Emphysema affects the number and characteristics of solitary pulmonary nodules identified by chest low-dose computed tomography. A study on screenees with high-risk lung cancer recruited in Upper Silesia
Key words: by Chilet-Rosell and Lumbreras, see p. 4



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Emphysema affects the number and characteristics of solitary pulmonary nodules identified by chest low-dose computed tomography. A study on screenees with high-risk lung cancer recruited in Upper Silesia
Introduction: Chest low‑dose computed tomography (LDCT) has recently been proved effective in lung cancer screening.
Objectives: We aimed to assess the association between the occurrence of emphysema and solitary pulmonary nodules (SPNs) in first‑round screening with LDCT.
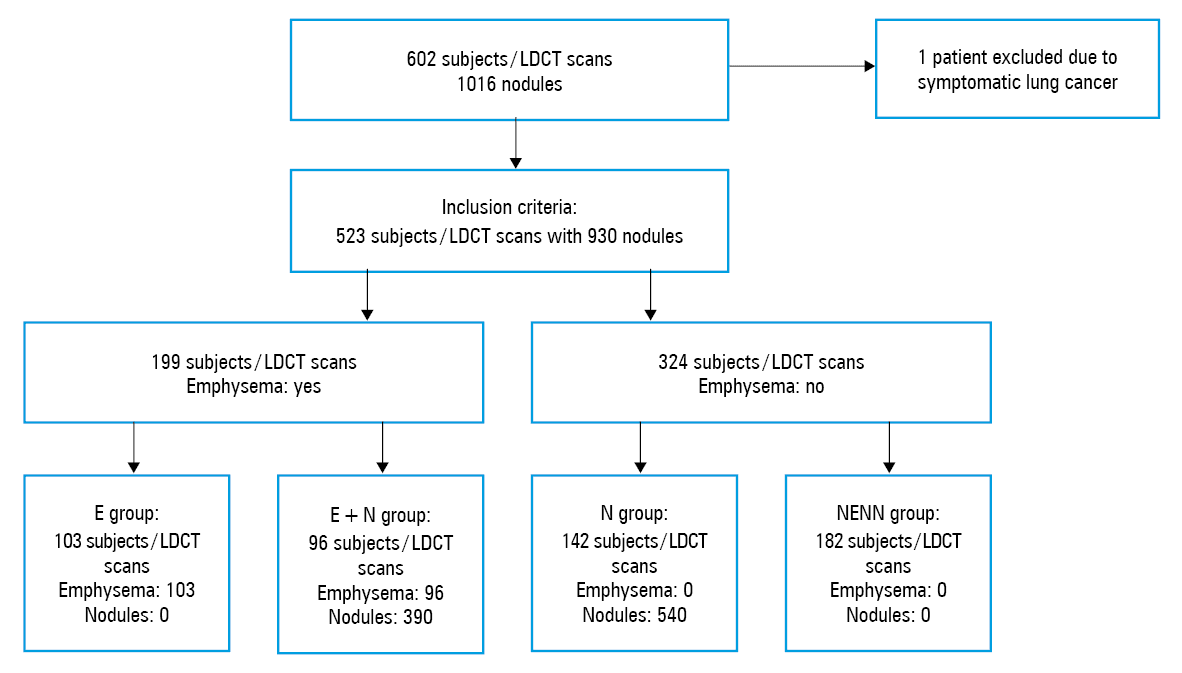
Patients and methods: A total of 601 asymptomatic volunteers with a smoking history underwent LDCT; 523 patients were assigned to one of the following groups: E, emphysema without nodules (n = 103); E+N, emphysema with coexisting nodules (n = 96); N, nodules without emphysema (n = 142); and NENN, no nodules and no emphysema (n = 182). The effect of emphysema and demographic factors on the profile of SPNs was assessed.
Results: Patients in the E+N group were older than those in the N group (median age, 65 vs 63 years; P = 0.001) and they smoked more (median pack‑years, 37.8 vs 32; P = 0.01). Emphysema was detected in 199 of the 523 patients (38%), while nodules, in 238 (45.5%). The number of nodules in the E+N group was 390 (4.1 nodules per patient), and in the N group, 540 (3.8 nodules per patient). Multiple SPNs, of different size and morphology, constituted 93.3% of the nodules in the E+N group. Seven cases of cancer were detected among 238 patients with nodules, and their distribution was similar in the groups with and without emphysema (4.2 per 100 patients in the E+N group and 2.1 per 100 in the N group; P = 0.44).
Conclusions: Emphysema was more frequently associated with multiple SPNs of different morphology among elderly patients with a higher number of smoking pack‑years.
What's new?
Low‑dose computed tomography (LDCT) for lung cancer screening not only detects lung nodules that are early‑stage lung cancer but also reveals other important lung findings, such as the presence of emphysema. Screening with LDCT has been proved to reduce mortality in a high‑risk group of heavy smokers aged over 50 years, but it should not be used in all populations. Research is ongoing to find the most optimal factors for patient selection for screening tests. Some results showed that the coexistence of emphysema with lung nodules can affect carcinogenesis. In our study, the morphology, size, and location of pulmonary nodules differed between patients with and without emphysema. Emphysema was more common in older people with higher tobacco consumption. However, the distribution of lung cancer was similar between groups.
Introduction
According to the Surveillance, Epidemiology and End Results (SEER) database, lung cancer is the leading cause of cancer‑related mortality, accounting for 1.6 million deaths annually in men and women.1 Chronic respiratory diseases including chronic obstructive pulmonary disease (COPD) and emphysema are the fourth leading cause of death in the United States and worldwide (>2.5 million deaths annually).2 The etiology of lung cancer and chronic respiratory diseases is strongly linked to tobacco exposure and environmental pollution.3,4 Additionally, it was documented that both diseases share some common genetic mechanisms involving iron metabolism and single nucleotide polymorphisms of proteolytic enzymes, which may give rise to similar metabolomic biomarkers.5-7 Kuźnar‑Kamińska et al8 reported that COPD and lung cancer are age‑related diseases, in which senescent cells can produce multiple agents collectively termed “senescence‑messaging secretome,” such as interleukins, chemokines, and growth factors. Some of them may be involved in lung carcinogenesis.8
Late detection of lung cancer, often as a locally advanced or metastatic disease, results in poor treatment outcome. Only 15% of lung cancer cases are diagnosed at an early stage, when the tumor size is smaller than 5 cm (T2a according to the TNM classification), the patient is asymptomatic, and the lesion is resectable. According to the Domestic Lung Cancer Database (KBRP) of the National Institute of Tuberculosis and Lung Diseases (Instytut Gruźlicy i Chorób Płuc [IGiChP]), which comprises patients who have had pulmonary resection, each year around 3500 individuals undergo a surgery for lung cancer. This means that approximately 18% of patients diagnosed annually with lung cancer in Poland are candidates for surgical resection. Out of 35443 patients who had undergone surgery (lobectomy, segmentectomy, or pneumonectomy) within 10 years (2007–2017), 83% had been diagnosed with lung cancer stages I and II, while 17%, with early stage IIIA (with invaded mediastinal lymph nodes [N2 disease in the TNM classification], amenable to surgical removal). In these patients, the 5‑year survival rate is approximately 55%, while the overall 5‑year survival rate worldwide and in Poland equals to 16% and 14.4%, respectively.9
To improve treatment outcomes, and thus to reduce lung cancer mortality, lung cancer screening with low‑dose computed tomography (LDCT) has been introduced. This modality allows a detection of early‑stage lung cancer in high‑risk individuals. Screening with LDCT among individuals over 55 years of age with a smoking history of at least 30 pack‑years was shown to reduce the relative risk of death by 20% (95% CI, 6.8–26.7; P = 0.004).10,11 Moreover, LDCT screening has been recommended by most scientific societies, including the U.S. Preventive Services Task Force since 2014, as well as the American College of Radiology and the National Comprehensive Cancer Network (NCCN) since 2015.12-14 In Poland, a health policy program for the detection of early lung cancer, funded by the European Union, will be launched.15
There is evidence showing that almost 80% of patients undergoing LDCT screening had solitary pulmonary nodules (SPNs) coexisting with COPD or emphysema, which is associated with a less favorable outcome.16-18 As a result, some investigators suggested that the presence of COPD or emphysema should be considered an inclusion criterion for lung cancer screening.17-20
In this study, we aimed to provide data to support a hypothesis that the coexistence of SPNs along with emphysema may be a susceptibility factor for SPN malignancy.
The study was designed to determine the possible effect of additional factors (such as age, sex, and tobacco consumption) on the quantitative and qualitative features of the nodules.
Patients and methods
Study design and participants
The analysis was performed using data from the Pilot Silesian Study for Early Lung Cancer Detection with LDCT. Participants were recruited between 2010 and 2012. A total of 602 volunteers older than 46 years, current or former smokers (who quitted smoking within the previous 15 years) or never‑smokers but with a high risk of lung cancer, were examined. After applying the inclusion criteria (age over 50 years and a smoking history of at least 20 pack‑years), the total number of participants was 524. One patient was excluded from statistical analysis due to symptoms related to advanced lung cancer. This resulted in the final study sample of 523 individuals. The population comprised residents of Upper Silesia, which indicated an additional exposure to risk factors related to heavy industry. The study group included 272 men (52%) and 251 women (48%). The median age of participants was 63 years (interquartile range [IQR], 9 years; range, 52–85 years). Demographic data and information on smoking history was obtained using a survey. Emphysema was diagnosed in 199 patients, and the total number of detected SPNs was 930.
Low‑dose computed tomography protocol and data collection
Participants underwent baseline LDCT screening, performed and assessed at 5 selected radiology centers in Silesia. Imaging was performed with a 4‑row detector computed tomography (CT) scanner (imaging protocol, 120–140 kVp; 40–80 mA; 1.25‑mm slice thickness including minimal available pitch, field of view from the thoracic inlet to the adrenal gland). The procedure was performed by designated radiologists who followed appropriate guidelines on the use of equipment as well as general screening standards. All scans were performed in full inspiration without intravenous contrast administration. The LDCT reading was done by experienced radiologists using workstation equipped with high‑resolution monitors.
A bidimensional measurement of detected SPNs was performed by visualizing transverse sections with lung window settings (1500 Hounsfield units [HU]/–650 HU), while abnormal mediastinal structures were measured and assessed with mediastinal window settings (350 HU/25 HU). The scan descriptions were presented in written and digital form and stored in a database. Every diagnostic uncertainty was consulted with a pulmonologist.
Only first‑round LDCT scans (baseline/prevalence screening) were assessed, excluding subsequent rounds and follow‑up studies. Data from study descriptions were stored in our own relational database including the following characteristics: the size and number of nodules, localization, morphology, presence of emphysema, and other pulmonary and extrapulmonary findings. Data were classified into 4 groups: E, emphysema without nodules; E+N, emphysema coexisting with nodules; N, nodules without emphysema; and NENN, no nodules or emphysema detected. The analysis per participant and per population was conducted. The flowchart of study design is shown in Figure 1.
Characteristics of emphysema
Emphysema was diagnosed by radiologists on the basis of the World Health Organization’s definition and American Thoracic Society guidelines when the enlargement of any part or all of the acinus accompanied by destruction of the lung parenchyma was present.21-23 On radiologic assessment, emphysema was identified as low attenuation areas (LAAs) below a specific threshold of –950 HU (%LAA, –950).24 Emphysema was also assessed visually and reported as present or absent. Finally, on the basis of morphology, emphysema was classified as panlobular, centrilobular, mixed, or undetermined.
Characteristics of pulmonary nodules
Each pulmonary noncalcified lesion was measured with lung window settings, while abnormal structures of the mediastinum were assessed.
Pulmonary nodules were defined according to the British Thoracic Society’s definition25-27 as a rounded or irregular opacity, with a diameter of 3 cm or more, surrounded by an aerated lung. The quantitative and qualitative characteristics of nodules were assessed.
Lesions were categorized in quantitative terms as single or multiple SPNs. Qualitatively, each SPN was classified according to its size (transverse diameter expressed in millimeters), localization (right lung, left lung, or both lungs), morphology (solid, part‑solid, or nonsolid). The nodule was defined as solid if the underlying bronchoalveolar architecture could not be visualized. Nonsolid and part‑solid nodules (including both solid and ground glass opacities) were defined as the focal areas of increased lung attenuation through which lung parenchymal structures could be seen. Each CT scan with at least 1 noncalcified nodule was assessed, while calcified nodules were excluded from the analysis and considered as nonsuspicious lesions. Nodules confirmed to be primary lung cancer on pathologic examination were assigned to one of the groups: N, E+N, E, or NENN.
Ethics
Prior to LDCT, each patient completed and signed the informed consent form. The study protocol was approved by the Research Ethics Committee of the Medical University of Silesia, Katowice, Poland (KNW/0022/KB/38/16).
Statistical analysis
Statistical analysis was performed with Dell Statistica, version 13 (Statistica, Tulsa, Oklahoma, United States). Quantitative variables were expressed as means (SD) or medians (IQR), while qualitative variables were presented as the total number of events and percentage. The conformity of data to a normal distribution was evaluated with the Shapiro–Wilk test. As data were not normally distributed, the significance between 2 groups was assessed using the Mann–Whitney test for quantitative data and the χ2 test for qualitative data. The χ2 test was used to compare proportions. In the case of disturbed assumptions in the χ2 test, the Fisher test was performed. The 2‑tailed tests were conducted, and a P value of less than 0.05 was considered to be significant in all analyses.
Results
Population characteristics
The study group included 523 patients (251 women and 272 men). Emphysema was identified in 199 participants (38%), including 90 women (35.9%) and 109 men (40.1%). The presence of emphysema was similar in both sexes. Patients with emphysema were older than those without. Data are presented in Table 1. Additionally, patients with emphysema were more heavy smokers (median [IQR] number of pack‑years, 37.5 [15] vs 32.4 [14]; P = 0.001).
Parameter | Total (n = 523) | Emphysema (n = 199); E and E+N groups | No emphysema (n = 324); N and NENN groups | P value | |
A P value of less than 0.05 was considered significant.
a χ2 test
b Mann–Whitney test
Abbreviations: IQR, interquartile range; others, see Figure 1 | |||||
Sex, n | Male | 272 | 109 | 163 | 0.32a |
Female | 251 | 90 | 161 | ||
Age, y | Mean | 63.8 | 65.6 | 62.6 | <0.001b |
Median | 63 | 65 | 62 | ||
SD | 6.5 | 6.8 | 6 | ||
IQR | 9 | 10 | 9 | ||
Smoking, pack‑years | Mean | 37.2 | 39.7 | 35.6 | 0.001b |
Median | 35 | 37.5 | 32.4 | ||
SD | 14.6 | 16 | 13.4 | ||
IQR | 16.3 | 15 | 14 | ||
Occurrence and morphology of solitary pulmonary nodules in the study group
Lung nodules were detected in 238 of the 523 individuals (45.5%), of whom 96 (40.3%) were diagnosed with both pulmonary nodules and emphysema (E+N group). The groups with pulmonary nodules were similar in terms of sex distribution but differed in terms of age (median [IQR] age, 66 [9.5] years in the E+N group vs 63 [9]years in the N group; P <0.001). Similarly, patients in the E+N group had a higher number of pack‑years in comparison with the N group (mean [IQR], 37.8 [18.5] vs 32 [15]; P = 0.01). Data are presented in Table 2.
Parameter | Total (n = 238); E+N and N groups | Nodules and emphysema (n = 96); E+N group | Nodules and no emphysema (n = 142); N group | P value | |
A P value of less than 0.05 was considered significant.
a χ2 test
b Mann–Whitney test
| |||||
Sex, n | Male | 119 | 53 | 66 | 0.19a |
Female | 119 | 43 | 76 | ||
Age, y | Mean | 65.5 | 66.3 | 63.4 | <0.001b |
Median | 64 | 66 | 63 | ||
SD | 6.1 | 6.3 | 5.7 | ||
IQR | 9 | 9.5 | 9 | ||
Smoking, pack‑years | Mean | 36.8 | 39.8 | 34.7 | 0.01b |
Median | 34.5 | 37.8 | 32 | ||
SD | 13.9 | 15.1 | 12.7 | ||
IQR | 14.8 | 18.5 | 15 | ||
The majority of nodules (58.1%) were detected in patients without emphysema (N group). Data on the size, number, and morphology of nodules in each subgroup are presented in Tables 3 and 4.
Parameter | Nodules, E+N and N groups (n = 238); all nodules (n = 930) | Emphysema (n = 199) | No emphysema (n = 324) | P value | ||
E group (n = 103); without nodules | E+N group (n = 96); nodules (n = 390) | N group (n = 142); nodules (n = 540) | NENN group (n = 182); without nodules | |||
Qualitative variables are presented as number (percentage). A P value of less than 0.05 was considered significant.
a The mean size of nodules was obtained for each patient by determining weighted average in accordance with the following formula (the numbers by which the number of nodules is multiplied are the average size in range, and for the group of nodules measuring over 20 mm, there was an arbitrary number): the mean size of the nodule = 2*number of nodules [0–4 mm) + 5*number of nodules [4–6 mm) + 7*number of nodules [6–8 mm) + 11.5*number of nodules [8–14 mm) + 17*number of nodules [14–20 mm] + 23.5*>20 mm, where “)” means <, and “[“ means ≥.
b χ2 test
c Mann–Whitney test
Abbreviations: SPN, solitary pulmonary nodule; others, see Figure 1 | ||||||
Number of nodules depending on size (quantitative analysis) | ||||||
Size ≤5 mm | 750 (80.6) | – | 297 (76.2) | 456 (84.4) | – | 0.003b |
Size >5 mm | 180 (19.4) | – | 93 (23.8) | 87 (15.6) | – | |
Size of SPNsa | ||||||
Mean | 16.7 | – | 18.2 | 15.7 | – | 0.047c |
Median | 11.5 | – | 12 | 10 | – | |
SD | 18.8 | – | 18.8 | 18.7 | – | |
IQR | 15 | – | 13 | 15 | – | |
Localization | ||||||
Left lung | 43 (18.1) | – | 17 (17.7) | 26 (18.3) | – | 0.22b |
Right lung | 101 (42.4) | – | 35 (36.5) | 66 (46.5) | – | |
Both lungs | 94 (39.5) | – | 44 (45.8) | 50 (35.2) | – | |
Quantitative status | ||||||
Single SPN | 89/238 (37.4) | – | 27/96 (28.1) | 62/142 (43.6) | – | 0.02b |
Multiple SPNsa | 149 (62.6) | – | 69 (71.9) | 80 (56.3) | – | |
Morphology of SPNs (per number of patients) | ||||||
Solid | 122 (51.3) | – | 49 (51.4) | 73 (51.4) | – | 0.01b |
Part‑solid | 50 (21) | – | 12 (12.5) | 38 (26.8) | – | |
Nonsolid | 65 (27.3) | – | 35 (36.5) | 30 (21.1) | – | |
Parameter | All nodules (n = 930) | E+N group (n = 390) | N group (n = 540) | P valuea | |
Qualitative variables are presented as number (percentage). P value of less than 0.05 was considered significant.
a χ2 test
| |||||
Size, mm | 0–3 | 466 (50.1) | 198 (50.8) | 268 (49.6) | 0.01 |
4–5 | 284 (30.5) | 99 (25.4) | 185 (34.3) | ||
6–7 | 122 (13.1) | 59 (15.1) | 63 (11.7) | ||
8–14 | 46 (4.9) | 27 (6.9) | 19 (3.5) | ||
>15 | 12 (1.3) | 7 (1.8) | 5 (0.9) | ||
Localization | Left lung | 74 (8) | 30 (7.7) | 44 (8.2) | 0.001 |
Right lung | 235 (25.3) | 75 (19.2) | 160 (29.6) | ||
Both lungs | 621 (66.8) | 285 (73.1) | 336 (62.2) | ||
Number | Single SPN | 85 (9.1) | 26 (6.7) | 59 (10.9) | 0.03 |
Multiple nodules | 845 (90.9) | 364 (93.3) | 481 (89.1) | ||
Morphology | Solid | 358 (38.5) | 126 (32.3) | 232 (43) | <0.001 |
Part‑solid | 184 (19.8) | 42 (10.8) | 142 (26.3) | ||
Nonsolid | 387 (41.6) | 222 (56.9) | 165 (30.6) | ||
Not specified | 1 (0.1) | 0 (0) | 1 (0.2) | ||
There was a trend for larger nodules in the E+N group, as compared with the N group: median (IQR), 12 (13) mm vs 10 (15) mm (P = 0.047). The quantitative analysis revealed that multiple nodules occurred more often in the E+N than in the N group, (71.9% vs 56.3%; P = 0.02).
Considering the morphology of the nodules, we observed that while the presence of solid nodules was similar in all groups, there was a 2‑fold higher percentage of patients with part‑solid nodules in the N group and a higher percentage of patients with nonsolid nodules in the E+N group. Detailed data are presented in Table 3.
In our study, emphysema was identified in 199 patients, with an undetermined type detected in 166 individuals (83.4%) and determined types (panlobular, centrilobular, and mixed) in 33 (16.6%).
Quantitative and qualitative analysis of solitary pulmonary nodules in participants with and without emphysema
The characteristics of nodules in the emphysema and non–emphysema groups are shown in Table 4. A total of 930 pulmonary nodules were detected in 523 LDCT scans, of which 390 SPNs coexisted with emphysema (41.9%). The number of nodules tended to decrease with an increasing nodule size (Table 4).
Pulmonary nodules were reported more often in the right than in the left lung, irrespective of the presence of emphysema (P = 0.001). In both groups, we observed a similarly smaller percentage of nodules located in the left lung (P = 0.001), with a tendency for localization in both lungs. However, the N group showed a notably higher percentage of nodules located in the right lung than the E+N group (Table 4).
More than 90% of SPNs were multiple nodules (845 of 930). The quantitative analysis revealed that multiple SPNs were more common than single ones in individuals with emphysema. Moreover, single SPNs were detected more often in the N group than in the E+N group (Table 4).
The E+N and N groups differed considerably in terms of the morphological types of nodules, with nonsolid SPNs predominating in the group with emphysema and solid ones being more common in the non–emphysema group (Table 4). Additionally, the occurrence of determined types of emphysema (panlobular, centrilobular, mixed) was higher in the E+N group than in the E group (26 [27.1%] vs 7 [6.8%], P <0.001). On the other hand, an undetermined type of emphysema predominated in the E group, as compared with the E+N group (96 [93.2%] vs 70 [72.9%], respectively; P <0.001).
Characteristics of lung cancer
The workup of first‑round LDCT scans with suspicious SPNs allowed an identification of 7 cases of early‑stage lung cancer (2.9% of detected cancers among 238 LDCT scans with nodules), of which 4 were diagnosed in the E+N group and 3 in the N group. Lung cancer tended to occur with a similar frequency in patients with and without emphysema (4.2 vs 2.1 per 100 patients; 2‑tailed Fisher exact test, P = 0.44). All malignant SPNs (ie, early lung cancer) had solid morphology. The following histopathologic types of lung cancer were identified: 2 cases of squamous cell carcinoma, 2 cases of mixed cancer (adenocarcinoma coexisting with large cell cancer; small cell cancer with large cell cancer), 2 cases of adenocarcinoma, and 1 case of large cell carcinoma. The majority of lung cancers were diagnosed in stage I (6 in IA and 1 in IB). One cancer lesion was missed due to its nonsuspicious size and morphology (false‑negative result), while in 1 patient, a growing sarcoid nodule was removed (false‑positive result).
Discussion
Our study showed that SPNs tend to coexist with emphysema more frequently among current smokers, particularly in elderly patients. However, we did not show a more frequent occurrence of malignant lung nodules in the emphysema group. We focused on the relationship between SPNs and emphysema to confirm its relevance for screening inclusion criteria. It is likely that the emphysema‑modified microenvironment of the peripheral airways and alveoli is one of the predictive factors for neoplastic transformation, and, as such, it may serve as a radiologic biomarker of suspicious pulmonary nodules. Accumulating evidence confirms an association between the presence of emphysema and the incidence of lung cancer as well as cancer‑related mortality, regardless of smoking history, degree of obturation, and nodule size.17,28-33 Hohberger et al34 reported that severe local emphysema occurs more frequently in patients with malignant than with benign nodules (1.34 vs 1.12, respectively; 95% CI, 1.112–1.620; P = 0.002 vs 95% CI, 0.725–1.725; P = 0.61). Nevertheless, the analysis was conducted using different resolutions and radiation doses in diagnostic CT. Using data and images from the National Lung Screening Trial, Liu et al35 reported that perinodule and total emphysema associated with SPNs was a predictive factor of lung cancer risk, together with a positive screening result (noncalcified nodules ≥4 mm; P <0.001).
The majority of detected SPNs were benign lesions, determined by histopathology as granulomas (organized collections of epithelioid macrophages and other inflammatory cells) or hamartomas in 40% and 15% of cases, respectively. With regard to multiple nonneoplastic SPNs, tuberculosis and sarcoidosis were most often diagnosed.36 Apart from lung cancer, malignant nodules were identified as mesotheliomas, thyroid cancer, and metastases from the primary site of origin, most commonly from the breast.14 The results of the quantitative analysis demonstrated that single SPNs were detected less often than multiple SPNs: in 89 participants (37.4%) and 149 individuals (62.6%), respectively. Of note, single SPNs were diagnosed more frequently in patients without emphysema (P = 0.02). Multiple pulmonary nodules coexisting with emphysema might be explained by a long‑lasting exposure to tobacco smoke and the resultant chronic inflammation in the lung parenchyma.
Most frequent lesions found in the lungs of tobacco smokers are tiny, benign SPNs (≤5 mm),37 which in our study constituted 80.6% of the nodules (n = 750). A nodule diameter or volume has been well documented as a factor associated with the risk of malignancy.26-28 According to the NELSON study (Dutch‑Belgian Randomized Lung Cancer Screening Trial), the risk of lung cancer was lower in participants with a nodule volume lower than or equal to 100 mm3 or the maximum nodule size lower than 5 mm.38
It was reported that nonsolid SPNs are malignant in 63% of cases, while pure ground glass and solid nodules in 18% and 7% of cases, respectively.39-42 In our cohort, over half of diagnosed nodules were solid, followed by nonsolid and part‑solid. However, the limitation of this study is the lack of central reading of CT scans. The results were reported by a few independent radiologists, which may have led to the underestimation of some nodule subclasses. Nevertheless, a pathologic and immunohistochemical analysis still remains the only examination to assess the nodule type, despite the development of modern molecular diagnostic methods and radiomics.
Our findings may suggest a correlation between emphysema and qualitative and quantitative characteristics of pulmonary nodules. However, an important limitation of our study is the small size of the study group. In addition, the population included only inhabitants of a highly urbanized area of Poland, characterized by excessive air pollution. About 50% of participants were industry employees, including coal miners (n = 117) and asbestos workers (n = 76). This may have had a significant impact on the development of lung lesions. Another limitation is a subjective visual interpretation of emphysema by radiologists. The results of other studies, with larger populations and using more precise methods, demonstrated the higher risk of lung cancer in patients with COPD regardless of tobacco consumption, especially in the presence of emphysema.28-31 The rate of early lung cancer cases diagnosed during the first round of screening in our cohort (1.34%, 7 cancers per 523 patients) was similar to that reported by other Polish screening university centers: 1.24% in Gdańsk and 0.7% in Szczecin.43,44
Clinical studies have shown that emphysema with or without COPD is a significant risk factor of lung cancer, even in nonsmokers (hazard ratio, 1.66; 95% CI, 1.06–2.59).45,46 The predictive value of COPD in lung cancer (high‑risk group according to NCCN v. 2.2019)14 is high enough to consider lower pack‑year thresholds for screening eligibility.20 It seems reasonable to consider additional examinations (eg, spirometry) prior to referring current smokers for screening in order to detect COPD or emphysema. de‑Torres et al47 evaluated risk factors for lung cancer in patients with COPD confirmed by spirometry, using LDCT scans from the Pittsburgh Lung Screening Study database and Pamplona International Early Lung Cancer Action Detection Program database. As shown by the authors, age older than 60 years, body mass index lower than 25 kg/m2, a smoking history of at least 60 pack‑years, and emphysema are independent risk factors for lung cancer.47 Our study showed that emphysema was diagnosed more frequently among elderly participants regardless of the presence of nodules.
A number of studies reported a correlation between emphysema and a histological type of lung cancer. Shin et al48 evaluated 754 patients with lung cancer and reported an association between emphysema and squamous cell carcinoma, while adenocarcinoma more often occurred in areas with no emphysema. These results were in line with a study by Mouronte‑Roibás et al,49 who reported that patients with lung cancer and COPD were predominately men with a long history of smoking and squamous cell carcinoma. Patients with lung cancer had a similar median survival as those with lung cancer and COPD (22 vs 16 months).49
However, not all studies reported a positive correlation between emphysema and lung cancer. Maldonado et al50 did not confirm the effect of emphysema on the frequency of malignant nodule diagnosis.
It is obvious that the first‑round LDCT examination is not sufficient to assess cancerous transformation of nodules. To achieve this goal, more sophisticated methods should be employed, including volume doubling time, nodule volume growth, as well as blood‑derived biomarkers such as CD14+ cells, circulating tumor DNA, and microRNA. The same applies to the detection of emphysema, as there may be discrepancies depending on the methodology used (eg, visual vs automatic quantitative and densitometric assessment) or the site of emphysema (eg, perinodular vs panlobular).
In conclusion, the morphology, size, site, and quantitative status of nodules differ between patients with and without emphysema. In our cohort, patients with emphysema were older and were more heavy smokers. The distribution of cancer did not differ between the study subgroups, possibly because of a small sample size. Our research provides a novel insight into the correlations between radiographic pulmonary findings; nevertheless, the results should be confirmed in well‑planned prospective studies.
- Noone AM, Howlader N, Krapcho M, et al. SEER Cancer Statistics Review, 1975‑2015. National Cancer Institute. Bethesda, MD. https://seer.cancer.gov/csr/1975_2015/. Based on November 2017 SEER data submission. Published April 2018. Updated September 10, 2018. Accessed February 26, 2019.
- Zulueta JJ, Wisnivesky JP, Henschke CI, et al. Emphysema scores predict death from COPD and lung cancer. Chest. 2012; 141: 1216‑1223. | Crossref
- Dai J, Yang P, Cox A, et al. Lung cancer and chronic obstructive pulmonary disease: from a clinical perspective. Oncotarget. 2017; 8: 18513‑18524. | Crossref
- Denholm R, Schuz J, Straif K, et al. Is previous respiratory disease a risk factor for lung cancer? Am J Respir Crit Care Med. 2014; 190: 549‑559. | Crossref
- Brzoska K, Bartlomiejczyk T, Sochanowicz B, et al. Carcinogenesis‑related changes in iron metabolism in chronic obstructive pulmonary disease subjects with lung cancer. Oncol Lett. 2018; 16: 6831‑6837. | Crossref
ARTICLE INFORMATION