Periocular xanthogranuloma with adult-onset asthma: a rare disorder associated with elevated IgG4 levels



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Periocular xanthogranuloma with adult-onset asthma: a rare disorder associated with elevated IgG4 levels
A 69‑year‑old man with periocular xanthogranuloma was admitted to the Department of Hematology and Clinical Immunology of Holy Cross Cancer Center in Kielce, Poland, for a diagnostic workup due to suspicion of systemic histiocytosis. He had a 5‑year history of bilateral yellowish swelling of the upper and lower eyelids. He also reported sinusitis, nasal polyps, and adult‑onset asthma that began 3 years before the periocular infiltration. Moreover, his medical history included skin lesions and eosinophilia. Physical examination showed significant swelling of the eyelids (Figure 1A), erythematous and edematous skin lesions involving the torso and upper extremities, multiple excoriations (scratch marks), and clubbed fingers. Complete blood count revealed an elevated eosinophil count of 1.11 × 109/l. Other laboratory test results, including red blood cell and platelet counts, were normal. Biochemical tests indicated polyclonal hypergammaglobulinemia on serum protein electrophoresis, with the immunoglobulin (Ig) G levels of 21.3 g/l and IgE levels of 8.181 mg/l. C‑reactive protein level and erythrocyte sedimentation rate were within the reference range. The patient tested negative for antinuclear and antineutrophil cytoplasmic antibodies.
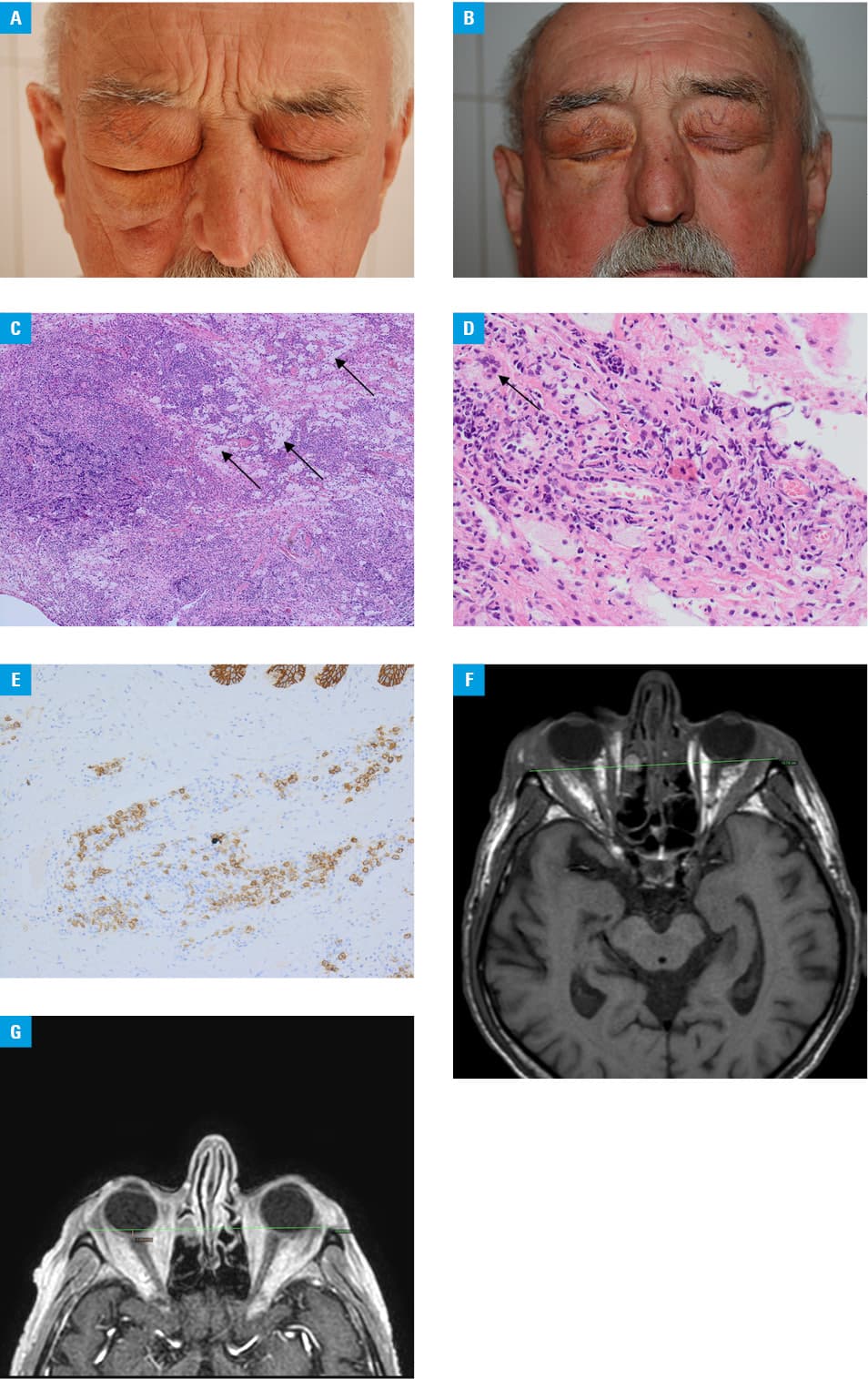
Before admission, the patient underwent a biopsy of the right inferior orbit, which showed histiocytic infiltration (Figure 1C and 1D). Additional immunostaining showed no expression of the CD1a and CD207 antigens, which excluded Langerhans cell histiocytosis. Magnetic resonance imaging confirmed hypertrophy of intraorbital adipose tissue, bilateral proptosis, and thickening of both eyelids (Figure 1F). To exclude systemic histiocytosis, whole‑body computed tomography was performed, which indicated no osteolytic lesions. The size of the liver and spleen was normal. High‑resolution computed tomography of the chest showed no changes suggestive of systemic histiocytosis. Bone marrow trephine biopsy was typical of normal hematopoiesis. The p.V600E mutation of the BRAF gene was not detected.1
A biopsy specimen of the affected skin segment from the right subscapular area showed perivascular inflammatory infiltrates consisting mainly of eosinophils, lymphocytes, and IgG4 plasmocytes (Figure 1E). Previously, the IgG4 plasma cells were also found in the biopsy specimens from the right inferior orbit. The serum IgG4 level was significantly elevated (3.38 g/l; reference range, [0.0392–0.864 g/l]).
Based on periocular histiocytic infiltration, symptoms of adult‑onset asthma, nasal polyps, and eosinophilia, we made a diagnosis of periocular xanthogranuloma associated with adult‑onset asthma (PXAOA).2,3 Treatment with oral prednisone was started at a dose of 1 mg/kg once daily, which was gradually tapered. At the same time, the patient received 6 cycles of intravenous cyclophosphamide at a dose of 750 mg/m2 every 4 weeks. Within 7 months, periocular swelling significantly decreased (Figure 1B and 1G). The serum IgG, IgG4, and IgE levels, as well as the eosinophil count, returned to normal values. However, when the prednisone dose was tapered to 10 mg/d, the ocular manifestations recurred. Methotrexate was then initiated with good effect.
PXAOA is a rare, benign, non‑Langerhans cell histiocytosis. Some cases have been described in the literature as a manifestation of IgG4‑related disease (IgG4‑RD).4 However, patients with elevated serum IgG4 levels present with a wide array of disorders, and only a minority of them have IgG4‑RD.5 The differential diagnosis is complicated, but according to the draft classification criteria for IgG4‑RD developed by the American College of Rheumatology and European League Against Rheumatism (Stone, unpublished data, 2018), the elevated serum IgG4 level in our patient was an accompanying immune disorder.
- Emile JF, Abla O, Fraitag S, et al. Revised classification of histiocytoses and neoplasms of the macrophage‑dendritic cell lineages. Blood. 2016; 127: 2672‑2681. | Crossref
- London J, Soussan M, Gille T, et al. Adult‑onset asthma associated with periocular xanthogranuloma: new diagnostic and therapeutic approaches in a very rare systemic disease. Ophthalmic Plast Reconstr Surg. 2013; 29: 104‑108. | Crossref
- Jakobiec FA, Mills MD, Hidayat AA, et al. Periocular xanthogranulomas associated with severe adult‑onset asthma. Trans Am Ophthalmol Soc. 1993; 91: 99‑125.
- London J, Martin A, Soussan M, et al. Adult onset asthma and periocular xanthogranuloma (AAPOX), a rare entity with a strong link to IgG4‑related disease: an observational case report study. Medicine (Baltimore). 2015; 94: e1916. | Crossref
- Ryu JH, Horie R, Sekiguchi H, et al. Spectrum of disorders associated with elevated serum IgG4 levels encountered in clinical practice. Int J Rheumatol. 2012; 2012: 232960. | Crossref
ARTICLE INFORMATION