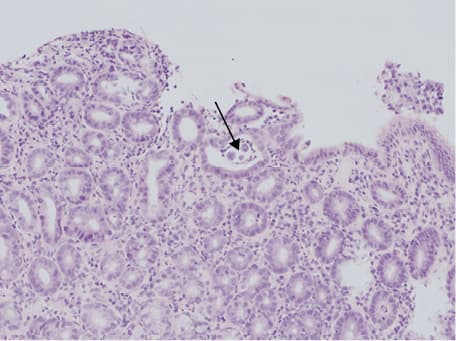
A 71‑year‑old woman with bronchial asthma after lobectomy of the right lung due to chronic respiratory failure was admitted to our department because of increased dyspnea, cough, and fever. Biochemical studies revealed mild normocytic anemia (hemoglobin, 11.7 g/dl; reference range, 12–16 g/dl), leukocytosis (white blood cells, 15.7 × 103/μl; reference range, 4–10 × 103/μl), and peripheral blood eosinophilia (eosinophils, 2.10 × 103/μl; reference range, 0.00–0.45 × 103/μl), which did not respond to treatment. Occult blood was present in the feces. Chest computed tomography revealed inflammatory changes of the lungs in the regression phase, mottled areas with reduced transparency (ground glass opacity) of the lung parenchyma, and features of bronchiectasis. Panendoscopy demonstrated superficial gastritis in the antrum and the gastric corpus, and colonoscopy revealed no pathological changes. Histologic examination of the material collected during gastroscopy revealed Strongyloides stercoralis larvae in the lumen of a single intestinal crypt (Figure 1). In the material collected during colonoscopy, we observed inflammatory infiltration with a large number of eosinophils. The patient was referred to the Outpatient Clinic of Infectious Diseases in Łańcut, and albendazole was administered at a daily dose of 2 × 400 mg for 7 days.
Strongyloidiasis is a parasitic disease caused by Strongyloides stercoralis, a nematode that occurs mainly in tropical and subtropical areas and sporadically in places with a moderate climate.1 The parasite, in the form of invasive larvae that live in contaminated soil, water, or feces, penetrates the skin and enters the bloodstream, making its way to the lungs through the veins. After getting into the alveoli, the larvae move along the bronchial tree toward the throat where they are swallowed. In the digestive tract, they mature and transform into adult females living in the mucous membrane of the duodenum and jejunum.2
Most often, the course of infection is asymptomatic, but skin, gastrointestinal, and pulmonary symptoms may develop. The most common symptoms are rash accompanied by pruritus (16%–90%); abdominal pain, nausea, diarrhea, and bloating (41%–74%); and cough with hemoptysis, or dyspnea and bronchial spasm (~25%).3 The course of infection is occasionally severe, especially in patients with immune disorders. Laboratory tests reveal eosinophilia (which is often the only symptom), a high level of immunoglobulin E, and anemia. Diagnosis is usually made on the basis of fecal parasite larval infestation, but the test is not very sensitive and may require several attempts. For this reason, serological enzyme‑linked immunosorbent assay tests, which demonstrate high sensitivity and specificity, are considered the tests of first choice.4 An equally sensitive but invasive diagnostic method is histologic evaluation of the material obtained from biopsy of the duodenal mucosa during endoscopy examination.5
Treatment of strongyloidiasis should lead to complete eradication of the parasite. Currently, the most effective drug is considered to be ivermectin at a dose of 200 μg/kg body weight for 1 to 2 days. The second‑line drug is albendazole at a dose of 2 × 400 mg per day for 5 to 7 days.
- Jourdan PM, Lamberton PHL, Fenwick A, Addiss DG. Soil‑transmitted helminth infections. Lancet. 2018; 391: 252‑265. | Crossref
- Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001; 33: 1040‑1047. | Crossref
- Nuesch R, Zimmerli L, Stockli R, et al. Imported strongyloidosis: a longitudinal analysis of 31 cases. J Travel Med. 2005; 12: 80‑84. | Crossref
- Bosqui LR, Marques PD, de Melo GB, et al. Molecular and immune diagnosis: further testing for human strongyloidiasis. Mol Diagn Ther. 2018; 22: 485‑491. | Crossref
- Kishimoto K, Hokama A, Hirata T, et al. Endoscopic and histopathological study on the duodenum of Strongyloides stercoralis hyperinfection. World J Gastroenterol. 2008; 14: 1768‑1773. | Crossref
ARTICLE INFORMATION