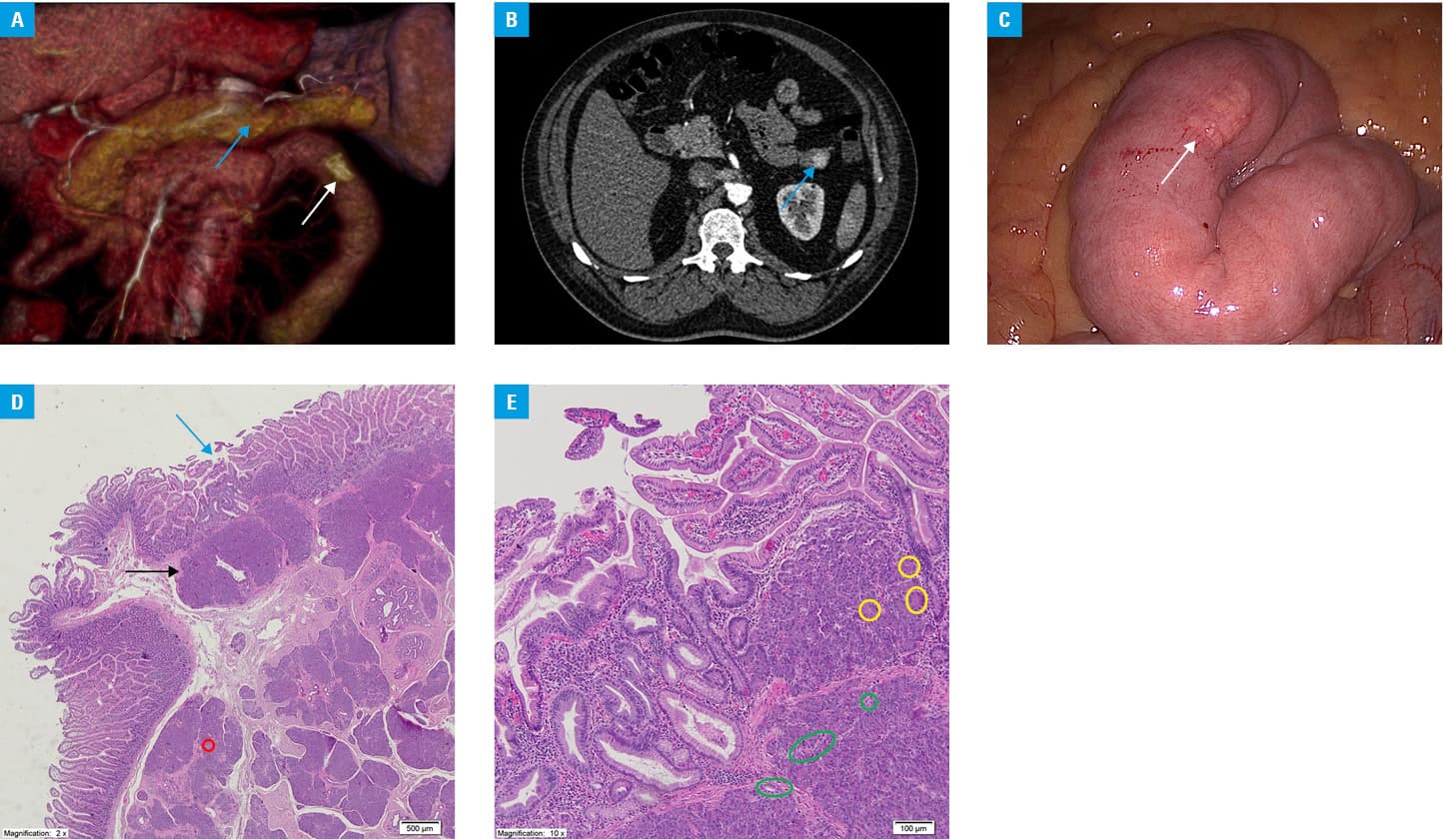
A 49‑year‑old man was referred to our hospital after a mass adjacent to the first jejunal loop was incidentally found on control computed tomography (CT) after treatment for pulmonary embolism (Figure 1A and 1b). No evident signs or symptoms were revealed in medical history or on physical examination. The preoperative CT scan showed a round endoluminal mass with homogenous enhancement of the overlying mucosa (Figure 1B).1 After an interdisciplinary discussion, a tentative diagnosis of gastrointestinal stromal tumor (GIST) was made, and the patient was referred for surgery. The mass was successfully removed with laparoscopic resection (Figure 1C). The specimen was sent for a histopathologic examination, which revealed a well‑differentiated ectopic pancreas (type 1 according to the Fuentes classification), with a normal intestinal wall, extending to the submucosal and muscularis propria of the jejunum (Figure 1D and 1E). The postoperative course was uneventful. At a follow‑up visit, the patient was in good condition.
An ectopic pancreas is a rare developmental anomaly, which usually remains asymptomatic, but in some cases, complications such as hemorrhage, obstruction, ulceration, or malignant transformation may result in a symptomatic presentation.2 About 70% of ectopic pancreatic lesions are found in the stomach and duodenum.2 The differential diagnosis for ectopic pancreas must include GIST, lymphoma, carcinoid tumors, and desmoid tumor.3 Ji et al1 demonstrated that certain CT findings help differentiate the ectopic pancreas from other gastrointestinal submucosal tumors. The ectopic pancreas usually presents as endoluminal, flat, or ovoid masses with irregular borders and prominent enhancement of the overlying mucosa on CT imaging.1 However, even with such diagnostic criteria, the definitive diagnosis can only be made on the basis of histopathology.
Gastrointestinal stromal tumors are the most common mesenchymal tumors of the gastrointestinal tract.4 They are slow‑growing tumors that are most frequently identified as incidental findings in asymptomatic patients, similarly to the ectopic pancreas. They may also produce nonspecific symptoms such as abdominal pain, nausea, anorexia, vomiting, and fever. The malignant potential of GIST depends on the size of the tumor; therefore, any lesions that measure 2cm or more in diameter and are suspected for GIST must be managed with surgical resection.5 In the present case, the patient had a 4‑cm lesion and therefore required surgical removal.
- Ji YK, Jeong ML, Kyung WK, et al. Ectopic pancreas: CT findings with emphasis on differentiation from small gastrointestinal stromal tumor and leiomyoma. Radiology. 2009; 252: 92‑100. | Crossref
- Ginsburg M, Ahmed O, Rana KA, et al. Ectopic pancreas presenting with pancreatitis and a mesenteric mass. J Pediatr Surg. 2013; 48: e29‑e32. | Crossref
- O’Malley RB, Maturen KE, Al‑Hawary MM, Mathur AK. Case of the season: ectopic pancreas. Semin Roentgenol. 2013; 48: 188‑191. | Crossref
- Mulkerrin G, Hogan NM, Sheehan M, Joyce MR. Melena as an unusual presentation of gastrointestinal stromal tumour, a case report. Int J Surg Case Rep. 2018; 44: 172‑175. | Crossref
- Nishida T, Goto O, Raut CP, Yahagi N. Diagnostic and treatment strategy for small gastrointestinal stromal tumors. Cancer. 2016; 122: 3110‑3118. | Crossref
ARTICLE INFORMATION