Introduction
A differential diagnosis of large intracardiac masses can be difficult, considering numerous overlapping characteristics between possible causes. In this report, we describe a benign mass in the left atrium (LA) diagnosed by transesophageal echocardiography (TEE) on the operating table before a planned cardiac surgery.
Case description
A 73‑year‑old woman was admitted to the hospital, complaining of worsening weakness over the past 6 months. During the previous month, even light exercise had caused breathlessness and the feeling of pressure in the left thorax, resulting in excessive cold sweat. The patient had been unable to sleep because of dyspnea and had no appetite (she reported a weight loss of 6 kg over 6 months). She did not report any nighttime sweats or fever.
Over 10 years earlier, the patient was diagnosed with permanent atrial fibrillation and mild‑moderate mitral stenosis, and since then she had received anticoagulant treatment with warfarin. She visited her general practitioner only once or twice a year, and her internationalized normalized ratio on the rare visits ranged from 2.6 to 3.6. Later, she admitted to not having been fully adherent to warfarin treatment. She had no history of embolic events.
The patient presented to the hospital in stable hemodynamic condition. Physical examination revealed a blood pressure of 110/92 mm Hg and atrial fibrillation with a heart rate of 120 to 160 bpm. She had grade IV systolic murmur with the maximum volume on the apex of the heart.
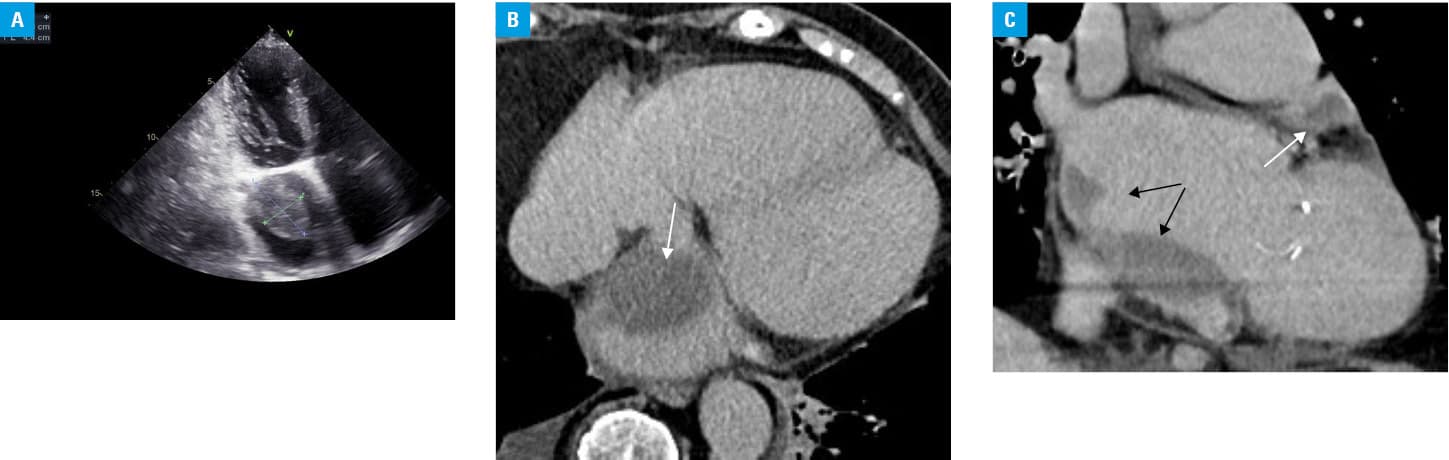
She was first examined at a local hospital with computed tomography and angiography to identify pulmonary embolism. No pulmonary embolism was shown, but a large mass in the LA was revealed. The patient was referred to a regional hospital for further differential diagnosis. Echocardiography was performed once tachycardia was stabilized. Both atria were severely dilated, and there was a large mass (4.4 × 2.8 cm) in the LA (Figure 1A). The mass showed a heterogeneous echotexture and a lobular structure. It was fixed to the septal wall (Figure 1B) and extended over the inferior wall to the lateral wall of the LA (Figure 1C). No mass was seen in the LA appendage. There was no LA spontaneous echo contrast. In addition, rheumatic mitral valve disease with moderate stenosis (mitral valve area, 1.2 cm²) and moderate regurgitation was noted. The LA mass did not obstruct the mitral outflow.
Magnetic resonance tomography (MRT) revealed the same lens‑shaped mass with no late contrast enhancement. The signal was the same on T1 and T2 images. The mass extended along the septal atrial wall. In the LA appendage, a separate small mass with a similar signal was observed.
A team of 2 cardiologists and a cardiac surgeon decided that a biopsy was needed for a conclusive diagnosis. The patient was scheduled for an elective cardiac surgery for rheumatic mitral valve repair and mass excision. Before surgery, a final TEE was performed, which showed that the mass had shrunk 3 times its size to a maximum dimension of 1 cm after 2 months of adequate warfarin treatment. The stenosis remained moderate and the mitral regurgitation was graded as mild. Clinical symptoms and the quality of life of the patient had drastically improved. Considering clinical and radiological improvement, the surgery was cancelled. The echocardiographic findings are shown in Supplementary material, Table S1.
The patient was evaluated 3 months later, and there was no intracardiac mass on TEE. She had no signs or symptoms of heart failure.
Discussion
There have been several case reports describing difficulties in differentiating myxomas from thrombi.1-3 There are specific characteristics that guide the correct diagnosis; however, sometimes it is still difficult to make the final decision. It is extremely important to establish the right diagnosis, considering that different treatment strategies are applied: anticoagulation for a thrombus and surgical removal for a myxoma.
Atrial myxomas are the most common primary intracardiac tumors in adults. Two‑thirds of myxomas occur in the LA. They are mostly singular and appear as well‑defined, smooth, oval, or lobulated lesions that are commonly pedunculated on echocardiography.1
Cardiac thrombi are more frequent than cardiac myxomas. They typically originate from the LA appendage, have smooth contours, are sessile, and therefore move synchronously with the adjacent heart wall.4 Intracardiac thrombi generally occur in patients with organic heart disease. Chronic conditions favoring thrombus formation are atrial fibrillation, atrial chamber enlargement, prosthetic or stenotic mitral and tricuspid valves, low cardiac output, and left or right atrial spontaneous echo contrast.2 However, a coexisting disease favoring thrombus formation cannot exclude a possible myxoma.3 Mitral stenosis is one of the major risk factors for an intracardiac thrombus. It is possible for a large LA mass to worsen the mitral pathology.
Left atrial myxomas most often originate from the fossa ovalis, which differentiates them significantly from LA thrombi, typically occurring in the LA appendage.3,5 In our case, there was a separate small thrombus in the LA appendage, but it was not associated with the bigger mass that originated from the septal wall.
A differential diagnosis between a thrombus and myxoma can be difficult because they share numerous known characteristics. It is also possible that a thrombus overlies a myxoma.4 In our case, the mass showed no late contrast enhancement on MRT, and it had a lobular structure, smooth edges, and an oval shape. All these features can be associated with both masses.5 The factors favoring a thrombus were the existing structural heart disease, a separate mass in the LA appendage, multiple lesions, and a sessile base. Factors favoring a myxoma were the large size of the mass, location on the septal wall, and the absence of LA spontaneous echo contrast on transthoracic echocardiography.
Lessons to be learned
In our patient, there were slightly different findings on transthoracic echocardiography and computed tomography or MRT. Our report suggests that an interdisciplinary team, including radiologists who would interpret the different imaging studies performed, could be valuable in more complex cases of differentiation between intracardiac masses. It also suggests that anticoagulation treatment should be attempted and a repeated radiological evaluation of an LA mass and mitral pathology should be considered before establishing the final diagnosis, in order to avoid an unnecessary cardiac surgery.
- Lee W, Huang MP, Fu M. Multiple intracardiac masses: myxoma, thrombus or metastasis: a case report. J Med Case Rep. 2015; 9: 179. | Crossref
- Jang KH, Shin DH, Lee C, et al. Left atrial mass with stalk: thrombus or myxoma? J Cardiovasc Ultrasound. 2010; 18: 154‑156. | Crossref
- Sim EK, Lim YT, Ng WL, et al. Co‑existing left atrial thrombus and myxoma in mitral stenosis – a diagnostic challenge. Singapore Med J. 1999; 40: 46‑47.
- Turhan S, Ozcan OU, Erol C. Imaging of intracardiac thrombus. Cor et Vasa. 2013; 55: 176‑183. | Crossref
- Scheffel H, Baumueller S, Stolzmann P, et al. Atrial myxomas and thrombi: comparison of imaging features on CT. Am J Roentgenol. 2009; 192: 639‑645. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION