Adrenocortical carcinoma mimicking pheochromocytoma on iodine 123–labeled metaiodobenzylguanidine scintigraphy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Adrenocortical carcinoma mimicking pheochromocytoma on iodine 123–labeled metaiodobenzylguanidine scintigraphy
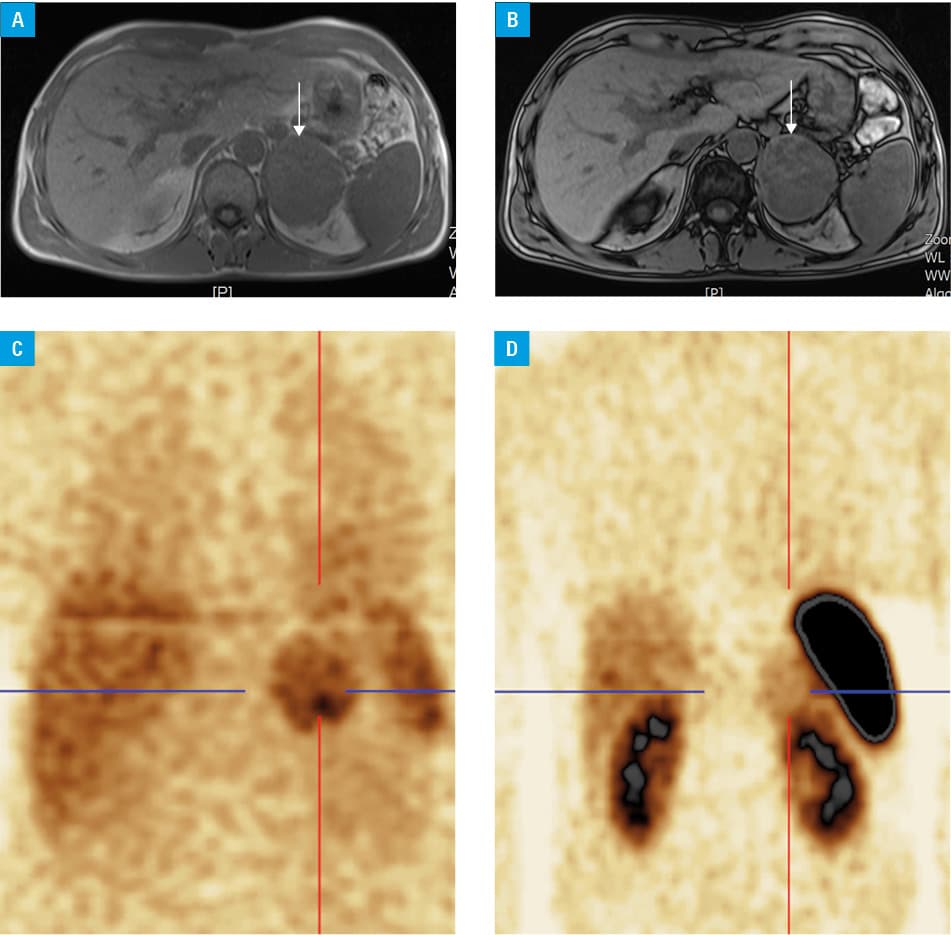
A 39‑year‑old man with decompensated hypertension of up to 190/100 mm Hg was admitted to our department of endocrinology due to bilateral adrenal tumors revealed by ultrasonography and computed tomography (CT) of the abdomen. Noncontrast attenuation of the 63‑mm left adrenal tumor was 35 HU, and its absolute (APW) and relative (RPW) percentage washouts at delayed contrast‑enhanced CT (delay, 10 min) were 60% and 30%, respectively, while for the smaller 23‑mm right adrenal tumor—98% and 77%, respectively. Chemical‑shift magnetic resonance imaging (MRI) classified the left adrenal tumor as nonadenoma, as no signal loss occurred in the out‑of‑phase sequence (Figure 1A and 1B). Hypercortisolism and hyperaldosteronism were excluded, but the urinary levels of methoxycatecholamines were 916 μg/24 h and 953 μg/24 h and remained in the upper limit of normal (up to 1000 μg/24 h). Iodine 123–labeled metaiodobenzylguanidine (123I‑MIBG) scintigraphy was carried out 6 hours after the patient had been given a 380‑MBq intravenous bolus injection of the radiotracer. It involved whole‑body scanning complemented by single‑photon emission CT (SPECT) centered on the lower part of the head, abdomen, and pelvis. The examination was performed with the E.cam imaging equipment (Symbia E SPECT gamma camera, Siemens Healthineers, Hoffman Estates, Illinois, United States) and showed an increased heterogeneous uptake in the left adrenal gland (Figure 1C). Somatostatin‑receptor scintigraphy with 630 MBq of technetium 99m–labeled hydrazinonicotinyl‑Tyr3‑octreotide gave similar results (Figure 1D).
Based on imaging and biochemical evaluation, a suspicion of pheochromocytoma (PCC) was raised and the patient underwent a surgery after 2 weeks of α-blocker intake. After that, the pathology report, verified by 2 well‑trained pathologists, revealed a 71‑mm adrenocortical carcinoma (ACC), which stained negative for chromogranin. Additional staining showed type 2 and 5 somatostatin receptors. Currently, 2 years after the initial diagnosis, the patient remains on mitotane treatment and has no signs of recurrence.
Scintigraphy is used in the diagnostic workup of adrenal disorders and is especially helpful when the diagnosis cannot be determined by CT or MRI.1 In the presented case, the clinical and biochemical evaluation, high density on unenhanced CT, normal APW on delayed contrast‑enhanced CT, and no lipids on MRI suggested PCC (approximately 25% of PCCs have a high APW and/or RPW value).2 In clinical practice, functional imaging with 123I‑MIBG can be useful in confirming the diagnosis of PCC.3 Radiotracer uptake in chromaffin cells occurs through passive diffusion and norepinephrine transporters. The tracer is then accumulated in the secretory granules of the cells via vesicular monoamine transporters.4 Although 123I‑MIBG scintigraphy (with SPECT) has high specificity (95%–100%) and sensitivity (83%–100%), false‑positive results do occasionally occur.3-5 Tumors that mimic PCC include adrenal adenoma, retroperitoneal angiomyolipoma, hemangioma, malignant lymphoma, hepatocellular carcinoma, and other neuroendocrine tumors not derived from chromaffin cells, such as medullary thyroid carcinoma, carcinoid tumors, Merkel cell carcinoma, or ganglioneuroma. An increased MIBG uptake was also described in 2 cases of ACC.4,5 It is speculated that it may be caused by passive diffusion of the radiotracer due to increased blood flow, but the underlying mechanisms are still incompletely understood. Nevertheless, these are extremely rare cases and they do not discredit the usefulness of 123I‑MIBG scintigraphy in diagnosing PCC. However, other adrenal lesions should be considered if an increased heterogeneous or inadequate radiotracer uptake is detected due to a large tumor mass.
- Łebek‑Szatańska A, Nowak KM, Papierska L. Usefulness of scintigraphy imaging in the diagnostics of adrenal disease . Postępy Nauk Medycznych. 2017; 30: 707‑716.
- Canu L, Van Hemert JAW, Kerstens MN, et al. CT characteristics of pheochromocytoma: relevance for the evaluation of adrenal incidentaloma. J Clin Endocrinol Metab. 2019; 104: 312‑318. | Crossref
- Taïeb D, Timmers HJ, Hindié E, et al. EANM 2012 guidelines for radionuclide imaging of phaeochromocytoma and paraganglioma. Eur J Nucl Med Mol Imaging. 2012; 39: 1977‑1995. | Crossref
- Jung HS, Moon SJ, Kim YM. False positive radioiodinated metaiodobenzylguanidine (123I‑MIBG) uptake in undifferentiated adrenal malignant tumor. Case Rep Oncol Med. 2015; 2015: 164280. | Crossref
- Rainis T, Ben‑Haim S, Dickstein G. False positive metaiodobenzylguanidine scan in a patient with a huge adrenocortical carcinoma. J Clin Endocrinol Metab. 2000; 85: 5‑7. | Crossref
ARTICLE INFORMATION