Determinants of long-term outcome in patients after percutaneous stent-assisted intervention for renal artery steno-occlusive atherosclerotic disease
Key words: blood pressure, cardiovascular adverse events, percutaneous transluminal angioplasty, renal artery stenosis, renal function



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Determinants of long-term outcome in patients after percutaneous stent-assisted intervention for renal artery steno-occlusive atherosclerotic disease
Introduction: The effect of stent‑assisted percutaneous transluminal angioplasty (PTA) for renal artery stenosis (RAS) on systolic (SBP) and diastolic blood pressure (DBP) as well as renal function, in comparison with medical therapy, is still debatable. Data on determinants of cardiovascular (CV) outcome after PTA are lacking.
Objectives: We aimed to identify determinants of major cardiac and cerebral events (MACCEs) following PTA for RAS.
Patients and methods: A total of 248 PTAs for RAS were performed in 211 patients with difficult‑to‑treat hypertension and/or progressive renal impairment. The primary outcomes were procedural success, in‑hospital complications, renal function (estimated glomerular filtration rate [eGFR]), change in SBP or DBP, and an incidence of MACCEs during a median of 47 months (interquartile range [IQR], 18–78 months).
Results: Procedural success and complication rates were 99.2% and 4.7%, respectively. We observed significant differences in SBP, DBP, and eGFR at 12 months as compared with baseline. A total of 63 MACCEs (30.6%) were noted in 206 patients with available follow‑up data. The receiver operating characteristic curve analysis indicated the following best cutoff values for the risk of CV death: an increase in eGFR by at least 11 ml/min/1.73 m2 and a decrease in SBP and DBP by at least 20 mm Hg and 5 mm Hg, respectively. At 12‑month follow‑up, an increase in eGFR of at least 11 ml/min/1.73 m2 was independently associated with a reduced risk of death (hazard ratio [HR], 0.42; 95% CI, 0.19–0.90; P = 0.02) and MACCEs (HR, 0.54; 95% CI, 0.32–0.93; P = 0.03), while a decrease of DBP by 5 mm Hg or higher, with a reduced risk of stroke (HR, 0.1; 95% CI, 0.02–0.39; P = 0.001).
Conclusions: This study confirms the efficacy and safety of PTA as well as its significant effect on changes in blood pressure and eGFR values. Patients with an increase in eGFR of at least 11 ml/min/1.73 m2 have a significant risk reduction of MACCEs and CV death, while those with a decrease in DBP of at least 5 mm Hg, of stroke.
What's new?
After failure of the CORAL and ASTRAL trials, stent‑assisted percutaneous transluminal angioplasty (PTA) for renal artery stenosis (RAS) is experiencing a renaissance. The novelty of our study is the identification that an increase in estimated glomerular filtration rate (eGFR; calculated by the Modification of Diet in Renal Disease formula [MDRD]) of at least 11 ml/min/1.73 m2 and a reduction in diastolic blood pressure of at least 5 mm Hg after PTA of RAS are associated with better prognosis with respect to the incidence of major cardiac and cerebral events (MACCEs). Thus, we were able to identify a subgroup of patients with atherosclerotic RAS who obtain a significant clinical benefit from PTA in terms of a reduced risk of MACCEs and cardiovascular death. We chose the MDRD formula because it was shown to provide a less biased estimate together with the highest accuracy in patients with reduced renal function.
Introduction
Stent‑assisted percutaneous transluminal angioplasty (PTA) of symptomatic atherosclerotic renal artery stenosis (RAS) still remains a controversial issue, which was reflected by a weak level of evidence in the European Society of Cardiology (ESC) and American Heart Association/American College of Cardiology guidelines.1,2 On the one hand, a series of observational studies indicated a significant decrease in blood pressure (BP) and/or creatinine levels.3-7 Furthermore, a number of studies reported the effect of PTA for RAS on the reduction of cardiovascular (CV) risk as well as symptoms of heart failure and/or angina,8-11 although the effect was not as encouraging as in patients with fibromuscular dysplasia.12 In contrast, randomized controlled trials (RCTs) largely do not support the clinical benefit of PTA plus medical therapy in comparison with medical therapy alone.13-20 Among the 8 available RCTs, the CORAL study (Cardiovascular Outcomes in Renal Atherosclerotic Lesions) confirmed the advantage of PTA plus medical therapy over medical therapy alone in terms of improving BP control, while these findings were confirmed only by 2 of the numerous nonrandomized studies.13-22
Importantly, BP control with medical therapy does not prevent progression of RAS. Between 36% and 71% of patients were reported to experience progression during 5 years,23 while renal artery occlusion within 1 year was observed in 16% of medically treated patients.24
Renal artery stenosis is associated with poor long‑term prognosis, increasing the risk of all‑cause mortality and CV events.24,25 In the 1960s, Wollenweber et al26 reported the estimated risk of adverse CV events in patients with RAS of 47% during a 6‑year follow‑up, and it remained associated with the severity of stenosis and bilateral RAS. An annual all‑cause mortality rate was estimated at 12.7%, increasing to 18% in bilateral RAS.27
More recently, an association between the use of statins in patients with atherosclerotic RAS and a reduced risk of RAS progression (relative risk, 0.28; 95% CI, 0.10–0.77), lower rate of renal insufficiency progression, lower overall mortality, and lower incidence of adverse outcomes was reported.28,29 It was suggested that all patients with hypertension and hemodynamically significant RAS, with or without mild to moderate impairment of renal function, should be considered for renal PTA.30,31 In a study by Catena et al,30 stenting of hemodynamically significant atherosclerotic RAS was associated with a reduced BP, preserved renal function in a substantial proportion of patients, and improved left ventricular structure and function. Patients with atheromatous stenosis in a single functioning kidney, and those who present with signs of sodium and water retention, are likely to benefit most.31
However, irrespective of the impact of PTA for RAS on BP and renal function, there is vague evidence on its influence on CV morbidity and mortality. Therefore, the aim of the present study was to evaluate the safety and efficacy of PTA for RAS in terms of procedural success, in‑hospital complications, renal function, and changes in systolic (SBP) or diastolic BP (DBP). We investigated whether a change in BP values and renal function following PTA for RAS, as well as other potential factors, can be used as determinants of adverse CV events during long‑term follow‑up.
Patients and methods
In this retrospective study, we assessed the immediate and long‑term outcome of 248 PTAs for symptomatic RAS performed in 211 consecutive patients with difficult‑to‑treat arterial hypertension or known progressive renal impairment (or both) between November 2003 and September 2017.
The inclusion criteria were de novo unilateral or bilateral atherosclerotic RAS of at least 60% with all or any of the following: accelerated hypertension (SBP >160 mm Hg or hypertensive crisis despite the use of 3 or more BP‑lowering drugs, including at least 1 diuretic), drug‑resistant hypertension (SBP of >140 mm Hg and/or DBP of 90 mm Hg, despite the use of at least 3 BP‑lowering drugs, including at least 1 diuretic), or hypertensive crisis (defined as severely elevated BP, ie, SBP >220 mm Hg or DBP >120 mm Hg, with no evidence of target organ damage). We also included patients with acute or progressive renal failure during the previous 3 to 6 months (a recent deterioration of renal function defined as a significant decrease of estimated glomerular filtration rate [eGFR] ≥30% or an increase of serum creatinine levels >0.5 mg/dl detected during 3–6 months before the decision on PTA) and/or an episode of acute renal failure associated with angiotensin‑converting enzyme inhibitor (ACEI) treatment. The other inclusion criteria were flash pulmonary edema, congestive heart failure, and severe angina or acute coronary syndrome that could not be explained by coronary artery status.
The exclusion criteria were as follows: well‑controlled BP on antihypertensive drugs, renal atrophy (kidney length <7 cm in women and <8 cm in men), and lack of patient consent.
The use of ACEIs, sartans, β-blockers, calcium channel blockers, diuretics, α-blockers, and central nervous system blockers were reported in 58%, 8%, 78%, 60%, 100%, 14%, and 16% of patients on admission, prior to the procedure. As per the study policy, we did not change initial medications until PTA for RAS was performed to avoid bias related to renal function and BP value modification due to additional medical regimens.
All patients gave their informed consent before enrollment in accordance with the requirements of the local ethics committee (approval no., KBET/392/B/2003). The study was performed in line with the principles of the Declaration of Helsinki.
Cardiovascular risk factors
The prevalence of CV risk factors was assessed. Diabetes mellitus was defined as treated or newly diagnosed diabetes (glucose >11 mmol/l [200 mg/dl] in an oral glucose tolerance test). Hyperlipidemia was defined as treated or newly diagnosed hyperlipidemia (total cholesterol >4.9 mmol/l [190 mg/dl] and/or low‑density lipoprotein cholesterol [LDL‑C]) >3.0 mmol/l [115 mg/dl] and/or high‑density lipoprotein cholesterol [HDL‑C] <1.0 mmol/l [40 mg/dl] for men and <1.2 mmol/l [46 mg/dl] for women and/or triglycerides >1.7 mmol/l [150 mg/dl]). Smoking was defined as current active smoking or active smoking in the past 5 years.
Laboratory tests and renal function assessment Blood samples were collected on admission, prior to any intervention, and immediately after the signed informed consent was obtained from patients. The following biochemical parameters were analyzed: serum creatinine, total cholesterol, HDL‑C, LDL‑C, high‑sensitivity C‑reactive protein, and triglycerides. The eGFR was assessed using the Modification of Diet in Renal Disease (MDRD) formula, according to the following equation: MDRD = 175 × creatinine [mg/dl] − 1.154 × age [years] − 0.203 × 0.742 [if female]. Renal function assessment including the measurement of serum creatinine and eGFR levels was repeated at 3 to 6 and 12 months, and during the final follow‑up visit.
Assessment of atherosclerosis in major arterial territories
At baseline, all patients were examined for concurrent steno‑occlusive atherosclerotic disease in other major arteries. Coronary artery disease, carotid artery stenosis, and peripheral artery disease (PAD) were diagnosed on the basis of a history of revascularization or the presence of substantial atherosclerotic lesions (defined as at least 50% vascular lumen reduction in the corresponding territory as assessed by duplex ultrasonography, computed tomography [CT] angiography, or invasive angiography).
Renal artery stenosis was initially diagnosed with duplex ultrasonography based on the peak‑systolic aortic and renal artery velocities and intra‑renal flow parameters. The RAS was confirmed with either CT angiography or directly during invasive angiography preceding the PTA procedure. In some patients, the severity of stenosis was established using translesional resting and hyperemic gradients.
Additionally, the ankle‑brachial index was routinely evaluated in all patients as a screening tool for PAD, with a cutoff value of less than 0.9. The diagnosis of PAD was confirmed with Doppler ultrasound in all cases with an ankle‑brachial index of less than 0.9. Stenosis of the carotid or lower extremity arteries assessed as significant by Doppler ultrasound based on the peak systolic and end‑diastolic velocities was verified by angiography or CT angiography.
Coronary and peripheral angiography was performed from radial or femoral vascular access using the Coroscop system (Siemens AG, Munich, Germany) equipped with the Quantcor v. 4.0 quantitative analysis software (Siemens, Erlangen, Germany). Angiography was performed in at least 2 orthogonal projections that best visualized the lesion.
Revascularization procedure for renal artery stenosis
Eligibility criteria were determined on the basis of the current guidelines for percutaneous revascularization of the RAS.32-34 In brief, the decision to perform PTA for RAS was reached based on clinical assessment, renal function evaluation, presence of drug‑resistant or malignant hypertension, and the severity of RAS exceeding at least 60%.
Renal angiography was performed using the femoral or radial/brachial approach. Aspirin at a loading dose of 300 mg, followed by 75 mg/d, was given indefinitely, and clopidogrel at a loading dose of 300 mg, followed by 75 mg/d, for 3 to 6 months. During the procedure, unfractionated heparin was administered according to patient weight and activated clotting time. Other medications, such as analgesics and β-blockers, were administered according to clinical indications. During the procedure, patients were routinely given 1.5 to 2.0 l of intravenous fluids to prevent contrast‑induced nephropathy.
The significance of RAS was determined by quantitative angiography (Coroscop, Siemens), and the Quantcor QCA V4.0 software for quantitative analysis (Siemens). The range of 50% to 69% diameter stenosis was considered as borderline, and additional invasive criteria were considered to confirm the significance of stenosis (resting mean translational pressure gradient >10 mm Hg or systolic hyperemic pressure gradient >20 mm Hg or renal fractional flow reserve ≤0.8).
During revascularization, a target vessel was routinely stented. Predilation and the choice of stent depended on the clinical circumstances and were at the discretion of an operator. The procedural success was defined as residual diameter stenosis of less than 30%. Procedural failure was considered if residual stenosis was 30% or greater according to angiographic measurement, including lesions that could not be dilated or crossed.
Follow‑up
During the 12‑month follow‑up, repeated measurements of BP (at least 3 measurements after 5‑minute rest) and renal function parameters were obtained at an outpatient clinic in the period between 3 and 6 months, and then at 12 months. If a patient died during the 12‑month follow‑up, the parameters from the last follow‑up visit were included in statistical analysis.
Successful treatment of hypertension was defined as BP values below 140/90 mm Hg in a patient taken off hypertensive medications. During the mean (SD) follow‑up of 53 (41) months (range, 1–163 months), the incidence of major cardiac and cerebral events (MACCEs), including myocardial infarction (MI), ischemic stroke (IS), and CV death, were recorded. The median follow‑up period was 47 months (interquartile range [IQR], 18–78 months).
The diagnosis of MI was based on the definitions proposed by the ESC, while IS was diagnosed by a neurologist to ensure validity of the diagnosis. Cardiovascular death was defined as fatal IS, fatal MI, or other CV death (ie, any sudden or unexpected death unless proven as noncardiovascular on autopsy).
Data on MACCEs were collected during the follow‑up visits. The final visit was conducted by telephone contact with a patient or an appointed family member. For patients lost to follow‑up (n = 4), the data on whether they were alive were obtained from a national health registry.
Statistical analysis
The t test for continuous and paired variables was used for comparison of continuous variables (both), and the χ2 test was applied to compare the proportions of categorical variables. Frequencies were compared by the χ2 test for independence.
We analyzed the effect of changes in renal function, BP parameters, and patient‑related factors on the incidence of the following endpoints: MACCEs, MI, IS, and CV death. To ensure reliable cutoff values for the change in BP and renal function parameters that could be potentially associated with the risk of CV death, receiver operating characteristic (ROC) curves were constructed. The area under the ROC curve and 95% confidence intervals (CIs) were calculated. The ROC curve analysis was followed by univariate and multivariate Cox model analyses.
To establish the factors that could affect the incidence of MACCEs, MI, IS, and CV death, the clinical, procedural, and angiographic variables were assessed by a univariate Cox hazards analysis, and in cases with a trend toward a difference (P <0.1), they were included in a multivariate stepwise Cox proportional hazards analysis. The results of the multivariate Cox analysis were expressed as hazard ratios (HRs) and 95% CIs. Statistical analyses were performed with the Statistica v. 13.0 software (StatSoft, Inc, Tulsa, Oklahoma, United States). A P value of less than 0.05 was considered significant.
Results
The main indication for the PTA procedure was drug‑resistant hypertension: 91 patients (43.1%), including 44 patients (20%) with hypertensive crisis despite administration of at least 3 antihypertensive drugs, including at least 1 diuretic. Overall, hypertensive crisis was noted in 80 patients (37.9%); pulmonary edema, in 6 (2.8%); and symptoms of severe or unstable angina or non–ST‑segment elevation myocardial infarction without significant coronary lesions, in 10 patients (4.7%). Other indications were as follows: RAS in patients with a single functioning kidney (30 patients [14.2%]), progressive or acute renal failure (18 patients [8.5%], including 4 patients (1.9%) with episodes due to ACEI use), documented RAS progression (14 patients [6.6%]), and a recent onset of arterial hypertension (2 patients [0.9%]).
Renal impairment at baseline (eGFR <60 ml/min/1.73 m2) was noted in 98 patients (46.4). Advanced renal failure (eGFR <30 ml/min/1.73 m2) was present in 28 patients (13.3%), in whom PTA was considered a potentially kidney‑saving procedure delaying the need for renal replacement therapy. Overall, in 68 patients (32.2%), more than 1 indication for RAS was noted. Detailed patient characteristics are presented in Table 1.
Parameter | Value | |
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: CABG, coronary artery bypass grafting; eGFR, estimated glomerular filtration rate; IS, ischemic stroke; MI, myocardial infarction; PCI, percutaneous coronary intervention; RAS, renal artery stenosis; TIA, transient ischemic attack | ||
Clinical characteristics | ||
Age, y | Mean (SD) | 66.5 (9.8) |
Range | 34–85 | |
Male sex | 114 (68.2) | |
Hypertension | 211 (100) | |
Diabetes mellitus | 67 (31.7) | |
Hyperlipidemia | 204 (96.7) | |
Smoking history | 98 (46.4) | |
Renal impairment (eGFR <60 ml/min/1.73 m2) | 130 (61.6) | |
Previous MI | 37 (17.5) | |
Previous PCI | 71 (33.6) | |
Previous CABG | 36 (17.1) | |
Previous IS or TIA | 26 (12.3) | |
Coronary artery disease | 146 (69.2) | |
Peripheral artery disease | 72 (34.1) | |
Carotid or vertebral artery disease | 94 (44.5) | |
Previous revascularization of extracoronary arteries | 65 (30.8) | |
Concomitant atherosclerotic occlusive lesions >50% in at least 2 major peripheral arterial territories | 100 (47.4) | |
Atherosclerotic involvement of contralateral renal artery >30% | 95 (45) | |
Indications for revascularization | ||
Progressive or acute renal failure in the last 3 months | 18 (8.5) | |
Pulmonary flash edema | 6 (2.8) | |
Hypertensive crisis | 80 (37.9) | |
Accelerated hypertension | 38 (18) | |
Drug‑resistant hypertension | 91 (42.1) | |
Severe angina pectoris despite normal coronary arteries | 10 (4.7) | |
RAS of a single functioning kidney | 30 (14.2) | |
The PTA of unilateral RAS was performed in 174 patients, and of bilateral RAS, in 37 patients. Procedural success rate was 99.2%. The mean (SD) baseline diameter stenosis was reduced from 74.9% (15.9%) to 17.7% (8.7%) after PTA (P <0.001) Detailed data are presented in Table 2.
Parameter | Value | |
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: PTA, percutaneous transluminal angioplasty; others, see Table 1 | ||
Patients treated with PTA, n | 211 | |
Lesions treated with PTA, n | 248 | |
Right renal artery disease (per procedure) | 119 (47.9) | |
Left renal artery disease (per procedure) | 129 (52.1) | |
PTA of bilateral RAS | 37 (17.5) | |
PTA of a single functioning kidney | 21 (9.9) | |
Lumen diameter stenosis before PTA, %, mean (SD) | 74.9 (15.9) | |
Lumen diameter stenosis, after PTA, %, mean (SD) | 17.7 (8.7) | |
Stent length, mm | Mean (SD) | 16.3 (4.2) |
Range | 7–38 | |
Stent diameter, mm | Mean (SD) | 5.7 (0.9) |
Range | 3–8 | |
Transfemoral access | 233 (93.9) | |
Radial access | 7 (2.8) | |
Brachial access by Sones technique | 8 (3.3) | |
Double site access (per staged successful procedures) | 4 (1.6) | |
Successful PTA ± stent (per procedure / per patient) | 246 (99.2) / 209 (99) | |
Balloon angioplasty alone | 2 (0.8) | |
Stent implantation (per procedure), n | 244 | |
Drug‑eluting stents implanted (per procedure), n | 24 (9.8) | |
Bare metal stents (per procedure), n | 220 (90.2) | |
Implanted stents (per procedure), n | 244 (98.4) | |
1 stent per lesion | 234 (95.9) | |
≥2 stents per lesion | 10 (4.1) | |
Direct stenting (per stent implantation) | 165 (67.6) | |
Simultaneous PTA in additional vascular territory (per patient) | 11 (5.2) | |
PTA of the coronary artery | 5 (2.3) | |
PTA of the lower limb artery | 6 (2.8) | |
Major in‑hospital complications (per patient) | Procedure‑related death (acute limb ischemia followed by multiple organ failure) | 1 (0.47) |
Acute occlusion of renal artery | 3 (1.42) | |
Renal infarction | 1 (0.47) | |
Access site major hematoma treated with blood transfusion | 2 (0.94) | |
Total | 6 (2.84) | |
Minor in‑hospital complications (per patient) | In‑hospital dialysis | 2 (0.94) |
Access site minor hematoma | 3 (1.42) | |
Access site pseudoaneurysm | 2 (0.94) | |
Total | 7 (3.31) | |
Postdischarge events during 30‑day follow‑up (per patient) | All‑cause mortality (pancreatitis, neoplasm) | 2 (1.42) |
Intracranial hemorrhage | 1 (0.47) | |
Ischemic stroke | 1 (0.47) | |
Myocardial infarction | 1 (0.47) | |
Peripheral embolization (blue toe syndrome) | 2 (0.94) | |
Total | 7 (3.31) | |
Although stent‑assisted PTA was preplanned as a routine approach, stent was not implanted in 4 procedures (2 cases of procedure failure due to unsuccessful lesion crossing with a guidewire; 2 cases of an optimal outcome of balloon angioplasty alone). Most of the implanted stents were bare metal stents (220 [90.2%]), while the remaining 24 stents (9.8%) were drug‑eluting stents. Direct stenting was performed in 165 procedures (67.6%), while predilation was necessary in 79 procedures (32.4%). Major periprocedural complications occurred in 6 patients (2.84%). Periprocedural death was noted in 1 patient (0.47%) due to acute limb ischemia followed by multiple organ failure. There were no cases of in‑hospital IS or MI. Other major in‑hospital complications included acute renal artery occlusion in 3 patients (successfully treated in 2 patients, while resulting in renal infarction in 1 patient), acute lower limb ischemia requiring urgent surgery in 1 patient, and bleeding requiring blood transfusion in 2 patients. Minor in‑hospital complications occurred in 7 patients (3.32%) (Table 2). Within 30 days after the procedure, postdischarge death was noted in 2 patients (0.94%) and was caused by pancreatitis and malignancy.
Follow‑up data were available in 206 patients. Overall, at 12 months, in comparison with baseline, we observed a decrease in SBP (mean [SD], 136 [19] mm Hg vs 148 [24] mm Hg; P <0.001) and DBP (76 [12] mm Hg vs 81 [14] mm Hg; P <0.001), as shown in Figure 1. Successful treatment of hypertension was noted in 4 patients (1.9%), while improvement of BP control accompanied by a reduction in the use of antihypertensive drugs, in 38 patients (18.4%). Overall, there was no difference in the mean (SD) number of antihypertensive drugs at 12‑month follow‑up in comparison with baseline: 3.30 (1.4) and 3.54 (1.4), respectively, P = 0.16.
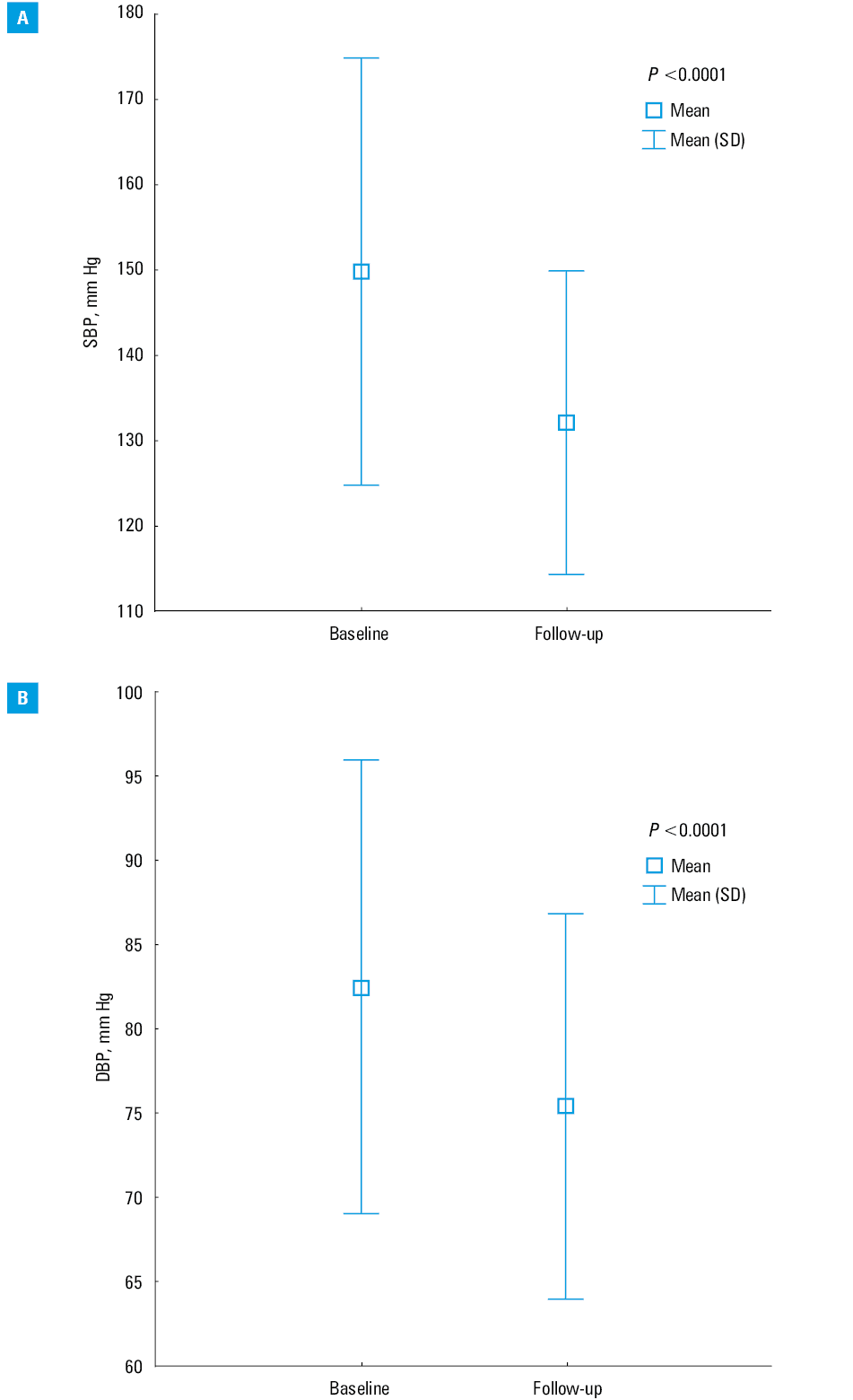
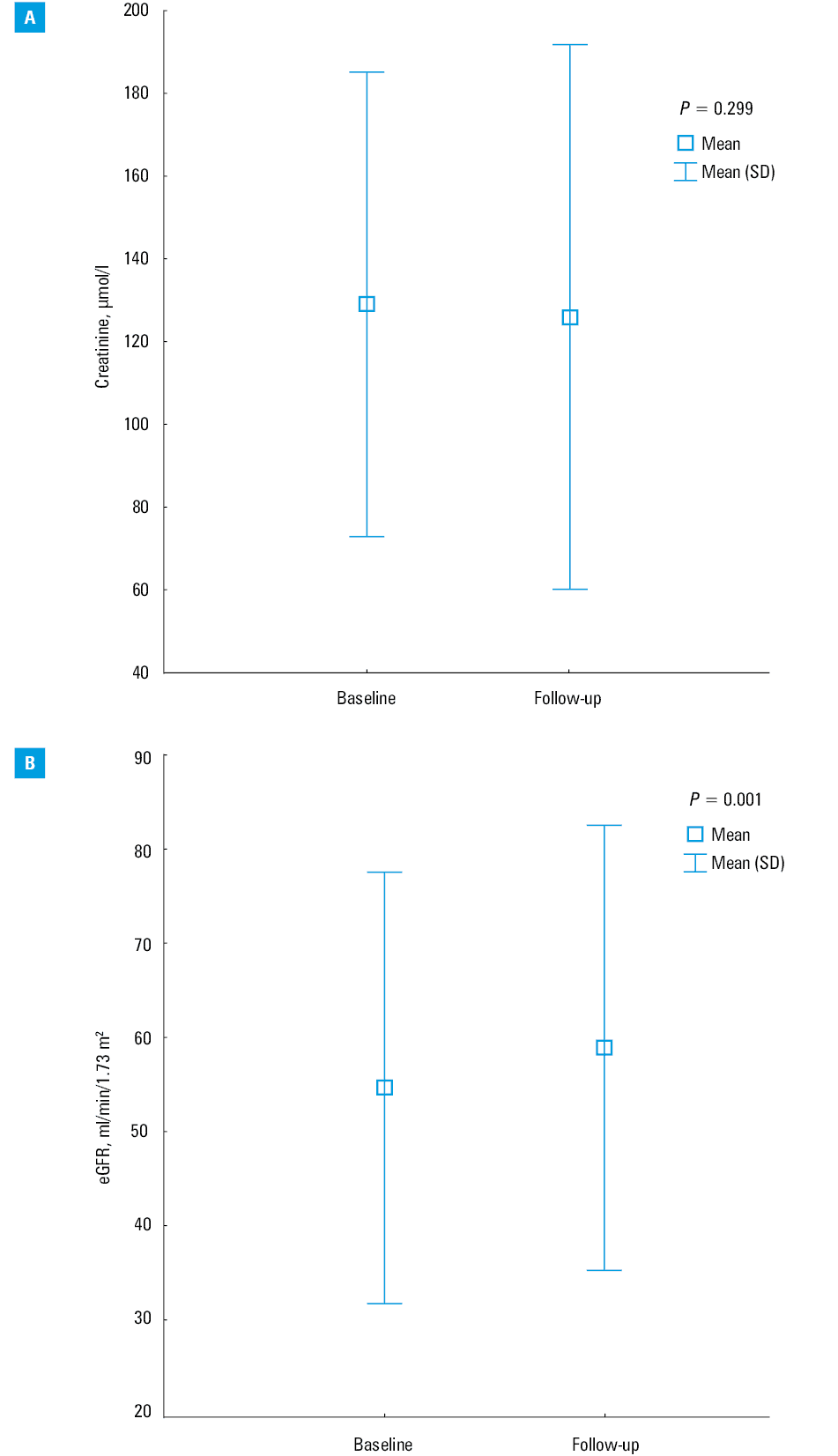
The mean (SD) eGFR value increased at 12 months from 54 (22) ml/min/1.73 m2 at baseline to 58 (23) ml/min/1.73 m2 after PTA (P = 0.001), despite no change in the mean (SD) serum creatinine level from 127 (54) μmol/l to 124 (60) μmol/l (P = 0.3) (Figure 2).
There were no differences in the Spearman correlation coefficient between eGFR and SBP as well as eGFR and DBP (r = 0.102, P = 0.17 and r = 0.084, P = 0.25, respectively). During a median follow‑up of 47 months (IQR, 18–78 months), 63 MACCEs (30.6%) were noted, including 28 CV deaths (13.6%), 23 nonfatal MIs (11.1%), and 15 nonfatal ISs (7.3%).
We used the ROC curve analysis to identify potential associations between the risk of CV death and changes in BP and renal function parameters. The best cutoff values were as follows: an increase in eGFR by at least 11 ml/min/1.73 m2, a decrease in serum creatinine levels by more than 20 μmol/l, and a reduction in SBP and DBP by at least 20 mm Hg and 5 mm Hg, respectively (Figures 3and 4).
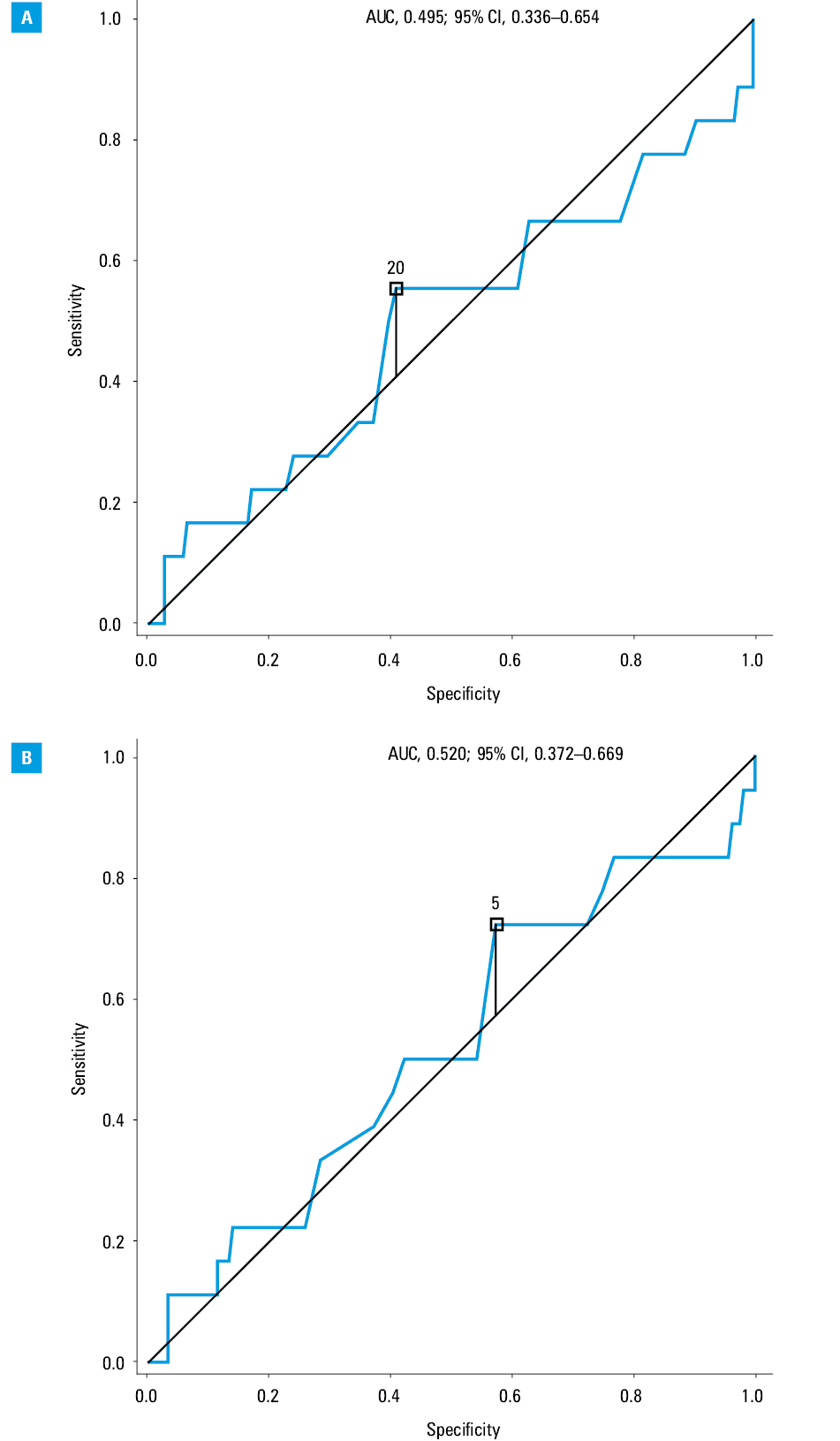
Out of the 206 patients presenting at follow‑up visits, a significant decrease in SBP (≥20 mm Hg) and/or DBP (≥5 mm Hg) was noted in 72 patients (34.9%) and 94 patients (45.6%), respectively, while an increase in eGFR by at least 11 ml/min/1.73 m2 was noted in 49 patients (23.8%), and a decrease in creatinine levels by more than 20 μmol/l, in 50 patients (24.3%).
The univariate Cox proportional hazards analysis indicated several potential clinical and angiographic parameters that could influence MACCEs (Table 3). The multivariate Cox hazards proportional model confirmed independent associations between the higher risk of MACCEs and male sex (HR, 1.81; 95% CI, 1.02–3.22; P = 0.04), multivessel coronary artery disease (HR, 2.28; 95% CI, 1.33–3.92; P = 0.002), history of hyperlipidemia (HR, 9.27; 95% CI, 1.13–5.73; P = 0.04), and concomitant atherosclerotic lesions (>30% stenosis) in contralateral renal artery (HR, 2.24; 95% CI, 1.31–3.83; P = 0.003). An increase in eGFR by at least 11 ml/min/1.73 m2 at 12‑month follow‑up was associated with a 46% reduction in the risk of MACCEs (HR, 0.54; 95% CI, 0.32–0.93; P = 0.03).
Parameter | MACCEs | CVD | MI | IS | ||||
HR (CI 95%) | P value | HR (CI 95%) | P value | HR (CI 95%) | P value | HR (CI 95%) | P value | |
Demographic parameters | ||||||||
Age, y | 1.01 (0.97–1.03) | 0.92 | 0.98 (0.95–1.02) | 0.38 | 0.99 (0.96–1.03) | 0.94 | 1.01 (0.96–1.06) | 0.64 |
Male sex | 2.02 (1.15–3.54) | 0.01 | 2.36 (1.01–5.55) | 0.05 | 4.71 (1.94–11.5) | 0.001 | 0.64 (0.25–1.63) | 0.35 |
Diabetes mellitus | 0.97 (0.56–1.68) | 0.92 | 0.85 (0.37–1.94) | 0.70 | 0.96 (0.47–1.98) | 0.92 | 1.37 (0.53–3.54) | 0.51 |
Hyperlipidemia | 4.98 (0.66–37.4) | 0.12 | 1.40 (0.90–10.3) | 0.74 | 3.39 (0.43–26.6) | 0.25 | 1.31 (0.00–1.00) | 0.99 |
Smoking | 1.21 (0.72–2.03) | 0.47 | 1.79 (0.84–3.82) | 0.13 | 0.85 (0.43–1.69) | 0.65 | 1.50 (0.59–3.80) | 0.39 |
Previous MI | 1.34 (0.67–2.66) | 0.41 | 1.68 (0.7–4.1) | 0.26 | 1.47 (0.60–3.61) | 0.40 | 1.18 (0.34–4.11) | 0.79 |
Previous IS | 1.53 (0.72–3.26) | 0.27 | 0.70 (0.2–2.9) | 0.63 | 0.59 (0.14–2.43) | 0.45 | 4.62 (1.72–12.4) | 0.002 |
Multivessel CAD | 1.21 (0.48–3.08) | 0.68 | 2.71 (1.25–5.89) | 0.01 | 4.38 (2.08–9.20) | 0.001 | 1.21 (0.47–3.08) | 0.68 |
LVEF, % | 0.99 (0.96–1.02) | 0.59 | 0.96 (0.93–1.00) | 0.06 | 0.98 (0.94–1.01) | 0.22 | 1.00 (0.96–1.06) | 0.81 |
Previous PCI | 1.20 (0.70–2.04) | 0.49 | 0.78 (0.35–1.75) | 0.55 | 1.29 (0.65–2.56) | 0.47 | 0.85 (0.32–2.28) | 0.75 |
Previous CABG | 1.76 (0.96–3.22) | 0.07 | 2.53 (1.14–5.63) | 0.02 | 3.62 (1.79–7.32) | <0.001 | 0.67 (0.16–2.91) | 0.59 |
Stenoses in additional 2 peripheral arterial territories | 2.54 (0.95–6.78) | 0.06 | 1.88 (0.88–4.01) | 0.10 | 2.13 (1.06–4.25) | 0.03 | 2.54 (0.95–6.78) | 0.06 |
Previous PTA | 1.07 (0.59–1.96) | 0.82 | 0.38 (0.11–1.27) | 0.11 | 1.22 (0.67–2.62) | 0.61 | 1.25 (0.45–3.52) | 0.67 |
SBP at baseline, mm Hg | 1.01 (0.99–1.02) | 0.10 | 1.01 (0.99–1.02) | 0.22 | 1.00 (0.99–1.02) | 0.70 | 1.01 (0.99–1.03) | 0.08 |
DBP at baseline, mm Hg | 0.99 (0.97–1.01) | 0.65 | 1.00 (0.97–1.04) | 0.79 | 0.99 (0.97–1.02) | 0.56 | 1.00 (0.97–1.04) | 0.84 |
Creatinine at baseline, µmol/l | 1.01 (1.00–1.01) | <0.001 | 1.01 (1.00–1.01) | <0.001 | 1.01 (1.00–1.01) | 0.001 | 1.00 (0.10–1.01) | 0.06 |
eGFR at baseline, ml/min/1.73 m2 | 0.98 (0.97–0.99) | 0.004 | 0.98 (0.96–0.99) | 0.03 | 0.98 (0.97–1.00) | 0.08 | 0.97 (0.95–0.99) | 0.02 |
Procedural data | ||||||||
Contralateral RAS ≥30% | 2.16 (1.28–3.66) | 0.004 | 3.54 (1.56–8.06) | 0.002 | 1.10 (1.01–3.96) | 0.05 | 2.70 (1.01–7.22) | 0.05 |
Bilateral PTA of RAS | 1.50 (0.81–2.80) | 0.20 | 1.65 (0.70–3.90) | 0.25 | 1.17 (0.48–2.84) | 0.73 | 1.75 (0.62–4.93) | 0.29 |
PTA of the one functioning kidney | 2.09 (1.07–4.08) | 0.03 | 2.27 (0.91–5.66) | 0.08 | 2.01 (0.82–4.97) | 0.13 | 2.10 (0.69–6.45) | 0.19 |
Diameter RAS, % | 1.00 (0.98–1.03) | 0.58 | 1.01 (0.98–1.03) | 0.65 | 1.00 (0.98–1.03) | 0.81 | 0.99 (0.96–1.03) | 0.91 |
Diameter stenosis post PTA, % | 1.02 (0.99–1.04) | 0.19 | 1.01 (0.97–1.05) | 0.65 | 1.29 (1.00–1.06) | 0.59 | 1.00 (0.95–1.06) | 0.90 |
Final follow‑up data | ||||||||
SBP decrease ≥20 mm Hg | 1.04 (0.56–1.93) | 0.88 | 0.34 (0.07–1.54) | 0.12 | 0.74 (0.34–1.56) | 0.43 | 0.34 (0.07–1.54) | 0.16 |
DBP decrease ≥5 mm Hg | 0.70 (0.38–1.28) | 0.25 | 0.25 (0.06–0.91) | 0.03 | 0.91 (0.42–1.95) | 0.81 | 0.25 (0.07–0.91) | 0.03 |
eGFR increase >11 ml/min/1.73 m2 | 0.51 (0.30–0.86) | 0.01 | 0.37 (0.18–0.78) | 0.01 | 0.52 (0.26–1.04) | 0.06 | 0.47 (0.18–1.19) | 0.11 |
Creatinine decrease >20 µmol/l | 1.39 (0.75–2.61) | 0.29 | 1.44 (0.56–3.72) | 0.45 | 1.55 (0.71–3.39) | 0.27 | 0.51 (0.11–2.5) | 0.37 |
The risk of CV death was associated with male sex (HR, 3.26; 95% CI, 1.33–8.00; P = 0.009), presence of atherosclerotic lesions (>50% stenosis) in at least 2 additional arterial territories (HR, 2.87; 95% CI, 1.29–6.40; P = 0.009), previous PTA in another arterial territory (HR, 5.84; 95% CI, 1.64–20.67; P = 0.006), history of hypertensive crisis (HR, 2.97; 95% CI, 1.35–6.55; P = 0.006), and concomitant atherosclerotic lesions (>30% stenosis) in the contralateral renal artery (HR, 2.83; 95% CI, 1.22–6.50; P = 0.03). An increase in eGFR by at least 11 ml/min/1.73 m2 at 12‑month follow‑up was independently associated with the reduction in the risk of CV death (HR, 0.42; 95% CI, 0.19–0.90; P = 0.03). A decrease in DBP by at least 5 mm Hg was related to a lower risk of IS (HR, 0.10; 95% CI, 0.02–0.39; P = 0.001). Other independent predictors are presented in Table 4.
Predictors | HR | 95% CI | P value | |
MACCEs | Male sex | 1.81 | 1.02–3.22 | 0.04 |
Multivessel CAD | 2.28 | 1.33–3.92 | 0.002 | |
History of hyperlipidemia | 9.27 | 1.13–5.73 | 0.04 | |
Concomitant atherosclerotic lesions in contralateral renal artery >30% | 2.24 | 1.31–3.83 | 0.003 | |
Increase in eGFR ≥11 ml/min/1.73 m2 at 12 months | 0.54 | 0.32–0.93 | 0.03 | |
Cardiovascular death | Male sex | 3.26 | 1.33–8.00 | 0.01 |
Multilevel CAD | 2.87 | 1.29–6.40 | 0.01 | |
Previous PTA in another arterial territory | 5.84 | 1.64–20.67 | 0.006 | |
History of hypertensive crisis | 2.97 | 1.35–6.55 | 0.006 | |
Concomitant atherosclerotic lesions in contralateral renal artery >30% | 2.83 | 1.22–6.50 | 0.015 | |
Increase in eGFR ≥11 ml/min/1.73 m2 at 12 months | 0.42 | 0.19–0.40 | 0.026 | |
MI | Male sex | 4.44 | 1.79–10.49 | 0.001 |
Multivessel CAD | 4.19 | 1.97–8.88 | 0.001 | |
Increase in eGFR ≥11 ml/min/1.73 m2 at 12 months | 0.64 | 0.32–1.29 | 0.21 | |
IS | Previous ischemic stroke | 5.27 | 1.57–17.79 | 0.007 |
Multilevel CAD | 6.76 | 1.66–27.57 | 0.007 | |
A decrease in DBP by ≥5 mm Hg at 12 months | 0.10 | 0.02–0.39 | 0.001 | |
Discussion
We showed high efficacy and safety of PTA for RAS, despite high‑risk profile of patients enrolled into the present study, with a substantial number of comorbidities and with advanced multilevel atherosclerosis. The overall procedural success was 99.2%, while the complication rate was 6.15%, including a periprocedural death rate of 0.47%. In other studies, the reported rates of procedure‑related mortality were estimated at 0.4% to 3%, and of total complications, at up to 20%.14,15,35
We demonstrated a significant reduction in the mean SBP of at least 12 mm Hg and DBP of at least 5 mm Hg. At the same time, successful hypertension treatment was possible in 1.94% of patients, while the mean number of antihypertensive drugs was not reduced.
In a study by Khan et al,7 SBP and DBP decreased by 26 mm Hg and 10 mm Hg after PTA, respectively, while the number of antihypertensive drugs was also reduced (mean [SD], 4.1 [1.0] to 2.7 [2.1]; P = 0.002) at 6 months. Both effects were sustained at long‑term follow‑up.
A meta‑analysis by Jenks et al,20 who pooled data from RCTs, showed a change in BP in the PTA group in comparison with the medical‑treatment group: a nonsignificant mean difference of –1.07 mm Hg for SBP (95% CI, –3.45 to 1.30; P = 0.38) and a significant mean difference of –2.00 mm Hg for DBP (95% CI, –3.72 to –0.27; P = 0.02). Similar results were presented in a meta‑analysis by Caielli et al36 with respect to BP reduction. Additionally, there was a significant reduction in the number of antihypertensive drugs after PTA as compared with medically treated patients.
The effect of PTA for RAS on renal function is at least controversial. Previous studies indicated renal improvement in 14% to 72% of patients with RAS, particularly those with advanced renal impairment at baseline.37,38 However, at the same time, about 20% to 25% of individuals experienced further deterioration of renal function.9,35,36
Jenks et al20 reported a nonsignificant mean difference of creatinine levels between groups treated medically vs those treated with PTA in combination with medical treatment. In our study, we also failed to show a significant decrease in serum creatinine levels after the procedure.
There is an ongoing debate as to which patients are likely to respond to renal artery stenting (in terms of improvement in kidney function or hypertension) and which patients are not. In a study by Kim et al,39 patients with a high‑risk profile at baseline (defined as having 1 or more of the following: pulmonary edema, refractory hypertension, and rapid deterioration of kidney function) were most likely to be classified as responders. High initial BP values or bilateral RAS should also be considered as predictors of favorable response to PTA.40,41
Despite the immediate clinical effect of the PTA, its influence on all‑cause mortality, CV mortality, and adverse renal or CV events is debatable.9,11,15,40,42 In the present study, during a median follow‑up of 47 months, we observed all‑cause mortality, CV death, MACCEs, and end‑stage renal failure in 23.3%, 13.6%, 30.6%, and 5.8% of patients, respectively. Vassallo et al,40 in a study on 112 patients after PTA for RAS, who were followed for a median of 59.9 months, reported death in 75 patients (67%); CV events, in 36 (32.1%); and end‑stage kidney disease, in 21 (18.7%).
Wright et al42 confirmed that PTA for RAS is associated with a reduction in the risk of CV events and a 45% reduction in all‑cause mortality, irrespective of the achieved goals. Also Kalra et al37 and Kennedy et al43 reported better survival in revascularized patients with renal insufficiency. In contrast, none of the RCTs have shown that revascularization of RAS improves CV outcome or confers an added benefit to optimal medical therapy in unselected populations.13,14,16
To our knowledge, our present study is the first to demonstrate that improvement of renal function, defined as an increase in eGFR (calculated by the MDRD formula) of at least 11 ml/min/1.73 m2 (but without a change in serum creatinine levels), was associated with a significant reduction in the risk of MACCEs and CV death. We used the MDRD formula to calculate eGFR because it was shown to provide a less biased estimate and the highest accuracy in patients with reduced renal function.44 Our finding is important because patients with progressive renal failure quickly develop end‑stage renal disease, which considerably worsens the 1‑year survival.45 Of note, RAS is common in patients with coronary and extracoronary athero‑occlussive disease.46 Furthermore, a decrease in DBP by at least 5 mm Hg at 6- to 12‑month follow‑up after PTA was related to 90% reduction in the risk of future IS. Our data indicated a significant decrease in DBP ≥5 mm Hg and MDRD increase by 11 ml/min/1.73 m2 was noted in 45.6% and 23.8% subjects respectively.
In a study by Vassallo et al,46 PTA for RAS was associated with survival benefit in patients presenting with pulmonary flash edema (HR, 0.4; 95% CI, 0.2–0.9; P = 0.01). Only patients with N‑terminal fragment of the prohormone brain natriuretic peptide levels higher than 300 ng/l gained benefit from revascularization with regard to all adverse endpoints compared with patients on medical treatment.42,47 The same investigators reported that revascularization improved outcomes in patients with higher baseline eGFR and lower proteinuria but not in those with coexisting comorbidities and baseline proteinuria exceeding 1 g/d.48 In contrast, in a study by Green et al,11 including 152 patients with coexisting heart failure, with or without a history of acute pulmonary edema, PTA for RAS did not reduce the rate of hospitalization for heart failure, as compared with medical therapy.
Our study indicated a number of independent clinical parameters associated with the risk of MACCEs, MI, IS, and CV death, such as male sex, multilevel athero‑occlusive disease or multivessel coronary artery disease, previous PTA in another arterial territory, history of hypertensive crisis, and concomitant atherosclerotic lesions (>30% stenosis) in the contralateral renal artery. These risk factors are similar to those reported by studies in patients with advanced multiterritorial occlusive disease.49,50
In light of our present findings, the CV prognosis can be improved in a significant proportion of patients. The key unresolved issue is how to identify patients in whom renal function and DBP can be improved above the calculated thresholds.
Limitations
Our study has several limitations, including a retrospective, single‑center observational design, long‑term patient enrollment resulting in a possible bias in the treatment procedure and medical therapy, as well as the lack of a control group. Other limitations are lack of data on proteinuria, kidney diameter, and renal resistive index.
Conclusions
In high‑risk patients, PTA of atherosclerotic RAS is an effective and safe procedure. The increase in eGFR of at least 11 ml/min/1.73 m2 is associated with a significant reduction of MACCEs and CV death during follow‑up, while a decrease in DBP of at least 5 mm Hg is related with 90% reduction in the risk of IS. The threshold values associated with the reduction in the risk of adverse CV events were observed in 45% of patients for DBP and in 23.8% of patients for eGFR.
- Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: the European Stroke Organization (ESO). The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018; 39: 763‑816. | Crossref
- Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013; 127: 1425‑1443. | Crossref
- Zeller T, Frank U, Müller C, et al. Predictors of improved renal function after percutaneous stent‑supported angioplasty of severe atherosclerotic ostial renal artery stenosis. Circulation. 2003; 108: 2244‑2249. | Crossref
- Rocha‑Singh K, Jaff MR, Lynne Kelley E; RENAISSANCE Trial Investigators. Renal artery stenting with noninvasive duplex ultrasound follow‑up: 3‑year results from the RENAISSANCE renal stent trial. Catheter Cardiovasc Interv. 2008; 72: 853‑862. | Crossref
- Beck AW, Nolan BW, De Martino R, et al. Predicting blood pressure response after renal artery stenting. J Vasc Surg. 2010; 51: 380‑385. | Crossref
ARTICLE INFORMATION