Use of bedside ultrasound to assess fluid status: a literature review
Key words: carotid Doppler ultrasound, inferior vena cava/abdominal aorta index, point-of-care ultrasound, transthoracic lung ultrasound, volume status



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Use of bedside ultrasound to assess fluid status: a literature review
The assessment of a patient’s body fluid status is a challenging task for modern clinicians. Ultrasonography has numerous advantages, the most important being reproducibility and bedside monitoring of the patient. The examination is quick and has a significant diagnostic value. We reviewed the literature to assess the possibility of using ultrasound methods for evaluating body fluid status. The search of PubMed and Medline databases was performed up to February 2019. Data from published reports and clinical observations show that the quick and noninvasive ultrasound examination facilitates the assessment of intravascular volume status and that the results correlate with other modalities, including invasive methods. Ultrasound enables physicians to determine the baseline status of hydration and to monitor the patient during fluid therapy. Additionally, it allows an assessment of asymptomatic patients, patients who are well adapted to chronic oxygen deficiency, and those who develop pulmonary congestion secondary to congestive heart failure or chronic kidney disease. The development of a protocol for an ultrasound assessment of the volume status would significantly facilitate the everyday practice of internal medicine specialists.
Introduction
Despite rapid advancements in medicine, regulation of body fluid volume remains a key concern for modern clinicians. From the pathophysiologic perspective, it is most important to assess intracellular water volume as it directly impacts arterial and venous pressure, volume status, and, consequently, life functions of the body. There is a considerable spectrum of available modalities to assess intracellular water volume: from a clinical evaluation of vital signs to advanced invasive methods, such as pulmonary artery catheterization.1 The point‑of‑care ultrasound is currently used to assist clinicians in problem solving at bedside, and one of the challenges involved is the evaluation of intravascular volume status. This method allows for a real‑time and noninvasive assessment of the degree of hydration, and owing to its reproducibility, it is also suitable for monitoring. The results of the ultrasound assessment of the degree of hydration correlate with those obtained with other referential methods.2Moreover, the method is easy to learn even for inexperienced clinicians.3
Ultrasound assessment of the inferior vena cava
Method (equipment, technique)
An ultrasound device to assess fluid status should be equipped with a convex or phased array probe. The selection of an adequate probe depends on the patient’s physique. Convex and phased array probes are effective for in‑depth examination of tissues (about 25–30 cm). This enables an assessment of the inferior vena cava (IVC) and aorta (Ao) when the probe is placed over the epigastric region and over the right lateral abdominal wall. The standard placement of the probe to visualize both vessels is in the anterior median line over the epigastrium (inferior to the xiphoid process). In cases when the assessment over the epigastrium is difficult (eg, due to substantial amounts of intestinal gas, large dressings or wounds in the median line), the probe should be placed over the lateral abdominal wall, in the right anterior axillary line. An assessment with the probe placed over the lateral abdominal wall can be very effective because the liver is a perfect acoustic window for the imaging of the major abdominal vessels. The Color Doppler mode is not required for the evaluation of fluid status. The examination involves only the assessment of the vein diameter, and in the case of the IVC/Ao index, it also involves calculating the ratio of the IVC diameter to the aorta diameter.
First, the IVC collapsibility is assessed. The maximal and minimal IVC diameters are measured, using the M‑mode, during the expiratory and inspiratory phases of the respiratory cycle. The obtained results are computed according to the following formula: dIVC = ([Dmax – Dmin]/Dmax) × 100%, where d stands for distensibility (collapsibility); Dmax, maximal diameter; and Dmin, minimal diameter. In fluid‑responsive patients, the value of the IVC collapsibility exceeds 40%. Patients who do not respond adequately to fluid therapy have the IVC collapsibility index of less than 15%. Moreover, the IVC collapsibility index exceeding 50% is strongly associated with low values of the central venous pressure.4
The value of the IVC/Ao index is obtained by calculating the ratio of the IVC to Ao diameters. The IVC diameter is assessed in the intrahepatic segment, about 3 cm below the diaphragm, during the expiration phase of the respiratory cycle. The Ao diameter is measured at the same level by moving the probe with a swinging motion to the left of the patient’s body. A normal value of the IVC/Ao index ranges from approximately 0.8 to 1.2. The IVC/Ao index of less than 0.8 indicates that the patient requires fluid therapy, while the value of more than 1.2 indicates that the patient is most likely overhydrated.
For patients undergoing respiratory therapy, the assessment of the IVC compressibility is helpful. Technically, the examination is analogous to the assessment of the IVC collapsibility index by measuring the minimal and maximal diameters in the M‑mode. However, to assess the volume status, the so‑called IVC compressibility index is calculated using the following formula: IVC compressibility index = ([Dmax – Dmin]/Dmax) × 100%. The threshold of the IVC compressibility index is 18%. The use of this threshold allows a classification of patients into those potentially responsive (>18%) and nonresponsive (<18%) to fluid therapy.5,6
Clinical usefulness of the inferior vena cava/aorta index and the inferior vena cava index
The calculation of the IVC collapsibility and IVC/Ao indices is an auxiliary modality in determining the degree of the patient’s hydration. The indexes are particularly useful when the clinical assessment is difficult and may fail to provide adequate results. To determine body fluid status in adults with the use of ultrasoography, initially the IVC collapsibility was evaluated.7,8 The measurement of the IVC diameter on expiration and inspiration as well as its collapsibility ratio yields the so‑called IVC index. The usefulness of the IVC/Ao index was initially confirmed in the pediatric population.3,9Currently, both the IVC index and the IVC/Ao index are well documented as useful measurements in assessing body fluid status in adult patients.10-12One of the basic differences between the 2 methods is the impact of the patient’s individual characteristics, such as age, sex, height, body surface, body mass, and waist circumference. The IVC/Ao index is more susceptible to patient characteristics than the IVC index.12 Rahman et al13 and Lyon et al14 proved the efficacy of the IVC and IVC/Ao indices and demonstrated that they can be used as parameters for detecting an early phase of hypovolemic shock. However, the sensitivity of the IVC index in detecting early blood loss does not exceed 80%.15Additionally, the IVC/Ao index has been found to be useful for the evaluation of preoperative and intraoperative volume status, especially in a major surgery with marked fluid shift or blood loss.16
Other target groups for the application of ultrasonography in the assessment of body fluid status are patients with cardiovascular diseases, for example, those with exacerbation of congestive heart failure (HF), kidney diseases (such as acute kidney injury and exacerbation of chronic kidney disease [CKD]), as well as patients on dialysis. In these populations, the assessment of the initial body fluid status is essential, but more importantly, these patients should be carefully monitored during fluid therapy or fluid removal.
Limitations of the inferior vena cava/aorta index and the inferior vena cava index
The usefulness of ultrasound in the measurement of the IVC and IVC/Ao indices is limited by its high dependence on the experience of the operator and the presence of specific clinical conditions that prevent a reliable calculation, including pulmonary hypertension, elevated intra‑abdominal pressure, cardiac tamponade, and mechanical ventilation. Pathological obesity can be an obstacle to assessing the IVC diameter. When hypervolemia is detected, false‑positive results should be considered due to pulmonary hypertension, high intra‑abdominal pressure, or cardiac tamponade. The operator’s experience and ability to obtain optimal views are of key significance in a correct assessment of body fluid status. As in the case of any examination, training and gaining experience through practice are essential. Due to the high reproducibility of ultrasound examinations, especially when monitoring the patient, it is advisable that the examination is conducted by a clinician who is the treating physician.
Lung ultrasound in the assessment of body fluid status
Method (equipment, technique)
In a lung ultrasound examination, a convex probe is most often employed for the preliminary assessment, and a linear probe, for the visualization of small subpleural lesions and the pleural line.17 The linear probe helps differentiate B‑line artifacts, for example, irregularities, fragmentation, or the blurring of the pleural line in pulmonary fibrosis. In emergency cases, phased array probes are used as an extension of echocardiography (additionally, a small probe head facilitates intercoastal access) as well as micro‑convex probes.18,19The assessment of body fluid status is based on the analysis of artifacts. Consequently, it is necessary to switch off additional options improving visualization such as compound imaging, algorithms that reduce speckle, haze, and clutter artifacts, as well as harmonic imaging.
Features of the ultrasound device that facilitate bedside examination include a small size, a few‑second switching time, and an easily cleaned transducer. Additionally, Doppler options are not required. Modern pocket‑size imaging devices seem to be useful tools for assessing the lungs.20
In recumbent patients, when searching for B‑line artifacts, the region along the middle and posterior axillary lines is mainly assessed. In the case of patients mainly in the erect position, in order to search for interstitial and alveolar‑interstitial syndromes, first the lower lung fields are assessed. Then, the level up to which B‑line artifacts are present is analyzed by moving the probe up to the middle and upper lung fields. This examination technique is a result of the gravitation‑dependent presence of air and fluid. There are numerous imaging protocols that can be used for lung examination. The best‑known protocol is the evaluation of 8 regions. An anterior 2‑region scan may be sufficient to exclude interstitial syndrome in cardiogenic acute pulmonary edema.21
Lung ultrasound facilitates the assessment of extravascular lung water.22It has been proved that the degree of lung aeration, dependent on the fluid volume in the interstitial and interalveolar spaces, directly correlates with the ultrasound image.23Extravascular lung water assessment can be reliable and effective irrespective of the operator’s experience in lung ultrasound.24 Another important feature of extravascular lung water is the symmetric bilateral localization of the lesions. B‑line artifacts detected unilaterally may correspond to different processes within pulmonary interstitial spaces (eg, inflammation), and the presence of fluid in the interstitial and interalveolar spaces usually produces a symmetrical image on both sides of the chest.
Artifact analysis
Ultrasound assessment of body fluid status involves the analysis of artifacts seen on an ultrasound image.
A‑line artifacts
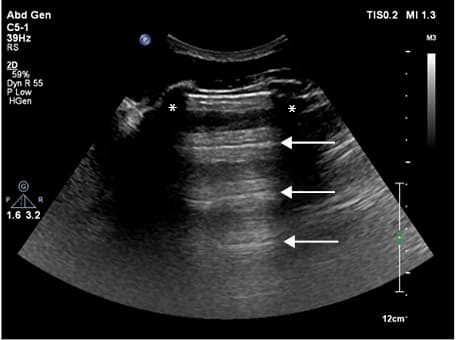
In a normal aerated lung, ultrasound images show A‑line artifacts. A lines are horizontal regularly spaced lines and a type of reverberation artifacts that appear between 2 bordering surfaces: the probe/body surface and the pleura/air in the alveoli. The distance between A lines is equal.25 When fluid status is assessed, such an image is interpreted as the so‑called dry lung.26An image showing A‑line artifacts may be also seen in pneumothorax; however, the pleural sliding sign is then absent (Figure 1).
B‑line artifacts
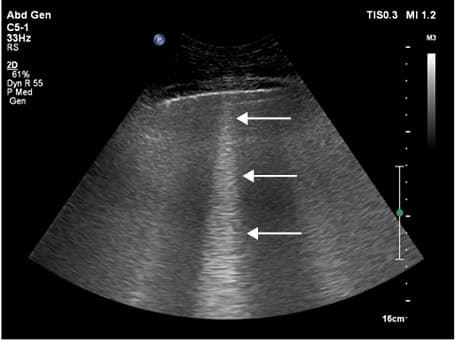
The major reason for B‑line artifacts is the presence of fluid in the interstitial or interalveolar spaces. These artifacts can also be found in pneumonia and fibrosis.27B‑line artifacts are caused by a reverberation phenomenon. The area where reverberation occurs covers a small space—the interlobular septa or pulmonary alveoli. Consequently, the obtained image shows an apparent vertical line consisting of numerous small horizontal lines.28B‑line artifacts are defined as laser‑like vertical hyperechoic reverberation artifacts that arise from the pleural line, extend to the bottom of the screen (without fading irrespective of the programmed depth of penetration), and move synchronously with the respiratory cycle (Figure 2).29
Depending on the fluid volume in the lung, B‑line artifacts produce:
1 The interstitial syndrome, corresponding to the presence of fluid in the interstitial spaces. Three or more B‑line artifacts are present within a single intercostal window with a longitudinal probe position. The distance between them is larger than 7 mm, which results from the anatomical structure and equates the thickness of interlobular septa. B‑line artifacts move synchronously with the respiratory cycle and pleural sliding and remain separated.26
2 The alveolar‑interstitial syndrome, corresponding to the presence of fluid in the interstitial and interalveolar spaces. The distance between the artifacts is 3 mm, and B‑line artifacts overlap synchronously with the respiratory cycle.25
3 The white lung sign, a completely white image of the lung, without visible single artifacts, corresponding to large fluid volumes within the alveolar‑interstitial spaces, the next stage being airless consolidation.29
Clinical usefulness of lung ultrasound in heart failure
In everyday clinical practice, the assessment of HF exacerbation is based on clinical examination, chest radiography, N‑terminal fragment of the prohormone brain natriuretic peptide (NT‑proBNP) levels, and echocardiography.30,31 Physical examination is still the initial diagnostic modality. However, it does not yield reliable results in asymptomatic patients and does not allow for a precise assessment of the degree of HF exacerbation.32 In asymptomatic patients, lung ultrasound facilitates the detection of pulmonary congestion, which in the early stage does not present any signs on auscultation. Crackles over the lung fields appear only when the fluid volume is large enough to be present in the interalveolar space. Additionally, the number of B‑line artifacts in HF increases synchronously with an increase of the New York Heart Association (NYHA) functional class and is directly dependent on the ejection fraction and degree of diastolic dysfunction.19 Moreover, a stable number of B‑line artifacts was observed in patients who, despite their heart disease, retained a stable level of exercise capacity.19In HF exacerbation, lung ultrasound is employed to monitor the resolution of pulmonary congestion and treatment efficacy, and the results correlate directly with NT‑proBNP levels and radiologic examinations.33Lung ultrasound is also useful in monitoring patients with pulmonary congestion who undergo intensive diuretic therapy or hemodialysis.34,35 A meta‑analysis of 7 large‑scale studies indicated that lung ultrasound differentiates cardiogenic and noncardiogenic dyspnea with a sensitivity of 94% and specificity of 92% in emergency department patients.36Moreover, a multicenter study revealed that the analysis of B‑line artifacts is more accurate in detecting acute decompensated HF than a clinical workup, chest radiography, or NT‑proBNP levels.37
Clinical usefulness of lung ultrasound in renal failure and dialysis therapy
Fluid overload is one of the most important prognostic factors in patients with CKD. Hypervolemia results in left ventricular (LV) hypertrophy. More than one‑third of patients undergoing dialysis die of cardiovascular incidents (arrhythmia, myocardial infarction). The most common causes of cardiovascular incidents include LV hypertrophy and arterial hypertension.38-40 A successful control of extracellular volume in patients on chronic dialysis allows clinicians to monitor arterial blood pressure, largely reducing or even eliminating the use of antihypertensive drugs.41
In patients on dialysis, fluid balance is still controlled on the basis of physical examination, assessment of the so‑called dry weight, and the measurement of arterial blood pressure.42Such an evaluation is not reliable as it involves parameters that depend on too many factors—consider, for example, the amount of fluid volume change necessary to obtain an alteration in arterial pressure, peripheral edema, and cardiac function.
In hemodialyzed patients, the number of B‑line artifacts before and after dialysis directly correlates with the measurements of the IVC diameter and bioelectrical impedance analysis. This correlation was revealed in both asymptomatic and symptomatic patients in all NYHA classes.43,44 Additionally, lung ultrasound appears to be an effective tool for detecting and monitoring patients with HF and CKD who develop pulmonary congestion despite the absence of symptoms. The use of lung ultrasound for monitoring in this population may reduce the risk of decompensated HF, which is the most frequent cause of death in patients on dialysis.43The use of the B‑line score defined as the percentage of regions where B lines are present also correlates with the extravascular lung water before and after hemodialysis.45,46 In patients undergoing peritoneal dialysis, lung ultrasound enables a determination of extravascular lung water, especially in asymptomatic individuals.47
Lung ultrasound limitations
Lung ultrasound is a relatively new modality for the assessment of body fluid status. It is an easy‑to‑use tool but has some limitations.48 It may prove problematic in patients who have undergone pneumonectomy. B‑line artifacts are found in many different clinical conditions including cardiogenic and noncardiogenic pulmonary edema, pneumonia, interstitial lung disease, and lymphangitis carcinomatosa. It is extremely important for the operator to differentiate between these conditions. The assessment of lesion distribution, localization of B‑line artifacts, regularity of B‑line artifact distribution, as well as the pleural line and associated lesions may help determine whether the condition is cardiogenic or lung related.18,19,49,50It should be noted that in the population of hemodialyzed patients with HF, the assessment may be limited.51 The development of guidelines and an algorithm for the assessment of body fluid status with lung ultrasound that would allow physicians to refer the examination to the general population would be an important step.
Usefulness of echocardiography in assessing body fluid status
Method (equipment, technique) and clinical significance
To assess the heart, a phased array probe is necessary. The ultrasound device must be equipped with a color Doppler mode. Portable and pocket‑size devices are much more frequently used at present. The phased array probe allows an optimal visualization of a single intercostal window due to the small surface of the probe head. During the examination, the patient is placed in the left lateral decubitus position, with the left arm abducted to widen the intercostal spaces. The assessment is performed in the following views: parasternal long axis (the probe is placed at the third or fourth intercostal space, just lateral to the left sternal border); parasternal short axis (the probe is placed as above, rotated by 90°), and apical (the probe is placed over the expected apex of the heart).
Left ventricular stroke volume correlates closely with the right ventricular filling pressure. The volume parameter, LV end‑diastolic volume, represents well the amount of intravascular volume lost. However, its calculation is time consuming, so a different parameter, LV end‑diastolic area (LVEDA), has been applied instead. Additionally, the analysis of LV outflow tract (LVOT) velocity time integer (VTI) has been proved useful in the assessment of fluid responsiveness.50,52
The LVEDA is measured at the mid‑papillary level in the left parasternal short‑axis view. It is important to perform the measurement in the plane perpendicular to the LV axis. The LVEDA values of less than 10 cm2 indicate hypovolemia, and the values exceeding 20 cm2 suggest hypervolemia.53,54 In extreme hypovolemia, the obliteration of the LV cavity can be observed, known as “kissing ventricles.” Then the LVOT in the apical 3- and 5‑chamber views is assessed. The sample gate should be placed about 10 mm from the level of the aortic valve (towards the LV lumen), in the center of the outflow tract. The obtained outflow tract should be outlined, thus automatically providing the value of LVOT VTI. The LVOT VTI is a good predictor of a potential fluid responsiveness. An increase in LV systolic volume of more than 12% is considered a positive response to fluid therapy,54 while an increase of less than 10% indicates a weak response.55 Additionally, an increase of the LVOT VTI of more than 12.5% after a passive leg raising maneuver (elevation to 45°, measurement taken after 1 minute) is indicative of fluid responsiveness.
Limitations of ultrasound heart assessment
When measuring the LVOT, the patient must be in sinus rhythm. The administered volume of fluid must be adequate in order to avoid false‑negative results, and it should amount to about 8 ml/kg. In obese individuals, patients with breast implants, and those with severe emphysema, it may be difficult to obtain views with standard placements of the probe. Echocardiography is largely dependent on the operator’s skills, and a considerable experience is needed to obtain diagnostic views.
Ultrasound of the carotid arteries in the assessment of body fluid status
Method (equipment, technique)
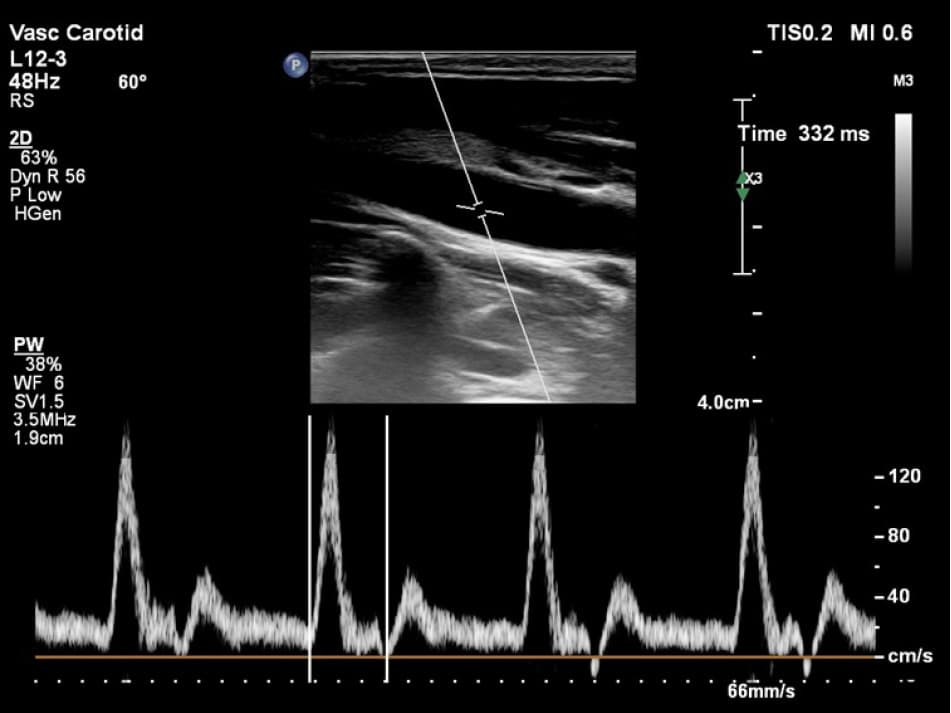
Corrected carotid flow time refers to the time length of blood flow through the common carotid arteries (CCAs) during systole, corrected for heart rate: time/√cycle time.56 This time is measured from the beginning of the systole to the beginning of diastolic flow. The measurement is taken with a linear probe placed at the level of the lower lobe of the thyroid, visualizing CCAs in the longitudinal plane (Figure 3). The Doppler gate is placed analogously to the regimen appropriate for other vessels. Hooman et al57 reported no significant differences between measurements taken on the right and left CCAs, which additionally increases diagnostic possibilities, for example, in patients who have a central venous catheter or neck injuries.
Clinical usefulness of the ultrasound assessment of the common carotid arteries
Blehar et al58 demonstrated that the corrected carotid flow time increases in dehydrated patients who received intravenous fluids. Additionally, the corrected flow time (FTc) changed in patients undergoing dialysis therapy. The FTc measured in milliseconds was significantly shorter as compared with the values obtained before the administration of hemodialysis. Moreover, Hooman et al56 demonstrated that this difference correlated with the volume of fluid removed by hemodialysis. Investigators also attempted to determine the reference and cutoff values for FTc.57 They revealed that FTc changes even with relatively small alterations in the intravascular volume status.
Limitations of vascular ultrasound assessment
In patients with arrhythmias, it is necessary to assess several cardiac cycles.59 Further studies are needed to determine reference values for large populations. Studies conducted to date have demonstrated that the differences depend on sex, among other factors.57 No data are available for FTc in patients with anomalies of the CCA.
Summary
Ultrasonography appears to be a useful tool for the assessment of body fluid status. Data from published reports and clinical observations prove that the quick and noninvasive ultrasound examination facilitates the evaluation of intravascular volume status, and the results correlate with other modalities, including invasive methods.60Miniaturization of ultrasound devices have diminished the obstacles to bedside assessment, allowing a reproducibility of the examination in order to monitor, for example, fluid responsiveness. Some issues associated with ultrasound assessment still require further studies, for example, to establish the examination protocol and the range of reference values. It seems that the near future will witness a breakthrough in ultrasound diagnostics of hypervolemia and hypovolemia, thus providing clinicians with an invaluable tool to administer and monitor fluid therapy safely as well as to control fluid deficiency (Table 1).
Ultrasound assessment | Advantages | Disadvantages |
Inferior vena cava | Sensitive in hypovolemia | Limitations: morbid obesity |
Easy to perform | Dependent on right ventricular function, respiratory, intra‑abdominal pressure | |
Correlated with other objective methods | ||
Lung ultrasound | Easy to perform | Level of hypovolemia cannot be evaluated |
Sensitive in hypervolemia | B‑line artifacts are found in numerous diverse conditions: noncardiac edema (acute respiratory distress syndrome, viral pneumonia, aspiration pneumonia), interstitial lung disease | |
Echocardiography | Reliable | Diagnostic views require considerable operator’s experience |
Sensitive, especially in hypervolemia | Requires a set of skills | |
Carotid arteries | Correlated with other objective methods | Requires further studies for standardization |
Commentary
Available literature reports indicate that ultrasound assessment is a reliable source of information on body fluid status. A large number of data can be obtained from various areas assessed by ultrasound examinations. A convex probe is necessary to assess the IVC/Ao index, IVC collapsibility index, and the lungs. In ambiguous cases, phased array and linear probes should be used to assess the heart and vessels. This, however, requires an access to a set of 3 probes as well as expertise in echocardiography. It is important that the examination is performed by a clinician who is the patient’s diagnostician and treating physician. Moreover, the interpretation of the images should be based on information obtained from the assessment of the patient’s general condition and results of additional tests. Available studies confirm a positive correlation between the assessment of the IVC/Ao index, IVC index, and the lungs and referential methods.11,12,31Echocardiographic assessment requires a skilled operator. Normally, to assess the heart, a phased array probe is used. However, due to the frequent need to examine a patient at bedside, especially in the case of critically ill patients, it is necessary to perform the examination with the use of a single universal probe, for example, a convex probe.61 Lichtenstein62 argued for the efficacy of a micro‑convex probe to assess individuals with dyspnea or critically ill patients. Due to its small head, it allows an optimal visualization of the intercostal spaces. Additionally, its penetration depth makes it possible to assess the vessels in the retroperitoneal space. From a technical point of view, a portable or pocket‑size device with a convex or micro‑convex probe seems to be optimal for a quick examination and continuous monitoring. In our clinical practice, we use single probe placement without performing complete procedures. The time needed to determine the patient’s hydration status should not exceed 2 minutes.
Monitoring fluid responsiveness in patients who require bedside diagnostics is based on multiorgan assessment: the IVC diameter, heart, and lungs. First, the IVC/Ao index or the IVC index is calculated. The IVC/Ao index of less than 0.8 or the IVC index exceeding 40% (or both) indicates that the intravascular volume is too low and fluid therapy is needed. The IVC/Ao index exceeding 1.2 or the IVC index lower than 15% (or both) usually indicates intravascular volume overload. The IVC assessment indicates the need for fluid therapy.
It is also possible to assess the heart using a convex probe. The LVEDA can be measured, with the values of less than 10 cm2 indicating hypovolemia and of more than 20 cm2 indicating hypervolemia.53,54In the case of severe hypovolemia, ventricular walls are clearly touching each other (“kissing ventricles”). Additionally, the ratio of the right to LV end‑diastolic diameter exceeding 0.6 is indicative of right ventricular overload.63 With access to a phased array probe, LVOT VTI analysis before and after fluid therapy can be performed to demonstrate fluid responsiveness.50,52
When assessing the lungs, it is especially important to visualize A- and B‑line artifacts during fluid therapy. If A‑line artifacts are present bilaterally, the resulting image presents the so‑called “dry lung.” Fluid therapy may be administered, although such an image is not an indication for fluid therapy, but serves as a green light for therapy administration when there are other indications. When B‑line artifacts are present bilaterally, the so‑called “wet lung” is visible, corresponding to pulmonary congestion. In this case, fluid therapy may only worsen the patient’s condition and it is contraindicated in such cases.20
Finally, the measurement of the carotid blood flow seems to be a promising parameter for the assessment of body fluid status; however, the reference range needs to be established first.
- Ginosar Y, Sprung CL. The Swan‑Ganz catheter. Twenty‑five years of monitoring. Crit Care Clin. 1996; 12: 771‑776. | Crossref
- Ekinci C, Karabork M, Siriopol D, et al. Effects of volume overload and current techniques for the assessment of fluid status in patients with renal disease. Blood Purif. 2018; 46: 34‑47. | Crossref
- Kosiak W, Swieton D, Piskunowicz M. Sonographic inferior vena cava/aorta diameter index, a new approach to the body fluid status assessment in children and young adults in emergency ultrasound – preliminary study. Am J Emerg Med. 2008; 26: 320‑325. | Crossref
- Nagdev AD, Merchant RC, Tirado‑Gonzalez A, et al. Emergency department bedside ultrasonographic measurement of the caval index for noninvasive determination of low central venous pressure. Ann Emerg Med. 2010; 55: 290‑295. | Crossref
- Barbier C, Loubieres Y, Schmit C, et al. Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004; 30: 1740‑1746. | Crossref
ARTICLE INFORMATION