Simultaneous cardiac free-wall rupture and ventricular septal rupture following acute myocardial infarction treated with emergency balloon inflation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Simultaneous cardiac free-wall rupture and ventricular septal rupture following acute myocardial infarction treated with emergency balloon inflation
Before the era of fibrinolytic reperfusion, free‑wall rupture (FWR) complicated 1% to 6% of ST‑segment elevation myocardial infarction (STEMI) cases, and ventricular septal rupture (VSR), 1% to 3%. With the introduction of primary percutaneous coronary intervention (PCI), the reported incidence of VSR has dropped and ranges from 0.2% to 0.5%. However, there is no evidence on whether primary PCI reduces the risk of FWR.1-4 We present our unique treatment strategy in a patient with simultaneous FWR and VSR following acute STEMI.
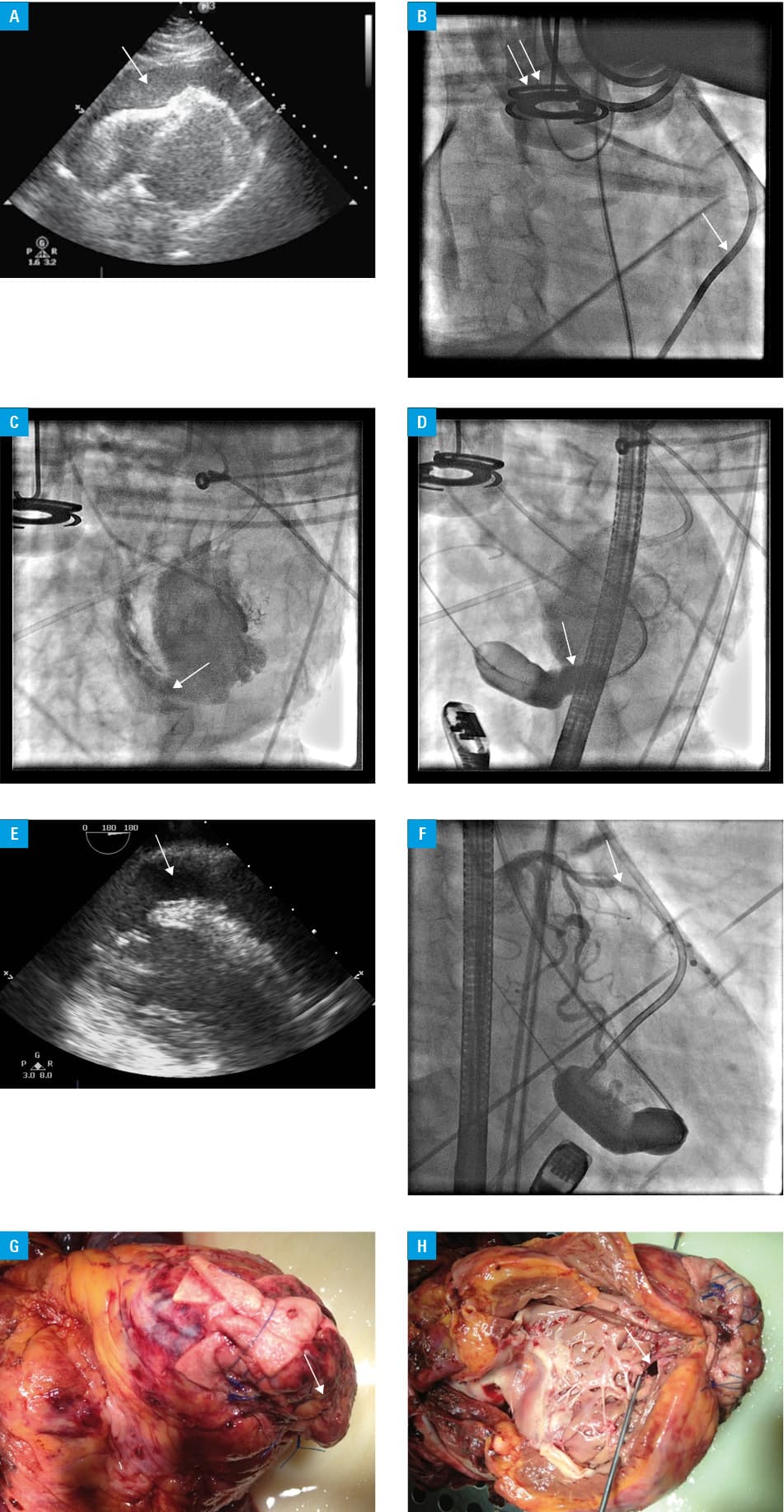
A 66‑year‑old woman was admitted within 2 hours of the onset of chest pain at rest with anterior‑wall STEMI. Physical examination on admission did not reveal any signs of heart failure. Baseline troponin T levels were 0.439 ng/ml (upper limit of normal, 0.014 ng/ml). Immediately after the examination, she experienced a cardiac arrest with pulseless electrical activity (PEA). A resuscitation procedure using the Lucas 2 system (Jolife, Lund, Sweden) was promptly initiated. Because of the PEA and the suspicion of cardiac tamponade, urgent transthoracic echocardiography was performed, which showed a large amount of pericardial effusion (Figure 1A). During pericardiocentesis with subsequent drainage, 200 ml of blood was aspirated (Figure 1B). Despite successful pericardiocentesis, the patient remained in shock with a systolic blood pressure of only 80 mm Hg on a high dose of epinephrine and norepinephrine. Therefore, she was transferred to the catheterization laboratory where a VSR near the left ventricular apex was found (Figure 1C). Under transesophageal echocardiography guidance, a balloon catheter (size, 20 × 40 mm) was introduced over the wire from the left to right ventricle and subsequently inflated in the septum. As a result, the VSR was closed and the left‑to‑right cardiac shunt was stopped (Figure 1D and 1E). Hemodynamic stability was achieved on a low dose of epinephrine and the pericardial hemorrhage was stopped. Afterwards, an occlusion in the mid part of the left anterior descending artery was revealed (Figure 1F). The patient, with the balloon inflated in the VSR, was transferred to the operating room, where the surgeons sutured both the VSR and FWR (Figure 1G). Two days after the surgery, the patient was conscious and was recovering without catecholamine infusion. Unfortunately, she died 2 days later. Autopsy revealed recanalization of the VSR (Figure 1H).
Cardiac arrest with PEA in a patient with STEMI is an extremely rare clinical situation,5 in which FWR should always be suspected. Therefore, to confirm any clinical suspicion, transthoracic echocardiography is mandatory, followed by pericardiocentesis. When the removal of pericardial effusion does not result in hemodynamic stability, other causes of cardiogenic shock should be considered. In our patient, we found VSR near the left ventricular apex that was not suitable for percutaneous closure. Therefore, we performed a transcatheter balloon inflation in the ruptured septum.
To the best of our knowledge, this is the first description of an emergency procedure with temporary balloon inflation in the septum that fully closed the VSR, rapidly improved the patient’s hemodynamics, and made it possible to perform a cardiac surgery.
- Jones BM, Kapadia SR, Smedira NG, et al. Ventricular septal rupture complicating acute myocardial infarction: a contemporary review. Eur Heart J. 2014; 35: 2060‑2068. | Crossref
- Xue X, Kan J, Zhang JJ, et al. Comparison in prevalence, predictors, and clinical outcome of VSR versus FWR after acute myocardial infarction: the prospective, multicenter registry MOODY trial‑heart rupture analysis. Cardiovasc Revasc Med. 2019 Jan 23. . | Crossref
- Piątek J, Kędziora A, Ulańska‑Poutanen J, et al. Early onset and persistent progression of coronary artery disease of unknown etiology in a 30‑year‑old man. Pol Arch Intern Med. 2017; 127: 698‑700.
- Karwowski J, Gierlotka M, Gąsior M, et al. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Pol Arch Intern Med. 2017; 127: 401‑411. | Crossref
- Soar J, Donnino MW, Maconochie I, et al. 2018 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: summary. Circulation. 2018; 138: e714‑e730.
ARTICLE INFORMATION