Introduction
This case describes macrophage activation syndrome (MAS) associated with systemic lupus erythematosus (SLE). This is an underrecognized hyperinflammatory syndrome of excessive immune activation. It is characterized by inappropriate survival of histiocytes and cytotoxic T cells, leading to a cytokine storm, hemophagocytosis, and multiorgan damage.1 If not promptly identified and treated, it is a life‑threatening condition. The diagnostic workup is difficult because many findings are nonspecific and the disease is rare. MAS is considered a subtype of hemophagocytic lymphohistiocytosis (HLH), which in turn is divided into familial HLH and secondary or acquired HLH (sHLH). Familial HLH normally presents in infancy. Secondary HLH may be triggered by malignancy, autoimmunity, or infection. HLH is termed MAS if it occurs in association with a rheumatic disease.2 In adults, MAS is most prevalent with adult‑onset Still disease, and is estimated to occur in 10% to 15% of patients with that disease.3,4 SLE‑associated MAS has an estimated prevalence ranging from 0.9% to 9% of patients with SLE, with the SLE prevalence of 1 to 25 per 100000 in the general population.5,6 However, in adults the leading cause of sHLH are infections, of which viruses account for the majority.7
Case description
A 37‑year old woman presented to the emergency department with a 6‑week history of new‑onset generalized nonpruritic erythematous rash covering her face, hands, arms, trunk, and lower limbs. She had intermittent fever over the same 6 week period and a weight loss of 5 kg. A sore throat proceeded the rash by 1 week. This was treated by a general practitioner with amoxicillin. She denied any other infective symptoms. She complained of diffuse hair loss. She had no history of Raynaud phenomenon, serositis, or skin thickening. She had 1 previous miscarriage in the first trimester and 3 normal pregnancies. She denied nausea, vomiting, contact with the sick, recreational drug use, or recent travel.
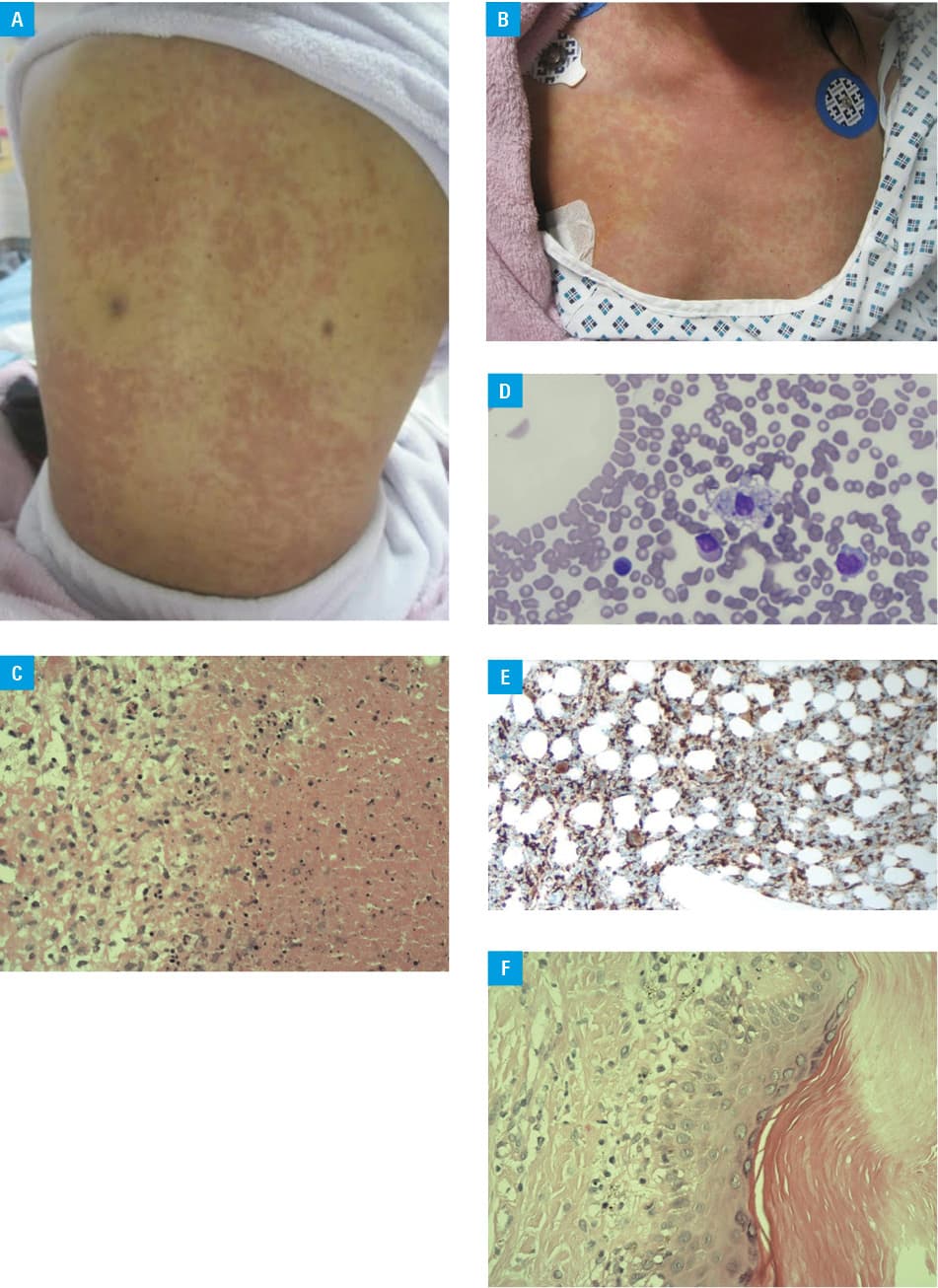
On examination, she had a widespread erythematous macular rash (Figure 1Aand 1b) with skin sloughing from the fingertips. There were associated areas of pigmentation on the trunk. She had no synovitis. Diffuse hair loss was noted, there was but no alopecia. Cardiac, respiratory, gastrointestinal, and neurological examinations were unremarkable. She did not take any medications regularly.
Course of events
Extensive laboratory evaluation was completed. On admission, hemoglobin was 11.7 g/dl (reference range, 11.5–16.5 g/dl) with mean corpuscular volume of 82 fl (reference range, 78–97 fl) and mean corpuscular hemoglobin of 28 pg/cell (reference range, 26–34 pg/cell). White cell count on admission was 1.1 × 109/l (reference range, 4.0–11.0) with neutrophils of 0.83, lymphocytes, 0.2, monocytes, 0.07, eosinophils, 0.00, and basophils, 0.01. Platelets on admission were 139 × 109/l (reference range, 150–145 × 109/l). Urea, creatinine, and electrolytes were within normal ranges. Liver function tests on admission showed evidence of transaminitis with alkaline phosphatase of 176 IU/l (reference range, 40–150 IU/l), alanine aminotransferase, 106 IU/l (reference range, <55 IU/l), γ-glutamyltransferase, 237 IU/l (reference range, 9–36 IU/l), and aspartate aminotransferase, 265 IU/l (reference range, 5–34 IU/l). Lactate dehydrogenase was elevated at 423 IU/l (reference range, 125–220 IU/l). C‑reactive protein on admission was 5.0 (reference range <5) and erythrocyte sediment ratio was 58 (reference range <12). Iron was decreased at 5 nmol/l (reference range, 9–30.4 nmol/l), vitamin B12, 516 pg/ml (reference range, 187–883 pg/ml), folate, 12 ng/ml (reference range, 3–20.1 ng/ml), and fibrinogen, 2.7 g/l (reference range, 1.5–4.0 g/l). Direct Coombs test was positive. Creatine kinase on admission was elevated at 424 IU/l (reference range, 29–168 IU/l). Total cholesterol was elevated at 8.00 mmol/l (reference range <5 mmol/l). Triglycerides were elevated at 15.08 mmol/l. High- and low‑density cholesterol were unsuitable for analysis as triglyceride level was so high.
The patient had intermittent high‑grade fever with temperatures in excess of 38°C from admission. Infectious diseases screening was performed and was negative for immunoglobulin M to Epstein‑Barr virus, positive for immunoglobulin G to Epstein‑Barr virus, negative for cytomegalovirus, HIV. Also, hepatitis B and C serology and surface antigen were negative. Herpes simplex virus 1 and 2 were not detected. Blood cultures completed 3 times every 24 hours were negative for growth; transesophageal echocardiogram was negative for vegetations. Urine dipstick was normal and urine culture showed no growth.
Hemoglobin subsequently dropped to 8.5 g/dl on the third day from admission with mean corpuscular volume of 74 fl and mean corpuscular hemoglobin of 23 pg. Platelet count dropped to a low of 69 × 109/l in the first week. Blood film was then completed and showed a left‑sided neutrophil shift with an occasional activated monocyte, target cells, leucopenia, neutropenia, and reduced platelet count. Ferritin level measured on the third day was elevated at 6.703 ng/ml (reference range, 5–204 ng/ml).
Autoimmune screening was completed to assess the presence of an underlying disease. The antinuclear antibody ratio was positive with a result of 9.9 (reference range <0.7), antibodies to double‑stranded DNA was negative, anti‑Ro antibody was positive at 240 U/ml (reference range <0.7 U/ml), anti‑La was positive at 84 U/ml (reference range <0.7 U/ml). Anti‑RNP antibody was elevated at 63 U/ml (reference range <0.7 U/ml). The following were negative: anti‑SCL 70 antibody, anti‑Jo1 antibody, anti‑Smith antibody, and anti‑centromere antibody. Complement analyses showed reduced component C3 level at 0.78 g/l (reference range, 0.83–1.8 g/l) and normal component C4 level at 0.22 g/l (reference range, 0.14–0.54 g/l). Serum protein electrophoresis showed normal immunoglobulin G and immunoglobulin M levels, and elevated immunoglobulin A level at 4.0 g/l (reference range, 0.21–2.91 g/l). Rheumatoid factor was normal. Lupus anticoagulant was negative.
The patient continued to have persistent fevers, anorexia, and fatigue. In the context of the associated weight loss, a computed tomography of the chest, abdomen, and pelvis was performed to rule out a malignant cause. The findings showed supraclavicular lymphadenopathy, which was biopsied and showed evidence of necrotizing lymphadenitis. (Figure 1C). A follow‑up with regular checkups was recommended. There was no evidence of malignancy.
The patient was examined by a hematologist, and a bone marrow biopsy was performed. The biopsy showed disorganized hematopoiesis and evidence of hemophagoctyosis (Figure 1D) which was also confirmed on CD68 straining (Figure 1E). On dermatologic assessment, the skin rash was characteristic of acute lupus. Skin biopsy was completed at 3 sites including the left foot, upper arm, and nasal alae. The appearances differed at each site. The biopsy showed perivascular karyorrhectic fibrosis, focal fibrinoid necrosis, and minimal red blood cell extravasation. The presence of vacuolar interface lesions was in line with acute lupus (Figure 1F). The patient met the diagnostic criteria for SLE as per the 2012 Systemic Lupus International Collaborating Clinics Criteria, with clinical (acute rash) and laboratory parameter requirements (positive for antinuclear antibodies and lupus anticoagulant, thrombocytopenia, leukopenia, low levels of complement component C3). Diagnosis of MAS secondary to acute SLE was made after the assessment of the extensive blood workup and after the HScore criteria for secondary HLH/MAS was met.
Treatment
The patient was treated with 500 mg methylprednisolone 3 times daily for the first 3 days and intravenous immunoglobulins at a dose of 1 g/kg for 2 consecutive days. The monitoring of ferritin and lactate dehydrogenase levels and full blood count was performed daily. On the fourth day of treatment, the patient was changed to 50 mg oral dexamethasone. After 14 days she was started on mycophenolate mofetil 500 mg daily for 2 weeks, titrated up to 1 g twice daily, and steroids were slowly tapered. She was started on alendronate for bone protection and esomeprazole for gastric protection while on steroids. Additionally, calcium and vitamin D supplementation was started. After the acute treatment, she was initiated on hydroxychloroquine 5 mg/kg/day orally for treatment of the underlying SLE. Luckily, the patient responded clinically with resolution of intermittent fever and improvement of biochemical parameters and rash.
The guidelines for clinical deterioration despite immediate treatment are derived from case reports. Anakinra, starting at 1 to 2 mg/kg and increasing to 8 mg/kg/d, is often used as the second‑line treatment. In patients who remain refractory, a discussion with hematologists is recommended as etoposide may be needed.8
Discussion
Secondary HLH is a clinical syndrome with features that mimic the features of many other systemic illnesses. Pyrexia of unknown origin is the cardinal feature of the syndrome. It is a nonspecific sign, and extensive investigations are required to establish the diagnosis.
Hyperferritinemia is a key laboratory feature and was a key diagnostic clue in this case. In a single‑center retrospective review of serum ferritin, levels of more than 10000 ng/ml were 96% specific and 90% sensitive for HLH.9 Serum ferritin level is also closely related to disease activity and both maximum ferritin levels and a decrease of less than 50% during treatment is associated with increased mortality.10 Other notable blood abnormalities include cytopenias, hypertriglyceridemia, and hypofibrinogenemia. This patient had a high ferritin level, cytopenias, and hypertriglyceridemia.
In sHLH, regardless of the cause (infectious, autoimmune, malignant), the overall mortality is significant at 41%.3 Internal organ involvement is frequent and includes hepatosplenomegaly, pulmonary involvement, adenopathies, neurological involvement, skin eruptions, gastrointestinal, and renal involvement. It often leads to progressive multiple organ failure, and intensive care treatment is needed in nearly half of the patients.11 This patient had a relatively benign disease course with a favorable outcome.
Lessons to be learned from the case
1) Clinicians should have a high degree of suspicion of MAS in a patient who is systemically unwell with pyrexia of unknown origin, cytopenias, and high ferritin levels; 2) it is important to investigate and treat the patient for all underlying causes of MAS, bearing in mind that up to one‑third of adults with HLH have more than 1 trigger; 3) there is little evidence regarding therapeutic approaches to adult sHLH and treatment relies largely on case reports and uncontrolled studies. It is important to get expert input early in the disease course.
- Henter JI, Samuelsson‑Horne A, Aricò M, et al. Treatment of hemophagocytic lymphohistiocytosis with HLH‑94 immunochemotherapy and bone marrow transplantation. Blood. 2002; 100: 2367‑2373. | Crossref
- Carter SJ, Tattersall RS, Ramanan AV, et al. Macrophage activation syndrome in adults: recent advances in pathophysiology, diagnosis and treatment. Rheumatology (Oxford). 2019; 58: 5‑17. | Crossref
- Dhote R, Simon J, Papo T, et al. Reactive hemophagocytic syndrome in adult systemic disease: report of twenty‑six cases and literature review. Arthritis Rheum. 2003; 49: 633‑639. | Crossref
- Fukaya S, Yasuda S, Hashimoto T, et al. Clinical features of haemophagocytic syndrome in patients with systemic autoimmune diseases: analysis of 30 cases. Rheumatology (Oxford). 2008; 47: 1686‑1691. | Crossref
- Tsuji T, Ohno S, Ishigatsubo Y. Liver manifestations in systemic lupus erythematosus: high incidence of hemophagocytic syndrome. J Rheumatol. 2002; 29: 1576‑1577.
ARTICLE INFORMATION