkaido, Japan.8 At diagnosis, patients in Hokkaido were significantly younger than those in Finland. In Sweden, 16547 individuals had a history of sarcoidosis in 2013, and the prevalence ranged from 152 to 215 per 100000 (incidence, 11.5 per 100000 per year in the years 2003–2012). The highest prevalence was in northern sparsely populated counties.9 In Germany, the prevalence of sarcoidosis was 44 to 48 per 100000 (incidence 10 per 100000; mostly women under 50 years of age).10 In Switzerland (about 7–8 million people in 2002–2012), there were 8385 cases hospitalized in the years 2002 to 2012 with a diagnosis of sarcoidosis.11 In an Italian province, based on data for inpatients and outpatients diagnosed with sarcoidosis, the prevalence of sarcoidosis between 2000 and 2013 was 49 per 100000.12 The incidence of sarcoidosis from 1993 to 2001 in a few areas in Spain was around 1.37 per 100000.13 In a multiethnic county of greater Paris, the crude prevalence and incidence of sarcoidosis between January and December 2012 were 30.2 and 4.86 per 100000, respectively.14 The prevalence of hospitalization for sarcoidosis in the Republic of Croatia from 1997 to 2002 was 4.1 per 100000.15
There are limited data on the epidemiology of sarcoidosis in Poland. In Silesia, in a study based on data from 2006 to 2010, the standardized incidence was 3.8 to 4.5 per 100000 population.16 The incidence of sarcoidosis was 2.3 per 100000 based on data for a single hospital center for respiratory medicine in Radom in the years 2000 to 2009.17 Additionally, the characteristics of patients with sarcoidosis in Poland have changed gradually in recent decades. In a study from Zabrze, the mean age of hospitalized patients with sarcoidosis increased between the years 1976 to 1980 and 1996 to 2000 (37 vs 41.6, P <0.05) and the percentage of women significantly decreased (63.3% vs 50.0%, P <0.05).18
International variation in the epidemiology of sarcoidosis suggests that there might be more than 1 causative agent, including environmental factors, in genetically susceptible hosts. For example, workplace settings in which there is exposure to inorganic triggers of inflammation can promote an exuberant granulomatous immune response to different antigens.19 Sarcoidosis likely has more than 1 cause.
Beyond the epidemiologic sources already cited, information on sarcoidosis in Poland is based on case reports or reports from selected regions of Poland.1,20,21 Investigators in the United States and Sweden have profitably used national administrative databases and patient registries to investigate sarcoidosis.6,22 This may be a promising approach for researchers in other countries as well.
We sought to describe patients during their first hospitalization for sarcoidosis in Poland from 2008 to 2015. To our knowledge, this is the first evaluation of the disease in Poland based on a hospital morbidity database.
Patients and methods
In this retrospective, population‑based study, we analyzed hospital discharge records of patients diagnosed with sarcoidosis. We obtained data from the National Institute of Public Health in Poland covering the period from 2008 to 2015. We analyzed the records relating to patients during their first hospitalization for sarcoidosis. All hospitals in Poland, except psychiatric and military facilities, are legally required to send discharge data to the institute. The data are anonymous and include information on hospitalizations with International Classification of Diseases, Tenth Revision code diagnoses, dates of admission and discharge, birth date, sex, and place of residence. We analyzed 2 samples: 1) all hospitalizations for sarcoidosis, and 2) first hospitalizations for sarcoidosis. We also obtained demographic data for the general Polish population from the Central Statistical Office of Poland.23 Incidence rates were calculated using the number of patients with sarcoidosis and corresponding census data. We conducted the study in accordance with generally applicable laws. Sarcoidosis often requires advanced differential diagnostic procedures or treatment during hospitalization. Therefore, hospitalized cases may provide a good basis for estimating incidence. We assumed that sarcoidosis diagnoses in hospitals were based on the most current, widely used criteria.
The study was conducted in accordance with the regulations of the Bioethics Committee of the Medical University of Warsaw.
Statistical analysis
To perform the statistical analyses, we used R24 and WINPEPI25 softwares. We computed means, medians, and ranges for continuous variables, and counts and percentages for categorical variables. We estimated 95% confidence intervals (CIs) by assuming that cases followed a Poisson distribution. We calculated prevalence and incidence rates by dividing the relevant number of disease cases by the corresponding census figures. To assess trends, we used linear regression, time series analysis, and the augmented Dickey–Fuller test. When normality assumptions were not met, we used the nonparametric Mann–Whitney test. To compute odds ratios, a univariate logistic regression model was used. A 2‑sided P value of less than 0.05 was considered significant.
Results
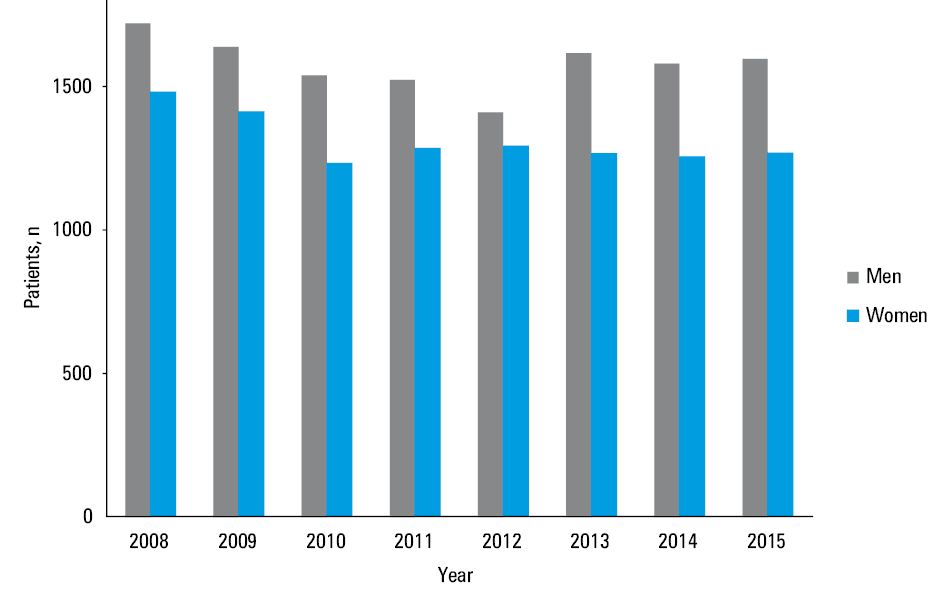
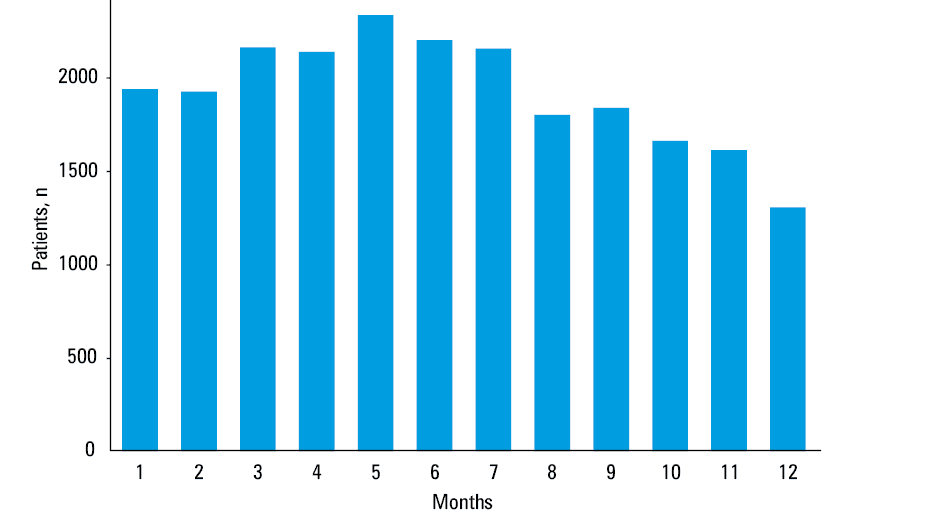
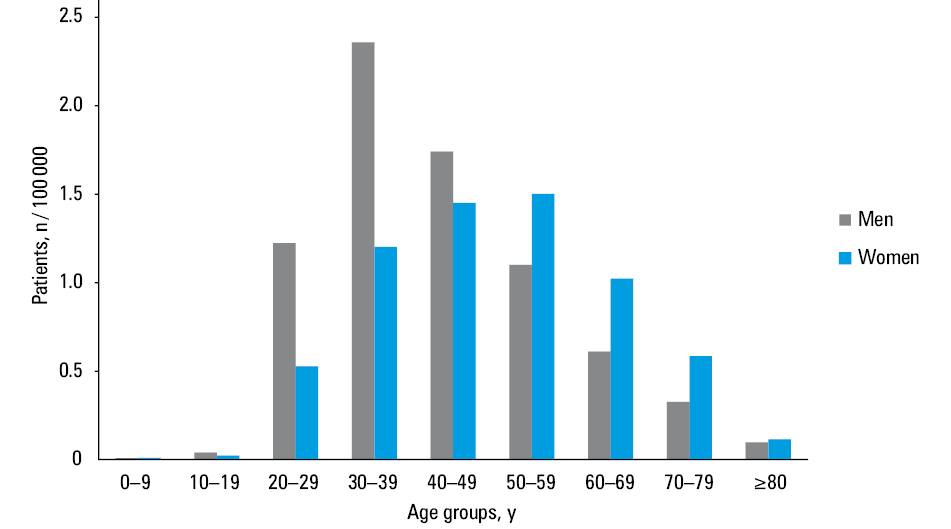
Among the 23097 patients during their first hospitalization for sarcoidosis, there were more men than women (54.7% vs 45.3%, P <0.001). The mean and median ages at hospitalization were 44.7 (95% CI, 44.5–44.9) and 42 years, respectively. Most patients resided in urban than in rural areas (65% vs 35%, P <0.001). The incidence rate was higher (P <0.001) for urban (8/100000; 95% CI, 7.9–8.2) than for rural areas (6.7/100000; 95% CI, 6.5–6.8). Based on hospitalization records and census data, the average annual incidence rate of sarcoidosis during the 8‑year period was 7.5 per 100000 (95% CI, 7.1–7.9). The number of first hospitalizations for sarcoidosis by sex and year is shown in Figure 1, and by month, in Figure 2. During the study, 73 patients died while hospitalized (0.3% of all patients). The point prevalence at the end of the study was 60 per 100000 inhabitants. Women were significantly older than men during their first hospitalization for sarcoidosis (48.6 years vs 41.3 years, P <0.05). Moreover, female patients tended to be in their 40s and 50s, while male patients, in their 30s and 40s (Figure 3).
Sarcoidosis most commonly affected the lungs without lymph node involvement (32.1%), followed by sarcoidosis of the lungs with lymph node involvement (25.8%), lymph nodes (18%), skin (1.4%), and other or unspecified sites (22.7%). Skin sarcoidosis occurred more often in women than in men (odds ratio [OR], 2.0; 95% CI, 1.55–2.6; P <0.001), while sarcoidosis of the lungs with coexisting sarcoidosis of lymph nodes was more prevalent in men (OR, 1.28; 95% CI, 1.12–1.46; P <0.001). There were no significant sex differences in the frequency of other types of sarcoidosis. The most common comorbidities among patients with sarcoidosis included cardiovascular (41.8%), respiratory (28.2%), musculoskeletal (10.7%), and digestive (8.7%) disorders, while other diseases accounted for less than 5% of the cases.
We observed no significant time trend in the incidence of first‑time hospitalizations with a sarcoidosis diagnosis. We also noted that the number of first hospitalizations for sarcoidosis differed by month (P <0.01), with the highest number in May and the lowest in December.
Discussion
Based on hospital discharge data, we estimated the average annual incidence of sarcoidosis in Poland to be 7.5 per 100000. This rate is similar to the rates observed in other European countries,8-10,14 including Poland.16,17
In our study, there were more men than women, and women tended to be older than men. This is in line with a previous Polish study on 1810 hospitalized patients with sarcoidosis during a 4‑year period, in which 47.6% of the population were women at a mean (SD) age of 43.5(12.2) years.1 Other studies provided inconsistent results regarding the differences in prevalence between sexes, with sarcoidosis reported to be either more prevalent in men22 or in women.12,13 In another Polish study, sarcoidosis occurred primarily in younger men (age, 25–50 years) and older women (age, 50–64 years).16 In a population‑based cohort of primarily Caucasian adults in Minnesota, United States, the mean age at diagnosis was 48.3 years in women and 42.8 years in men.7 In a study conducted in the United States, women tended to be older at disease onset and more often had cutaneous involvement than men.26 In patients with sarcoidosis hospitalized in Croatia from 1997 to 2002, 44.5% were between 20 and 39 years of age, 40.1% were between 40 and 59 years of age, and 15.3% were more than 60 years old.15 Women had a late onset of sarcoidosis in other studies.9,12 Our results are also consistent with a previous study reporting that the female‑to‑male ratio was significantly higher in patients with late‑onset sarcoidosis than in younger patients (5:1 and 1:1, respectively).27
A widely accepted hypothesis for the etiology and pathogenesis of sarcoidosis is that of a complex interaction between environmental and genetic factors. However, sarcoidosis is still poorly understood.28 Our results suggest the possible contribution of environmental factors to the pathogenesis of sarcoidosis. We observed no significant time‑trend in the incidence of first‑time hospitalizations with sarcoidosis diagnosis and found significant differences in the incidence of sarcoidosis by month. Sarcoidosis may be exacerbated by endogenous vitamin D production due to increased sun exposure in the summer, and we noted increased incidence in the summer months. The rates of hospitalizations for sarcoidosis in Switzerland were highest in June and lowest in October and December (P <0.001).11 In residents from Olmsted County, Minnesota, who were diagnosed with sarcoidosis between 1976 and 2013, the age- and sex‑adjusted incidence of sarcoidosis was lower in autumn compared with winter, spring, and summer, and this pattern was stable across decades.29 Yet, seasonal variations in sarcoidosis were not reported elsewhere. For example, in Turkey, the onset of symptoms was most frequent in spring and least frequent in the second half of the year (summer or autumn).30 Among veterans in the United States, there was no seasonality in the presentation of new sarcoidosis cases.31 There were also no significant calendar year trends in the incidence either for women or men in a large study from the United States characterizing the epidemiology of sarcoidosis from 1946 to 2013.7 In a Croatian study, the ratio of patients with sarcoidosis in the continental zone to the Mediterranean zone was 1.5:1.15 Geographical variation in the prevalence of sarcoidosis was also reported in a nationwide registry–based study in Sweden.9
In our study, the incidence rate of sarcoidosis was significantly higher for urban than rural areas. This is in contrast to findings from a previous study from one region of Poland, reporting the highest rates typical for districts with a predominance of forests and arable land.16
The higher incidence rate observed in urban regions in this study may be related to the fact that that most smokers live in rural regions in Poland.32 A population‑based nested case‑control study from the United States reported that current smokers had a reduced risk of sarcoidosis.33 Moreover, in a Polish study, the authors hypothesized that smoking protects from structural abnormalities in the lungs and suggested further studies to confirm this finding.34 However, another study from Poland, based on data of 180 patients with respiratory sarcoidosis diagnosed and treated in the years 2002 to 2010, reported that the incidence of sarcoidosis was not influenced by the place of residence of patients.35 Rural and urban populations in Spain had similar incidence rates of sarcoidosis.13
Epidemiologic studies demonstrated associations between environmental exposures and sarcoidosis.19,36-40 These studies suggested that exposure to many different antigens in the environment and workplace may influence the incidence rates of sarcoidosis in urban and rural areas in Poland. However, there are no studies showing a clear connection between occupational or environmental risk factors and the disease. Therefore, further research is needed, especially to elucidate the discrepancies in results reported in literature, as there is no clear pattern of the disease.
During the 8‑year period of our study, 0.3% of all patients with sarcoidosis died while being hospitalized. The risk of death from sarcoidosis during hospitalization seems to be relatively low. Similarly, the overall mortality rate of patients with sarcoidosis in the cohort of mostly Caucasian adults in Minnesota, United States, did not differ from that of the general population.7 In Sweden, individuals with sarcoidosis were at higher risk of death compared with the general population, but for the majority, the increased risk was small.22 In a 2015 nationwide cohort study in Denmark, patients with sarcoidosis had an increased cancer risk shortly after the sarcoidosis diagnosis. The risk was higher by 20% and 10% in the periods of 3 to 10 years and more than 10 years after the diagnosis, respectively.41 In a recent study, only age, the extent of fibrosis on high‑resolution computed tomography, and precapillary pulmonary hypertension were independent predictors of mortality in patients with sarcoidosis.42 Comorbidity burden was strongly associated with mortality in a Polish cohort of sarcoidosis patients.43
In our study, sarcoidosis of the lungs with and without lymph node involvement was most common. Moreover, in a previous study, the majority of Polish patients with sarcoidosis (80.6%) were discharged with the diagnosis of pulmonary and/or lymph node sarcoidosis.1 In the study by Unprasert et al,7 50% of sarcoidosis patients had evidence of pulmonary parenchymal infiltration.7 In our study, skin sarcoidosis was recorded for 1.4% of patients. This percentage is low compared with the 18% of patients with cutaneous skin involvement, which was the most common extrathoracic manifestation of sarcoidosis in the Minnesota cohort.7
Our study has several limitations. The hospital discharge database we analyzed did not include other variables that might have been related to sarcoidosis. Also, the database included discharge records from inpatient hospitalizations only, which means it excluded sarcoidosis patients who were seen only as outpatients. However, sarcoidosis is a systemic inflammatory disease with possible multiorgan involvement and may require treatment or advanced diagnostic procedures that can be performed in a short period of time only in the inpatient setting. Additionally, the date of the first hospitalization for sarcoidosis is not necessarily the date of the first diagnosis. This inaccuracy may have resulted in overestimating incident cases. However, the long study period may have minimized the overestimation.
- Martusewicz‑Boros MM, Boros PW, Wiatr E, et al. Systemic treatment for sarcoidosis was needed for 16% of 1810 Caucasian patients. Clin Respir J. 2018; 12: 1367‑1371. | Crossref
- Spagnolo P. Sarcoidosis: a critical review of history and milestones. Clin Rev Allergy Immunol. 2015; 49: 1‑5. | Crossref
- Judson MA, Costabel U, Drent M, et al. The WASOG Sarcoidosis Organ Assessment Instrument: an update of a previous clinical tool. Sarcoidosis Vasc Diffuse Lung Dis. 2014; 31: 19‑27.
- Kocoń P, Szlubowski A, Kużdżał J, et al. Endosonographyguided fineneedle aspiration in the diagnosis of sarcoidosis: a randomized study. Pol Arch Intern Med. 2017; 127: 154‑162.
- Kawalec PP, Malinowski KP. The indirect costs of systemic autoimmune diseases, systemic lupus erythematosus, systemic sclerosis and sarcoidosis: a summary of 2012 real‑life data from the Social Insurance Institution in Poland. Expert Rev Pharmacoecon Outcomes Res. 2015; 15: 667‑673. | Crossref
ARTICLE INFORMATION