Predictors of appropriate interventions and mortality in patients with implantable cardioverter-defibrillators
Key words: appropriate intervention, implantable cardioverter-defibrillator, mortality, predictorsEdiTOrial



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Predictors of appropriate interventions and mortality in patients with implantable cardioverter-defibrillators
Introduction: Additional risk assessment in patients with heart failure referred for implantable cardioverter‑defibrillator (ICD) implantation as primary prevention is needed. A reduction in left ventricular ejection fraction (LVEF) seems to lack sufficient sensitivity and specificity to be used for identification of patients at the highest risk of sudden cardiac death.
Objectives: The aim of this study was to identify short- and long‑term predictors of appropriate implantable cardioverter‑defibrillator therapy as well as predictors of long‑term mortality in patients with an ICD or cardiac resynchronization therapy defibrillator (CRT‑D).
Patients and methods: In this retrospective study, data from 457 patients who had an ICD or CRT‑D implanted between 2011 and 2017 were analyzed.
Results: During the median follow‑up of 31 months (interquartile range, 17–52 months), 153 patients died (33.9%) and 140 had appropriate interventions (31%). In a multivariate Cox regression analysis, implantation for secondary prevention (hazard ratio [HR], 2.49; P <0.001), severe mitral valve disease (HR, 2.17; P <0.001), and previous myocardial infarction (HR, 1.68; P = 0.009) were predictors of appropriate intervention. Resynchronization therapy (HR, 0.59; P = 0.025) and severe mitral valve disease (HR, 2.42; P <0.001) were predictors of appropriate intervention in primary prevention. Body mass index, hemoglobin concentrations, LVEF, diabetes, and left atrial diameter were significant predictors of death.
Conclusions: Implantation of ICD or CRT‑D as secondary prevention was a potent predictor of appropriate intervention, while resynchronization therapy and severe mitral regurgitation predicted ICD therapy in primary prevention. In patients with ICD or CRT‑D, independent predictors of mortality included: body mass index, hemoglobin concentrations, LVEF, diabetes, and left atrial diameter.
What's new?
We aimed to identify risk factors of cardiac events in patients with an implantable cardioverter‑defibrillator or cardiac resynchronization therapy defibrillator (ICD/CRT‑D). We found that diabetes and increased left atrial diameter were associated with the risk of mortality, while higher body mass index, hemoglobin levels, and left ventricular ejection fraction had a protective effect. Secondary prevention and severe mitral valve disease had a significant effect on the incidence of appropriate ICD therapy. Patients with resynchronization therapy had lower odds of appropriate ICD intervention.
Introduction
Although there are no controversies regarding implantable cardioverter‑defibrillator (ICD) implantation for secondary prevention of sudden cardiac death, additional risk assessment is needed in patients referred for ICD or cardiac resynchronization therapy defibrillator (CRT‑D) implantation as primary prevention. In the light of the DANISH trial (Danish ICD Study in Patients With Dilated Cardiomyopathy),1 a reduction in left ventricular ejection fraction (LVEF) does not appear to be a sufficiently sensitive and specific marker for identifying patients at the highest risk of sudden cardiac death.1
The contemporary population with ICD or CRT‑D differs from the populations included in landmark trials (MADIT [Multicenter Automatic Defibrillator Implantation Trial],2 SCDHeFT [Sudden Cardiac Death in Heart Failure Trial],3 and COMPANION [Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure]).4 This is due to differences in current pharmacotherapy and a wider use of revascularization therapy, especially in acute myocardial infarction. Moreover, consecutive patients in everyday practice may also differ from those included in clinical trials.
Only one‑third of patients implanted with an ICD or CRT‑D receive appropriate therapies.5,6 In some reports, this rate was as low as 1% per year in patients undergoing implantation for primary prevention.7 The remaining patients do not benefit from ICD or CRT‑D implantation but are at risk of complications, such as infections, device or lead malfunctions, and inappropriate interventions. In everyday life, the most common difficulties are due to upper limb movement limitations or possible electromagnetic field interference. Therefore, further studies are needed to establish the best treatment strategy for patients with heart failure and reduced LVEF in everyday clinical practice.
The aim of our study was to identify short- and long‑term predictors of appropriate ICD therapy in an unselected cohort of patients implanted with an ICD or CRT‑D, particularly in primary prevention. We also sought to identify predictors of long‑term mortality in these patients.
Patients and methods
Study design and patients
This was a retrospective study based on data of consecutive patients implanted with an ICD or CRT‑D in the Military Institute of Medicine in Warsaw, Poland, between January 2011 and December 2017. The devices were implanted according to contemporary guidelines.8,9 Numerous clinical factors were analyzed, including indications for implantation (primary or secondary prevention), etiology of heart failure (ischemic or nonischemic), New York Heart Association functional class at baseline, comorbidities (diabetes, hypertension, pulmonary disease, stroke, and atrial fibrillation), as well as coronary interventions (percutaneous coronary intervention, coronary artery bypass grafting) prior to implantation. We also compared baseline hemoglobin concentrations and renal function (serum creatinine and estimated glomerular filtration rate [calculated using the Modification of Diet in Renal Disease formula]),10 assessed at the time of implantation.
Echocardiography
All patients underwent 2‑dimensional echocardiography before device implantation. Echocardiography was performed using standard parasternal, apical, and subcostal views (2.5‑MHz transducer; VIVID S6 and S7, GE Medical Systems, Wauwatosa, Wisconsin, United States). The left atrial and left ventricular end‑diastolic diameters were measured. The LVEF was calculated using the biplane Simpson method in apical 2- and 4‑chamber views.11 Mitral valve disease was assessed using the European Association of Echocardiography recommendations.11 It was defined as the presence of a prosthetic mitral valve, severe mitral regurgitation, or previous surgical repair of severe mitral regurgitation.
Follow‑up and device programming
Patients were followed according to contemporary guidelines8: at the first visit 1 month after implantation and at least twice annually thereafter. The follow‑up data were retrospectively analyzed up to the final visit. The follow‑up was arbitrarily defined as “short‑term” when lasting 12 months or less, and “long‑term” when lasting longer than 12 months. The devices were programmed individually. For primary prevention, detection in the ventricular tachycardia (VT) zone was programmed typically as higher than 170 bpm, and in the ventricular fibrillation (VF) zone, as 200 bpm or higher. For secondary prevention, the VT zone was programmed as about 10 bpm below the clinical VT rate. During follow‑up, we analyzed the rate of appropriate interventions, percentage of ventricular pacing, and, in the CRT‑D group, percentage of biventricular pacing (≥98% was considered satisfactory). An ICD intervention was defined as appropriate if delivered for VT or VF; all other episodes were considered inappropriate. Only episodes with intracardiac electrograms available were considered. The episodes were analyzed by an experienced physician. Doubtful cases were resolved by 2 electrophysiologists. All‑cause mortality was also assessed. All data were obtained by reviewing the medical records, device checkups during follow‑up, or by direct telephone contact.
Statistical analysis
Continuous variables were presented as mean (SD) or median (interquartile range [IQR]), depending on the variable distribution. Categorical variables were presented as frequencies. A univariate Cox regression analysis including all available parameters was performed. Then, a multivariate Cox regression analysis was performed to assess the independent significance of all parameters with a P value of less than 0.05 in the univariate analysis. A log‑rank test was used in an intervention‑free survival analysis. For all calculations, 2‑tailed tests were used, and a P value of less than 0.05 was considered significant. Statistical analysis was performed with Statistica v. 12 (Statsoft Inc., Tulsa, Oklahoma, United States).
Results
A total of 457 patients were included in the study. The baseline characteristics of the population are shown in Table 1. Data on survival were available for 451 patients, and on appropriate interventions, for 452 patients. During the median 31‑month follow‑up (interquartile range [IQR], 17–52 months), 153 patients died (33.9%) and 140 had appropriate interventions (31.0%).
Parameter | Value |
Abbreviations: CRT‑D, cardiac resynchronization therapy defibrillator; eGFR, estimated glomerular filtration rate; IQR, interquartile range; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association | |
Age, y, mean (SD) | 66 (11) |
Female sex, n (%) | 89 (19.4) |
Weight, kg, mean (SD) | 81.88 (16.99) |
CRT‑D, n (%) | 146 (31.9) |
Primary prevention, n (%) | 374 (81.8) |
LVEF, %, median (IQR) | 29 (25–33) |
LVEF <25%, n (%) | 125 (27.4) |
NYHA class, median (IQR) | 2 (2–3) |
Ischemic etiology of heart failure, n (%) | 330 (72.2) |
Previous myocardial infarction, n (%) | 301 (65.8) |
Hypertension, n (%) | 161 (67.9) |
Diabetes, n (%) | 156 (34.1) |
Hemoglobin, mmol/l, mean (SD) | 8.37 (1.05) |
eGFR, ml/min/1.73 m2, mean (SD) | 73.3 (23.2) |
eGFR <60 ml/min/1.73 m2, n (%) | 151 (33.1) |
Severe mitral valve disease, n (%) | 50 (11.2) |
Left atrial diameter, mm, mean (SD) | 43.6 (12.3) |
Left ventricular diameter, mm, mean (SD) | 58.7 (16.4) |
Atrial fibrillation at baseline, n (%) | 187 (41.0) |
Appropriate interventions: the whole study group One‑year follow‑up data were available for 394 patients (87% of the whole group). The remaining 57 patients were lost to follow‑up: 20 patients died without an ICD/CRT‑D intervention within the first year of follow‑up, 11 patients were followed in other centers, and 32 patients were lost to follow‑up in the context of data on appropriate interventions (7%).
Appropriate ICD interventions in the first year after implantation were noted in 68 patients (17.3%). In the univariate Cox regression analysis, implantation for secondary prevention and severe mitral valve disease were significant predictors of appropriate intervention in the 1‑year follow‑up. In the multivariate Cox regression analysis, implantation for secondary prevention (hazard ratio [HR], 2.64; 95% CI, 1.60–4.37; P <0.001) and severe mitral regurgitation (HR, 2.43; 95% CI, 1.38–4.26; P = 0.002) remained independent predictors of appropriate interventions in the 1‑year follow‑up. When patients were divided according to the year of implantation (years 2011–2017), the number of appropriate interventions in the 1‑year follow‑up in subsequent years ranged from 9% in patients implanted in 2014 to 24% in patients implanted in 2011, without significant differences between the results (P = 0.44). In the univariate Cox regression analysis (including all 452 patients and all available follow‑up data), the significant predictors of appropriate interventions were implantation for secondary prevention, severe mitral valve disease, and previous myocardial infarction (Table 2). In the multivariate Cox regression analysis, all 3 parameters remained predictors of appropriate intervention (HR, 2.49; 95% CI, 1.70–3.65; P <0.001; HR, 2.17; 95% CI, 1.39–3.37; P <0.001; and HR, 1.68; 95% CI, 1.14–2.47; P = 0.009; respectively).
Parameter | Univariate analysis | ||
HR | 95% CI | P value | |
a Per 1‑year increase; b Per I‑class increase; c Per 0.1‑g/l increase; d Per 1‑mm increase; e Per 1% increase; f eGFR <60 ml/min/1.73 m2
Abbreviations: HR, hazard ratio; others, see Table 1 | |||
Agea | 1.00 | 0.99–1.02 | 0.60 |
NYHA classb | 0.88 | 0.67–1.16 | 0.36 |
Hemoglobinc | 1.02 | 0.92–1.13 | 0.70 |
Left atrial diameterd | 0.99 | 0.98–1.01 | 0.25 |
LVEFe | 1.00 | 0.98–1.02 | 0.91 |
Left ventricular end‑diastolic diameterd | 0.99 | 0.98–1.01 | 0.33 |
Sex (women vs men) | 0.88 | 0.57–1.34 | 0.54 |
Cardiac resynchronization therapy defibrillator | 0.74 | 0.51–1.08 | 0.12 |
Secondary prevention implantation | 2.26 | 3.29–1.55 | <0.001 |
Myocardial infarction | 1.66 | 1.13–2.43 | 0.001 |
Coronary artery disease | 1.44 | 0.91–2.27 | 0.12 |
Hypertension | 0.91 | 0.65–1.28 | 0.60 |
Diabetes | 1.02 | 0.72–1.45 | 0.92 |
Kidney diseasef | 1.10 | 0.76–1.60 | 0.60 |
Severe mitral valve disease | 2.00 | 1.29–3.09 | 0.002 |
Pulmonary disease | 1.04 | 0.67–1.60 | 0.86 |
Atrial fibrillation | 1.22 | 0.87–1.71 | 0.25 |
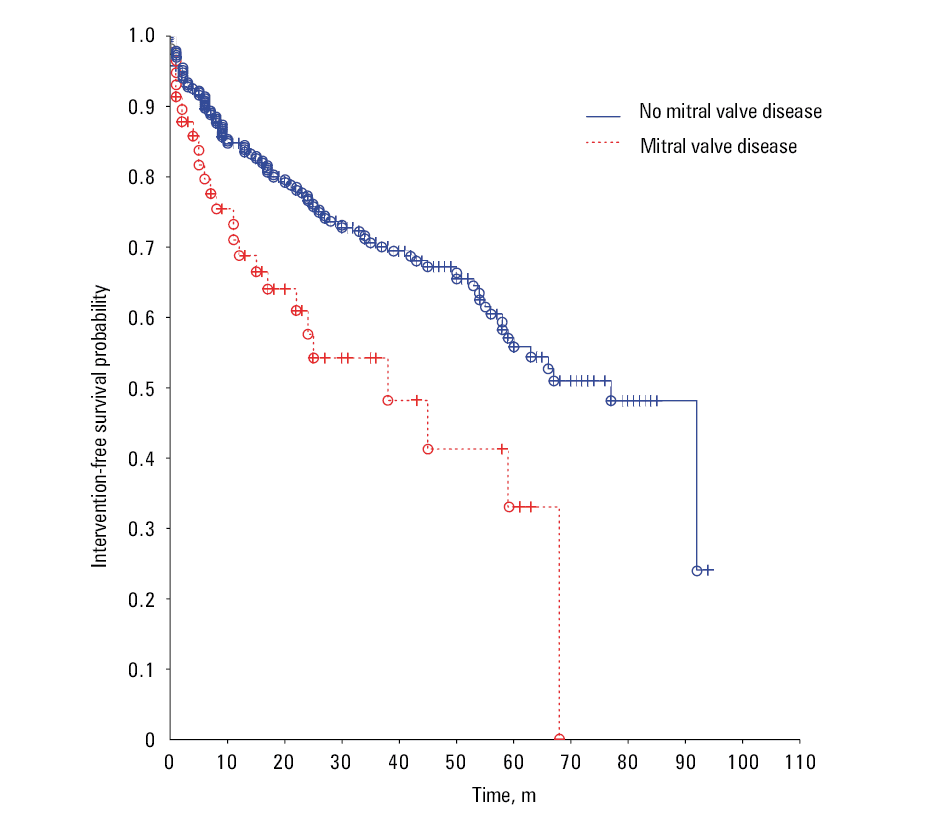
The Kaplan–Meier analysis showed an early dissociation of intervention‑free curves of patients with and without severe mitral valve disease (Figure 1). Appropriate interventions within the first year of follow‑up were noted in 4 of the 12 patients with a prosthetic mitral valve and 1 of the 4 patients after surgical repair of severe mitral regurgitation. On the other hand, none of the 8 patients with significant aortic valve disease or a prosthetic aortic valve underwent appropriate interventions within the first year of follow‑up.
Appropriate interventions: the primary‑prevention group
A total of 374 patients were implanted with an ICD or CRT‑D for primary prevention; 322 patients (86%) completed the 1‑year follow‑up. During the first year after implantation, 47 patients (14.6%) underwent appropriate interventions, as compared with 21 of the 70 patients (30%) in the secondary‑prevention group (P = 0.003). In the univariate Cox regression analysis, resynchronization therapy (protective effect) and severe mitral valve disease were significant predictors of appropriate interventions in the 1‑year follow‑up. In the multivariate Cox regression analysis, both parameters remained independently associated with appropriate interventions in the 1‑year follow‑up (HR, 0.36; 95% CI, 0.17–0.75; P = 0.006 and HR, 3.04; 95% CI, 1.60–5.80; P <0.001; respectively).
In the univariate Cox regression analysis including all patients in primary prevention and all available follow‑up data, significant predictors of appropriate interventions were similar to those for the 1‑year analysis and included resynchronization therapy, severe mitral valve disease, and previous myocardial infarction (Table 3). In the multivariate Cox regression analysis, only resynchronization therapy and severe mitral valve disease remained predictors of appropriate intervention (HR, 0.59; 95% CI, 0.37–0.93; P = 0.03 and HR, 2.42; 95% CI, 1.48–3.98; P <0.001; respectively).
Parameter | Univariate analysis | ||
HR | 95% CI | P value | |
a Per 1‑year increase; b Per I‑class increase; c Per 0.1‑g/l increase; d Per 1‑mm increase; e Per 1% increase; f eGFR <60 ml/min/1.73 m2
Abbreviations: see Tables 1and 2 | |||
Agea | 1.00 | 0.98–1.02 | 0.85 |
NYHA classb | 0.93 | 0.66–1.31 | 0.67 |
Hemoglobinc | 1.06 | 0.93–1.19 | 0.39 |
Left atrial diameterd | 0.99 | 0.98–1.01 | 0.49 |
LVEFe | 0.99 | 0.96–1.02 | 0.38 |
Left ventricular end‑diastolic diameterd | 1.00 | 0.99–1.01 | 0.78 |
Sex (women vs men) | 0.93 | 0.57–1.53 | 0.78 |
CRT‑D | 0.61 | 0.39–0.95 | 0.03 |
Myocardial infarction | 1.58 | 1.02–2.47 | 0.04 |
Coronary artery disease | 1.51 | 0.87–2.61 | 0.14 |
Hypertension | 0.87 | 0.58–1.30 | 0.50 |
Diabetes | 1.17 | 0.79–1.75 | 0.43 |
Kidney diseasef | 0.83 | 0.54–1.28 | 0.41 |
Severe mitral valve disease | 2.24 | 1.38–3.64 | 0.001 |
Pulmonary disease | 1.06 | 0.64–1.75 | 0.82 |
Atrial fibrillation | 1.23 | 0.83–1.82 | 0.30 |
Mortality
The univariate Cox regression analysis including all patients and all available follow‑up data revealed numerous significant predictors of mortality (Table 4). In the multivariate Cox regression analysis, 3 protective factors remained significant independent predictors of mortality: higher body mass index (BMI), hemoglobin concentrations, and LVEF. Two risk factors were independent predictors of mortality: diabetes and increased left atrial anteroposterior diameter (Table 4).
Parameter | Univariate analysis | Multivariate analysis | ||||
HR | 95% CI | P value | HR | 95% CI | P value | |
a Per 1‑year increase; b Per 0.1‑kg/m2 increase; c Per 1% increase; d Per I‑class increase; e Per 0.1‑g/l increase; f Per 1‑mm increase; g eGFR <60 ml/min/1.73 m2
Abbreviations: BMI, body mass index; others, see Tables 1, 2, and 3 | ||||||
Agea | 1.03 | 1.01–1.04 | <0.001 | 1.01 | 0.99–1.03 | 0.48 |
BMIb | 0.95 | 0.92–0.99 | 0.007 | 0.94 | 0.90–0.98 | 0.004 |
LVEFc | 0.95 | 0.93–0.97 | <0.001 | 0.97 | 0.94–0.99 | 0.01 |
NYHA classd | 1.61 | 1.23–2.10 | <0.001 | 1.38 | 0.99–1.92 | 0.06 |
Hemoglobine | 0.83 | 0.76–0.92 | <0.001 | 0.86 | 0.77–0.97 | 0.02 |
Left atrial diameterf | 1.03 | 1.01–1.06 | 0.002 | 1.04 | 1.01–1.06 | 0.002 |
Sex (women vs men) | 1.00 | 0.67–1.50 | 0.99 | – | – | – |
CRT‑D | 0.81 | 0.56–1.17 | 0.27 | – | – | – |
Myocardial infarction | 1.11 | 0.79–1.56 | 0.56 | – | – | – |
Hypertension | 0.91 | 0.66–1.27 | 0.59 | – | – | – |
Diabetes | 1.59 | 1.15–2.20 | 0.005 | 1.48 | 1.02–2.16 | 0.04 |
Kidney diseaseg | 2.08 | 1.50–2.87 | <0.001 | 1.45 | 0.95–2.22 | 0.08 |
Severe mitral valve disease | 1.85 | 1.22–2.81 | 0.004 | 1.20 | 0.73–1.97 | 0.47 |
Pulmonary disease | 1.57 | 1.09–2.28 | 0.02 | 1.31 | 0.86–2.00 | 0.22 |
Discussion
We aimed to identify clinical factors predicting appropriate ICD interventions in an unselected real‑life cohort of patients, especially in those who underwent implantation for primary prevention. Wa also attempted to identify clinical predictors of mortality in this cohort.
In the primary‑prevention group, resynchronization therapy and severe mitral valve disease (risk factor) were significant predictors of appropriate intervention. The results were similar for the short‑term (1‑year) and long‑term follow‑up. In the whole patient cohort, implantation for secondary prevention and severe mitral valve disease were significant predictors of ICD interventions in the short- and long‑term follow‑up. In the long‑term follow‑up, previous myocardial infarction was also a predictor of ICD interventions.
Surprisingly, predictors of mortality were completely different: BMI, hemoglobin concentration, LVEF, diabetes, and left atrial diameter. Our results support previous observations that prevention of sudden cardiac death may not necessarily reduce all‑cause mortality and does not solve all problems in patients with heart failure.12 All‑cause mortality is strongly affected by comorbidities and natural course of heart failure.
The impact of resynchronization therapy on the prevalence of ventricular arrhythmia has been postulated previously and confirmed in subsequent studies.13,14 In our study, resynchronization therapy was associated with a lower rate of appropriate interventions. The ICD implantation for secondary prevention was previously described in the literature as a risk factor for arrhythmic episodes, which is in line with our findings.7,15
The most interesting observation of our study is that severe mitral valve disease (major mitral regurgitation) was associated with a higher rate of appropriate ICD intervention. The mechanism of this association is not well understood, and literature data are scarce. Patients with severe mitral regurgitation and heart failure are characterized by high morbidity and mortality rates.16 In CARE‑HF (Cardiac Resynchronization in Heart Failure Study), a higher degree of mitral regurgitation 3 months after enrollment was a predictor of worse outcome, independent of CRT‑D implantation.17 Likewise, in an analysis of 76 patients after cardiac resynchronization therapy, mitral regurgitation at baseline did not predict a poorer outcome, but its persistence after CRT‑D implantation was associated with a greater incidence of tachyarrhythmia and worse clinical evolution.18
The impact of comorbidities on the mortality of patients with heart failure is well established. Numerous studies have reported that patients with diabetes were at higher risk of mortality, which was confirmed by our research.19 Another well‑known risk factor for mortality in this population is anemia.20 Similarly, in our study, higher hemoglobin concentrations had a positive effect on survival. The same association was observed for higher LVEF, which is in line with previous reports.21
Obesity is associated with shorter life expectancy, but, notably, obese patients with heart failure have a better prognosis—this phenomenon is known as the “obesity paradox.”22 In our study, patients with higher BMI had a reduced mortality risk.
Several studies have shown a negative influence of atrial volume and atrial diameter on mortality in patients with heart failure. Current studies evaluate both right and left atrial size and volume,23,24 but in our study, only standard measurements were available, so we calculated the left ventricular and left atrial diameters. We observed that left atrial enlargement was associated with a poorer outcome.
Strengths and limitations
Our study group was well characterized and quite homogenous, and the follow‑up was long and thorough. We evaluated a large number of parameters that are not commonly assessed in large multicenter trials and registries. However, the study also has some limitations. First, this was a retrospective, single‑center analysis. Second, the impact of medication use on the incidence of arrhythmias and mortality was not analyzed, but during follow‑up, efforts were made to treat patients according to current guidelines. Finally, ICD interventions, at least in part, depended on specific ICD programming, and arrhythmia detection algorithms vary between different ICD manufacturers. The programming guidelines changed during the follow‑up as a result of the MADIT‑RIT trial (Multicenter Automatic Defibrillator Implantation Trial – Reduce Inappropriate Therapy),25 so the programmed parameters in patients implanted in 2016 and 2017 varied from those in patients implanted earlier.
Conclusions
Implantation of ICD or CRT‑D for secondary prevention was the most potent predictor of appropriate ICD intervention. Among the numerous other clinical factors, resynchronization therapy (protective effect) and severe mitral valve disease (risk factor) had a significant impact on the rate of appropriate ICD therapy. Higher BMI, hemoglobin levels, and LVEF had a protective effect on survival, while diabetes and increased left atrial diameter were associated with mortality risk in the long‑term follow‑up. These findings may help identify a population at the highest risk of an arrhythmic event or death and to provide them with more tailored care.
- Køber L, Thune JJ, Nielsen JC, et al. DANISH Investigators. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016; 375: 1221‑1230.
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002; 346: 877‑883.
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter‑defibrillator for congestive heart failure. N Engl J Med. 2005; 352: 225‑237.
- Bristow MR, Saxon LA, Boehmer J, et al. Cardiac‑resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004; 350: 2140‑2150.
- Gracieux J, Sanders GD, Pokorney SD, et al. Incidence and predictors of appropriate therapies delivered by the implantable cardioverter defibrillator in patients with ischemic cardiomyopathy: a systematic review. Int J Cardiol. 2014; 177: 990‑994.
ARTICLE INFORMATION