Primary nonadherence to medication and its drivers in Poland: findings from the electronic prescription pilot analysis
Key words: adherence, big data, electronic prescribing, health services research, pharmacoepidemiology



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Primary nonadherence to medication and its drivers in Poland: findings from the electronic prescription pilot analysis
Introduction: Primary nonadherence to medication occurs when a patient does not fill a prescription and often leads to suboptimal patient outcomes, lost productivity, and increased net costs. Pilot introduction of electronic prescriptions (e‑prescriptions) in Poland took place in 2018, enabling nationwide assessment of primary nonadherence.
Objectives: To determine the prevalence and drivers of primary nonadherence in Poland.
Methods: This retrospective analysis included data from all e‑prescriptions issued in Poland in 2018. Primary nonadherence was defined as not filling a prescription within 1 month from the date of issuing.
Results: Out of all 119 880 e‑prescriptions issued in Poland in 2018, 94 913 were filled, thus the primary nonadherence rate reached 20.8%. Although no differences in primary nonadherence were observed between sexes, age was found to have a significant effect, with older groups showing lower rates of primary nonadherence. In addition, slightly lower rates of primary nonadherence (17.0%) were found for e‑prescriptions issued for selected drugs of key importance (n = 47 492). Multivariable analysis performed within this subset showed that those aged ≥75 years had the lowest odds for nonadherence (odds ratio, 0.55; 95% CI, 0.48–0.64). Differences in primary nonadherence rates were observed across therapeutic areas (lowest value in antibiotics, 14.3%), drug classes (lowest value in sulfonylureas, 13.2%), and individual drugs. Primary nonadherence rates were lower for drugs covered by the “Leki 75+” program, which makes them free of charge for those aged 75 years or older.
Conclusions: A high percentage of prescriptions issued in Poland are never filled. E‑prescriptions allow the identification and analysis of drivers of this phenomenon. Our findings may help designing national health and medicine policies.
What's new?
Medication nonadherence is a major barrier to obtaining full benefits of evidence‑based therapies. On average, 50% of patients on long‑term treatment deviate from the drug regimen. Comparative studies have proved that nonadherence rates might be even higher in Poland. This, however, has been extensively studied for secondary nonadherence, that is, the execution of already started therapies, and there is no data on the rate of primary nonadherence. Objective assessment of primary nonadherence became possible with the introduction of electronic prescriptions. In this study we analyze the big data derived from the electronic prescription pilot in Poland and measure for the first time the primary nonadherence rate and determine the drivers of this phenomenon in the Polish population.
Introduction
The effectiveness of evidence‑based therapies relies on the execution of treatment plans. These plans are typically based around pharmacotherapy. Thus, health outcomes are directly related to adherence to medication.1
According to the ABC European consensus, medication adherence has been defined as active, cooperative, and voluntary adhering of a patient to recommendations from a healthcare provider. It involves 3 critical steps: 1) initiation, which defines the moment that the patient takes the first dose; 2) implementation, which is related to the extent to which the prescription regimen was followed; 3) discontinuation, which happens when the patient stops taking the prescribed medicine(s).2
In general, better adherence entails better health outcomes and improved patient quality of life.3 Moreover, adherence is also one of the major determinants of the costs of health care.4,5 Unfortunately, in real life conditions, adherence is far from expected, particularly in the case of chronic conditions: a World Health Organization report has estimated that adherence to long‑term therapy for chronic illnesses in developed countries averages 50% only.6 Data collected in Poland prove that in terms of poor implementation, nonadherence can range from 57.6% in the case of hypertension7 to 85.6% in the case of psychiatric conditions.8 Comparative studies also indicate that various forms of nonadherence are more prevalent in Poland than in western European countries.7,9
So far, most of the studies in this field have focused on poor implementation and discontinuation.10 However, primary nonadherence is also very important from the public health perspective, due to its negative effect on health outcomes. Moreover, even from a short‑term perspective, initial medication nonadherence has a negative impact on productivity due to lower work ability and leads to increased net costs.11
The Polish healthcare system, like many other European systems, is a health insurance system based on a principle of social solidarity. Health services are provided free of charge to those insured (ie, practically the entire population) by both public and private healthcare providers, and are paid by the only national health payer—the Polish National Health Fund (Narodowy Fundusz Zdrowia). Most of drugs are subject to out‑of‑pocket copayment, which varies within drug classes. Copayment is organized around the idea of stimulating the use of generic drugs: original (brand name) drugs incur higher copayments than generics. However, there is a wide variation in copayment among various generics holding the same active compound. Recently, the “Leki 75+” program has been introduced, allowing those aged 75 and older to obtain several drugs for free in community pharmacies provided that the prescription has been issued by their primary care physician. These are the drugs shortlisted by the Ministry of Health due to their importance in evidence‑based therapy for chronic conditions in the elderly. Currently, the list holds over 2000 drugs.
So far, primary nonadherence has not been extensively studied in Poland due to a lack of relevant data. However, the recent implementation of the uniform nationwide eHealth system in Poland creates a new opportunity for that type of studies, enabling comparisons of data between pharmacy claims and prescriptions. Once completely implemented, this system will be composed of several interlinked digital health solutions, such as electronic prescription (e‑prescription), patient electronic health record, and e‑referral. One of the first solutions to be implemented is e‑prescription, which has been piloted in 2018. Along other major advantages over traditional prescriptions, e‑prescription allows primary nonadherence to be traced through the comparison of data regarding prescribed and dispensed e‑drugs.
Therefore, the aim of this study was to analyze the rate of primary nonadherence in Poland and to identify major drivers of this problem among Polish patients.
Methods
This retrospective analysis used data from all e‑prescriptions issued in Poland in 2018. The entire database included 119 880 e‑prescriptions, each for individual drug item. Most of these prescriptions were issued within the national e‑prescription pilot. The pilot was running from May to September 2018. Participating healthcare institutions of various profiles (such as primary care centers, outpatient specialist clinics, and hospitals) were either invited by CSIOZ (see below), or joined the pilot on the voluntary basis. Thus, the pilot covered 9 provinces (out of 16), and included 190 physicians.
The data used in this study was obtained from the Center of Information Systems for Healthcare (Centrum Systemów Informacyjnych Ochrony Zdrowia, CSIOZ). The CSIOZ is a governmental institution responsible for the digitalization of the Polish healthcare system. One of its major tasks is building up a nationwide system of e‑prescriptions.
The source data was fully anonymized; therefore, according to the policy of Ethical Commission of Medical University of Lodz, the study was not subject to ethical approval.
The data was also simplified: along with basic characteristics of the patient (namely: age and sex), each record included the date of prescription, details (such as a trade name, a dose, a number of packs, etc) of the prescribed drug, date of dispensation (if it took place), and details of the drug being dispensed.
Primary nonadherence is often defined as failure to pick up a medication within a defined number of days after the prescription was made.12 Our data, however, were not linked to clinical data, nor were the longitudinal prescription histories for individual patients available. Therefore, for the purpose of this study, primary nonadherence was defined as the e‑prescription being not dispensed within 30 days, which corresponds with the typical period of prescription validity in Poland.
In order to perform an in‑depth analysis of the drivers of nonadherence, 47 drugs of key importance for public health were selected. These belonged to 6 major therapeutic areas and were derived from 16 drug classes, as detailed below, along with their corresponding Anatomical Therapeutic Chemical (ATC) codes:
-
Diabetes
-
Biguanides: metformin (A10BA02)
-
Sulfonylureas: gliclazide (A10BB09), glimepiride (A10BB12)
-
α-Glucosidase inhibitors: acarbose (A10BF01)
-
Dipeptidyl peptidase 4 inhibitors: sitagliptin (A10BH01)
-
-
Antithrombotic agents
-
Vitamin K antagonists (VKAs): warfarin (B01AA03), acenocoumarol (B01AA07)
-
Platelet aggregation inhibitors: clopidogrel (B01AC04)
-
Novel oral anticoagulants: dabigatran (B01AE07), rivaroxaban (B01AF01)
-
-
Cardiovascular system
-
Diuretics: hydrochlorothiazide (C03AA03), indapamide (C03BA11), furosemide (C03CA01), torasemide (C03CA04), spironolactone (C03DA01), eplerenone (C03DA04)
-
β-Blockers: metoprolol (C07AB02), bisoprolol (C07AB07), nebivolol (C07AB12), carvedilol (C07AG02)
-
Calcium channel blockers: amlodipine (C08CA01), lacidipine (C08CA09), diltiazem (C08DB01)
-
Angiotensin‑converting enzyme (ACE) inhibitors: enalapril (C09AA02), perindopril (C09AA04), ramipril (C09AA05), quinapril (C09AA06)
-
Angiotensin II receptor blockers: losartan (C09CA01), valsartan (C09CA03)
-
-
Lipid modifying agents
-
HMG CoA reductase inhibitors: simvastatin (C10AA01), atorvastatin (C10AA05), rosuvastatin (C10AA07)
-
Fibrates: fenofibrate (C10AB05)
-
-
Anti‑infectives for systemic use
-
Antibacterials for systemic use: doxycycline (J01AA02), amoxicillin (J01CA04), amoxicillin and β-lactamase inhibitor (J01CR02), cefuroxime (J01DC02), roxithromycin (J01FA06), azithromycin (J01FA10), clindamycin (J01FF01), ciprofloxacin (J01MA02)
-
-
Psychoanaleptics
-
Antidepressants: opipramol (N06AA05), fluoxetine (N06AB03), paroxetine (N06AB05), sertraline (N06AB06), escitalopram (N06AB10), venlafaxine (N06AX16).
-
For further analysis, ATC classification system codes were assigned according to the drug trade names originally provided on the e‑prescriptions. Thus, different drugs sharing the same chemical compound were classified under the same ATC code. Only drugs formed from a single chemical compound were included in this analysis, fixed‑dose combination drugs were excluded.
Statistical analysis
Data analysis included descriptive statistics of overall prevalence of primary nonadherence. Then, the effect of potential drivers of primary nonadherence was assessed, these included patient characteristics (age and sex), drug class, and special care program (the “Leki 75+” program). For the purpose of this analysis, age (a continuous variable) was categorized into 5 categories: 1 to 18 years, 19 to 39 years, 40 to 64 years, 65 to 74 years, and 75 years or older. Due to a low number of patients in the 2 youngest age groups, for the purpose of logistic regression analysis, these 2 groups were combined. Categorical variables were expressed as proportions and compared between relevant groups using the χ2 test.
In addition to the descriptive analyses, multivariable analysis was performed with age and sex accepted as independent variables, and primary nonadherence as a single dependent variable. In order to determine which of these factors, if any, were independently associated with primary nonadherence in our study population, a logistic regression was employed. This allowed the calculation of relevant odds ratios and 95% CI. For statistical calculations, Statistica 10 software (TIBCO Software Inc.) was used. A P value of less than 0.05 was considered significan
Results
Electronic prescription characteristics
Out of all 119 880 e‑prescriptions issued in Poland in 2018, nearly three fourth (72 149, 60.2%) were prescribed to women. Only 806 e‑prescriptions (0.7% of all) were prescribed to those aged up to 18 years, whereas the highest number of e‑prescriptions was issued for the 40‑to‑64‑years age group (40 742, 34.0%). Altogether, prescriptions for the elderly, that is, those aged 65 years or older, represented 57.3% (68 692) of the total number of e‑prescriptions; of these, nearly half were issued for those aged 75 years or older (Table 1).
Variable | Electronic prescription status | P value | ||
Filled (adherence) | Not filled (nonadherence) | All | ||
Data are presented as number (percentage). | ||||
Sex | ||||
Female | 57 120 (79.17) | 15 029 (20.83) | 72 149 (100) | 0.96 |
Male | 37 793 (79.18) | 9938 (20.82) | 47 731 (100) | |
Age group | ||||
1–18 y | 508 (63.03) | 298 (36.97) | 806 (100) | <0.001 |
19–39 y | 6290 (62.25) | 3350 (34.75) | 9640 (100) | |
40–64 y | 31 647 (77.68) | 9095 (22.32) | 40 742 (100) | |
65–74 y | 30 223 (80.76) | 7198 (19.24) | 37 421 (100) | |
≥75 y | 26 245 (83.93) | 5026 (16.07) | 31 271 (100) | |
Total | 94 913 (79.17) | 24 967 (20.83) | 119 880 (100) | – |
Primary nonadherence
Out of all e‑prescriptions issued in Poland in 2018, 94 913 were filled in, thus the rate of primary nonadherence was 20.8% (Table 1).
Across all e‑prescriptions, identical percentages were unfilled in the case of e‑prescriptions issued for women and men (20.8% and 20.8%; P = 0.97). On the other hand, age had an effect on primary nonadherence, with the lowest rate of nonadherence found in e‑prescriptions issued for the oldest group (36.9% of e‑prescriptions unfilled in those aged 1–18 years vs 16.1% in those aged ≥75 years; P <0.001) (Table 1).
Primary nonadherence in the subgroup of drugs of key importance
For the group of selected drugs of key importance, 47 492 e‑prescriptions were issued, of which 27 826 (58.6%) were prescribed to women. In this sample, the primary nonadherence rate reached 17.0% (Table 2).
Therapeutic area | Drug class | Drug name | E‑prescriptions issued, n | Primary nonadherence, % |
Abbreviations: ACE, angiotensin‑converting enzyme; e‑prescription, electronic prescription; HMG‑CoA, 3‑Hydroxy‑3‑methylglutaryl–coenzyme A | ||||
Diabetes | Total | 4878 | 14.90 | |
Biguanides | Metformin | 417 | 15.42 | |
Sulfonylureas | Total | 1322 | 13.24 | |
Gliclazide | 726 | 10.33 | ||
Glimepiride | 596 | 16.78 | ||
α-Glucosidase inhibitors | Acarbose | 123 | 17.89 | |
Dipeptidyl peptidase 4 inhibitors | Sitagliptin | 16 | 18.75 | |
Antithrombotic agents | Total | 1918 | 18.09 | |
Vitamin K antagonists | Total | 375 | 15.73 | |
Warfarin | 185 | 15.68 | ||
Acenocoumarol | 190 | 15.79 | ||
Platelet aggregation inhibitors | Clopidogrel | 395 | 14.18 | |
Novel oral anticoagulants | Total | 1148 | 20.21 | |
Dabigatran | 328 | 29.27 | ||
Rivaroxaban | 820 | 16.59 | ||
Cardiovascular system | Total | 27 634 | 17.19 | |
Diuretics | Total | 7132 | 18.55 | |
Hydrochlorothiazide | 71 | 18.31 | ||
Indapamide | 2960 | 16.89 | ||
Furosemide | 795 | 14.21 | ||
Torasemide | 2233 | 21.67 | ||
Spironolactone | 494 | 16.40 | ||
Eplerenone | 579 | 22.80 | ||
β-Blockers | Total | 10 747 | 17.14 | |
Metoprolol | 2214 | 16.31 | ||
Bisoprolol | 4556 | 17.80 | ||
Nebivolol | 3382 | 17.53 | ||
Carvedilol | 595 | 12.94 | ||
Calcium channel blockers | Total | 2837 | 17.98 | |
Amlodipine | 2318 | 18.94 | ||
Lacidipine | 449 | 15.14 | ||
Diltiazem | 70 | 4.29 | ||
ACE inhibitors | Total | 5503 | 15.10 | |
Enalapril | 269 | 15.61 | ||
Perindopril | 1089 | 15.79 | ||
Ramipril | 4003 | 14.91 | ||
Quinapril | 142 | 14.08 | ||
Angiotensin II receptor blockers | Total | 1415 | 17.17 | |
Losartan | 362 | 18.51 | ||
Valsartan | 1053 | 16.71 | ||
Lipid‑modifying agents | Total | 9281 | 17.91 | |
HMG‑CoA reductase inhibitors | Total | 7962 | 17.51 | |
Simvastatin | 1284 | 14.25 | ||
Atorvastatin | 3137 | 18.90 | ||
Rosuvastatin | 3541 | 17.45 | ||
Fibrates | Fenofibrate | 1319 | 20.32 | |
Anti‑infectives for systemic use | Antibacterials for systemic use | Total | 2747 | 14.27 |
Doxycycline | 126 | 15.87 | ||
Amoxicillin | 733 | 14.73 | ||
Amoxicillin and β-lactamase inhibitor | 627 | 12.44 | ||
Cefuroxime | 525 | 11.62 | ||
Roxithromycin | 5 | 0.00 | ||
Azithromycin | 423 | 17.02 | ||
Clindamycin | 103 | 17.48 | ||
Ciprofloxacin | 205 | 17.07 | ||
Psychoanaleptics | Antidepressants | Total | 1034 | 17.79 |
Opipramol | 420 | 16.90 | ||
Fluoxetine | 68 | 14.71 | ||
Paroxetine | 128 | 12.50 | ||
Sertraline | 222 | 18.02 | ||
Escitalopram | 125 | 22.40 | ||
Venlafaxine | 71 | 26.76 | ||
Total | 47 492 | 16.97 | ||
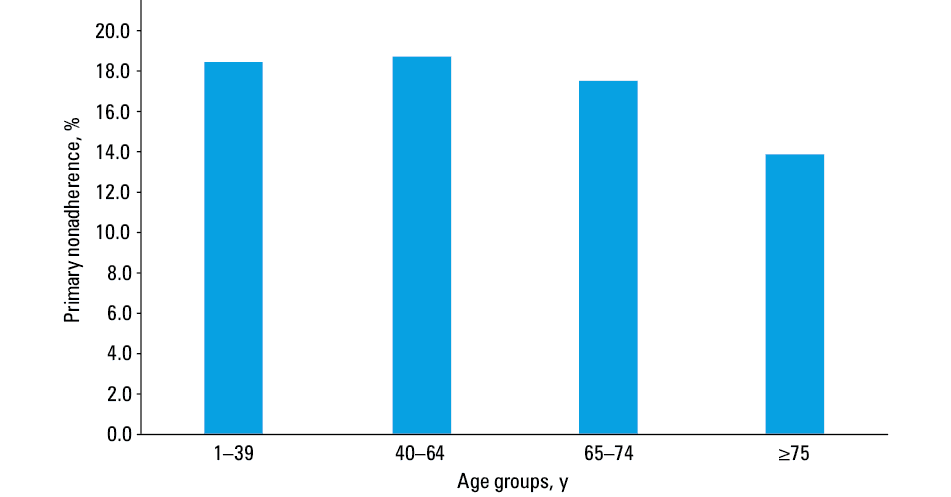
The univariable analysis found sex to have no effect on primary nonadherence in the selected drug sample, with primary nonadherence occurring in 16.8% of e‑prescriptions issued to women, and 17.3% to men (P = 0.13). Also in this sample, primary nonadherence was found to correlate with age, with the lowest rate of primary nonadherence observed in patients aged 75 years or older (Figure 1). Multivariable analysis confirmed that the odds for nonadherence decreased with age, with the lowest odds ratio of 1.81 (95% CI, 1.57–2.09) in those aged 75 years or older (Table 3).
Variable | OR (95% CI) | P value |
Abbreviations: OR, odds ratio | ||
Sex | ||
Male | Reference | |
Female | 0.96 (0.86–1.08) | 0.53 |
Age | ||
1–39 y | Reference | |
40–64 y | 0.77 (0.67–0.89) | <0.001 |
65–74 y | 0.73 (0.63–0.84) | <0.001 |
≥75 y | 0.55 (0.48–0.64) | <0.001 |
Variability in nonadherence was observed across therapeutic areas, drug classes, and individual drugs (Table 2). Out of the therapeutic areas, the lowest rate of dispensation failure was observed in antibiotics (14.3%), followed by antidiabetic agents (14.9%); the highest rates were observed for antithrombotic agents, lipid lowering agents, and antidepressants (18.1%, 17.9%, and 17.8%, respectively). Among drug classes, the lowest rates of primary nonadherence were observed for sulfonylureas and platelet aggregation inhibitors (13.2% and 14.2%, respectively), and the highest for fibrates and novel oral anticoagulants (20.3% and 20.2%, respectively). Finally, with regard to individual drugs, the lowest rates of primary nonadherence were observed with roxithromycin, diltiazem, and gliclazide (0.0%, 4.3%, and 10.3%, respectively) and the highest with dabigatran, venlafaxine, and eplerenone (29.3%, 26.8% and 22.8%) (Figure 2). However, it is important to note that only a limited number of e‑prescriptions were issued for both roxithromycin and diltiazem.
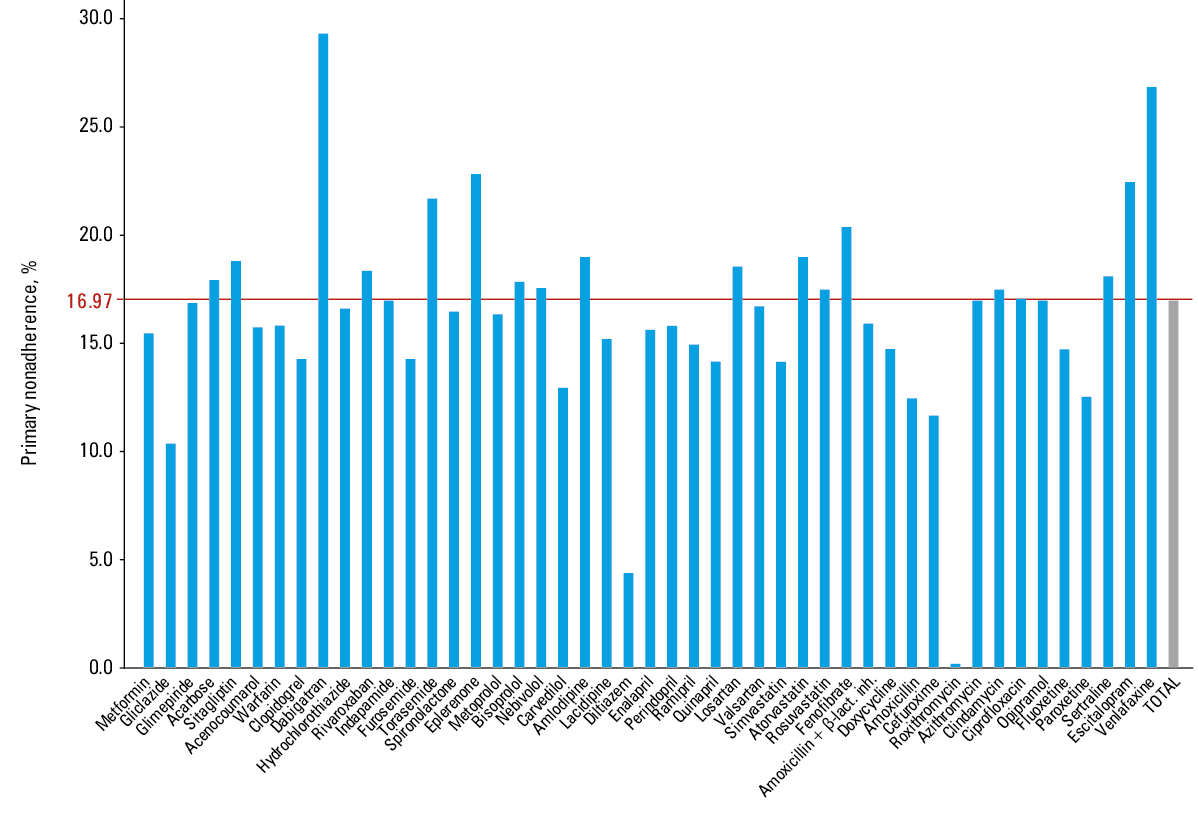
Abbreviations: β-lact. inh., β-lactamase inhibitor
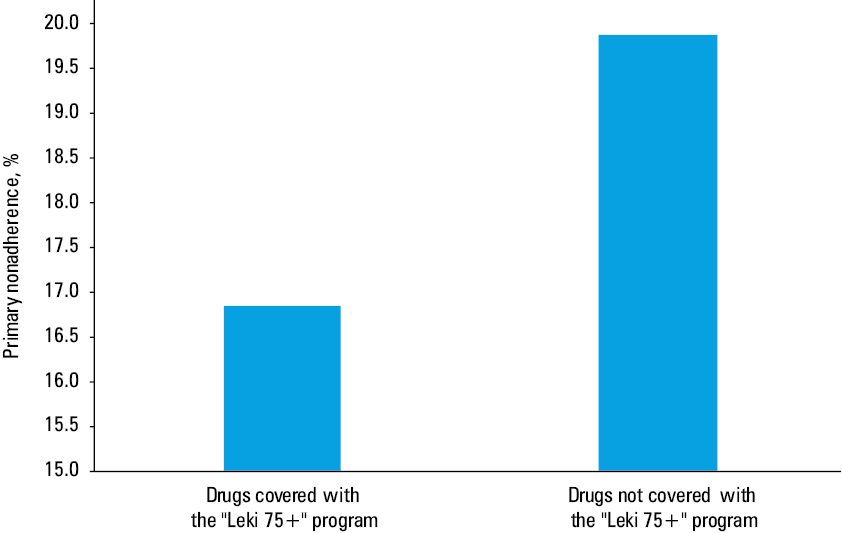
Several drugs belonging to the sample were covered by the “Leki 75+” program. As illustrated in Figure 3, prescriptions for drugs covered by this program were unfilled less often than the drugs that were not included in the program (16.9% vs 19.9%, respectively; P <0.001).
Discussion
This study is the first large‑scale assessment of primary nonadherence in Poland. Our results clearly indicate that a substantial proportion of issued e‑prescriptions, that is, 1 out of 5, was not collected. However, this Figure merits some further justification. Some of the uncollected e‑prescriptions were issued for items of lower importance, such as over‑the‑counter drugs available in pharmacies, dietary supplements, or even cosmetics. Despite this, the percentage of unfulfilled e‑prescriptions issued for selected drugs of major importance is of more concern. Although the rate of primary nonadherence in this sample was still high (17.0%), it is comparable to such values found in other countries, ranging from 6.3% for statins and 8.0% for antidepressants in Iceland,13 through 5.6% for oral anticoagulation drugs in Spain,14 9.3% for all drugs in Denmark,15 13.1% for drugs used in osteoporosis in Estonia,16 14.9% for antidepressants in Sweden,17 to 15% for antidepressants in Catalonia.18 In a small study in Portugal, primary nonadherence reached 22.8%.19 Perhaps the largest European cohort studied so far, that is, approximately 1.6 million Catalonian patients with 2.9 million prescriptions, indicated 17.6% primary nonadherence for all drug classes20
Despite dissimilarities between European and American healthcare systems, comparable results were obtained in several analyses performed in the United States. It has been found that 15.4% of patients prescribed statins in managed care organization settings did not collect their prescriptions within 90 days of the order date.21 In addition, 29.5% of women aged 55 years and older in integrated healthcare settings in California did not collect their bisphosphonate prescription within 60 days of the order date.22 Furthermore, 34% of patients prescribed treatment for hypertension did not fulfil their prescription within 30 days,23 and only 78% of all prescriptions issued in pediatric primary care were collected.24 Finally, among older adults consecutively discharged from a general internal medicine service at a large urban teaching hospital in Canada, 28% exhibited primary nonadherence at 7 days after discharge, and 24% at 30 days after discharge.25
Hence, the rate of primary nonadherence observed in the first year of e‑prescription use in Poland did not deviate from those observed in other countries. Interestingly, 22.5% of all 195 930 e‑prescriptions issued within the first year of a community‑based e‑prescription initiative in Massachusetts were not filled.26
Another interesting finding of our study is the effect of age on primary nonadherence rates. Contrary to our expectations, the older age group tended to display a lower percentage of unfilled e‑prescriptions, with the lowest values observed in those aged 75 years or older (16.1% in the general population and 13.9% in a sample of selected drugs of key importance for chronic treatment). Similar observations have been made in other studies, across conditions and locations in Europe and the United States.17,21,26 While it is possible that this greater compliance might be related to a greater motivation felt by seniors to take care of their health, adherence may also be affected by the presence of a carer, as some seniors are less independent in managing their own medication. However, further studies are needed to more precisely identify the determinants of lower rates of primary nonadherence in this age group.
Of utmost importance is our observation that primary nonadherence varied across therapeutic areas, drug classes, and individual drugs. This has also been found to be the case in other studies.15,26-28
Not surprisingly, out of the studied therapeutic areas, primary nonadherence was the lowest for antibiotics (14.3%). This most likely is associated with the symptomatic nature of the infections treated with these antibacterials. Other studies have provided similar findings.24
Among cardiovascular agents, the lowest primary nonadherence was found for ACE inhibitors (15.1%); this compares to 17.1% for β-blockers, 17.2% for angiotensin II receptor blockers, 18.0% for calcium channel blockers, and 18.6% for diuretics. Interestingly, similar findings have been found in other countries: in one study of patients treated for newly diagnosed heart failure, the greatest rate of compliance was observed for β-blockers, followed by ACE inhibitors.29 In another study based on a large database of Catalonian e‑prescriptions, the lowest rate of primary nonadherence across all assessed drug classes was observed for ACE inhibitors.20 Perhaps one of the key drivers of this phenomenon is a very low level of adverse effects in the case of ACE inhibitors, and the contrary in the case of diuretics.
Several of our findings suggest that drug affordability may influence the rate of primary nonadherence. Firstly, primary nonadherence being generally low for drugs used in diabetic patients (14.9%), differed across individual drugs. It is not surprising as some of these drugs are very affordable, being subject to only minimal patient copayment in Poland (approximately 3.00 PLN, ie, 0.70 EUR). In contrast, sitagliptin, incurring out‑of‑pocket patient copayment of approximately 140.00 PLN (approximately 33.00 EUR) due to a lack of reimbursement, was associated with much higher rates of primary nonadherence (18.8%).
Similar scenario was observed in the case of antithrombotic agents, in which primary nonadherence ranged from 15.7% for VKAs to 20.2% for the more expensive novel oral anticoagulants. Very similar results have been observed in Spain, with OR of 2.76 (95% CI, 2.41–3.15) for primary nonadherence in the case of NOACs as compared with VKAs.14 Despite having a more patient‑friendly profile with no need for laboratory monitoring or subsequent dose adjustment, NOACs are a much more costly than VKAs. In Poland, this corresponds with much higher patient copayment. Recent study in patients with atrial fibrillation in Poland found a high rate of nonadherence for dabigatran.30 Interestingly, in our study, we observed the highest rate of primary nonadherence in the case of dabigatran.
Finally, the free availability of selected drugs for the oldest patients within the “Leki 75+” program also appears to have a beneficial effect on compliance. Indeed, a higher drug cost have often been found to be the driver of primary nonadherence.13 This was studied in more detail in an analysis performed in Catalonia, where the introduction of a fixed copayment was followed by a significant increase in primary nonadherence among the poorer population, low/middle‑income pensioners, and low‑income nonpensioners (OR, 1.047–1.370), as well as a large but insignificant increase among the high‑income populations. Primary nonadherence decreased again in the low‑income population after suspension of the fixed copayment and the introduction of a coinsurance policy that granted this population free access to medication (OR, 0.676).31 Out of all drivers of primary nonadherence, pharmacy copayments or out‑of‑pocket medication expenses represented the strongest association with poor initial adherence in terms of effect size or ORs in a systematic literature review.28
The present study has certain limitations. Although the analysis of the e‑prescription database allows for the identification of primary nonadherence in an objective, unbiased way, it does not provide any information on why a patient has not filled a prescription. Many such reasons are possible, from lack of trust in a diagnosis or a physician, the type of drug formulation, to high out‑of‑pocket costs: in Poland, patients are obliged to participate in the drug costs, which vary according to the drug, indication, patient characteristics, and so on.32 In addition, it was not possible to identify individual patients based on the data processed. Therefore, it was not possible to present initial nonadherence by the number of patients, nor to determine whether a particular e‑prescription was the first for a particular patient or whether it occurred later in a series. For the same reasons, it was not possible to compare the rate of primary nonadherence to different drugs prescribed to a patient at the same time, and assess supposed prioritization. Finally, most of the analyzed e‑prescriptions were issued within the course of the national e‑prescription system pilot. The pilot run in selected locations only, which could lead to certain inclusion bias. Similarly, arrangements of this pilot could differ from usual care conditions to some extent. Nevertheless, we believe that all these limitations do not undermine the usefulness of our study, which is unique for Poland both in terms of database size and the accuracy of the used data.
Conclusions
Our findings highlight the problem of primary nonadherence in Poland and identify several drivers of this phenomenon. Primary nonadherence varies across therapeutic areas, drug classes, and individual medicines. It is the least prevalent in the oldest patients. Drug affordability seems to be an important driver of this variation: prescriptions for drugs covered by the “Leki 75+” program, which grants seniors free access to selected drugs for chronic conditions, are collected much more often than those outside the program.
The study proves that an e‑prescription system, an innovative e‑health solution currently implemented in Poland, provides unique opportunity to study primary nonadherence. Further studies combining e‑prescription data with clinical data, both at the individual and national level, could shed even more light on this matter. The chances for this may come with the implementation of a nationwide e‑prescription system, which has started on January 8, 2020. Nevertheless, our present findings offer practical recommendations for the Polish public health and can play a significant role in designing a national health policy.
- Marcum ZA, Hanlon JT, Murray MD. Improving medication adherence and health outcomes in older adults: an evidence‑based review of randomized controlled trials. Drugs Aging. 2017; 34: 191‑201. | Crossref
- Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012; 73: 691‑705. | Crossref
- Alfian SD, Sukandar H, Lestari K, Abdulah R. Medication adherence contributes to an improved quality of life in type 2 diabetes mellitus patients: a cross‑sectional study. Diabetes Ther. 2016; 7: 755‑764. | Crossref
- Cutler RL, Fernandez‑Llimos F, Frommer M, et al. Economic impact of medication nonadherence by disease groups: a systematic review. BMJ Open. 2018 21; 8: e016982. | Crossref
- Muszbek N, Brixner D, Benedict A, et al. The economic consequences of noncompliance in cardiovascular disease and related conditions: a literature review. Int J Clin Pract. 2008; 62: 338‑351. | Crossref
ARTICLE INFORMATION