Recent advances in the workup and management of Raynaud phenomenon
Key words: capillaroscopy, Raynaud phenomenon, therapy, thermography, ultrasonography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Recent advances in the workup and management of Raynaud phenomenon
Raynaud phenomenon (RP) is defined as recurrent, reversible episodes of vasospasm involving peripheral small vessels, typically in the fingers and toes. Primary (idiopathic) RP is common (it occurrs in about 5% of the general population) and is usually benign. Secondary RP accounts for 10% to 20% of all RP cases and may be associated with complications such as tissue loss, ulcers, and gangrene. Systemic sclerosis (SSc) or, more rarely, other connective tissue diseases are the main underlying conditions. A detailed clinical history and careful physical examination may be helpful in identifying the cause. Routine investigations include a full blood count, measurement of erythrocyte sedimentation rate, C‑reactive protein, antinuclear antibody levels, biochemical profile, thyroid function tests, protein electrophoresis, chest X‑ray, and nailfold capillaroscopy. Capillaroscopy can facilitate a very early diagnosis of SSc. Doppler ultrasound is recommended to evaluate the risk of pathologies in large to medium–sized arteries. Lifestyle modifications may be sufficient to control primary RP, but some patients, and most with secondary RP, require pharmacologic treatment. Several medications are proposed to manage RP and its complications, such as calcium channel blockers, phosphodiesterase type 5 inhibitors, intravenous prostanoids, and topical nitrates. However, scientific evidence for the use of these drugs is still weak to moderate. Despite the lack of efficacy of bosentan in RP treatment, this medication is approved for the secondary prevention of digital ulcers in patients with SSc. In conclusion, the management of RP still represents a challenge. Collaboration between healthcare professionals, patient organizations, and the society could encourage earlier medical assessment of people at risk of SSc.
Introduction
Raynaud phenomenon (RP) is defined as recurrent, reversible episodes of vasospasm involving peripheral small vessels of the fingers and toes, at times also of the other acral sites (nose, ears, oral mucosa, lips, or nipples), when exposed to a cold environment or stressful situation.1 This is characterized by a series of color changes in the affected area: first white (lack of blood flow), then bluish (deoxygenation of remaining blood), and red (reperfusion). Attacks can cause distal pain, burning, numbness, and paresthesia.2 Regarding its etiology, RP is classified as primary (idiopathic) or secondary. Primary RP, which is an isolated finding without an underlying pathology, is common, occurring in about 5% of the general population living in areas with cold climates.3 The prevalence of RP is higher in women (female‑to‑male ratio of 9 to 1). There is an associated genetic predisposition: one polymorphic variant was identified within the nitric oxide synthase 1 gene as significantly correlated with RP in the general population.4 Major risk factors for primary RP include, in addition to the female sex and family history, a previous sensation of cold hands, migraine, cardiovascular diseases, decreased body mass index, manual occupation (not including vibration tool use), and estrogen replacement therapy.3-6 Cigarette smoking and alcohol consumption are still of unclear significance when concerning the prevalence of primary RP.7
Secondary RP associated with a known disease, mainly with systemic sclerosis (SSc) (>80% of patients) or other connective tissue diseases (CTDs), is rare and accounts for 10% to 20% of all RP cases.8 Other common causes of secondary RP include diseases of arteries in the upper limbs (60% of RP occurring in individuals older than 60 years), malignancies, endocrine diseases, occupational syndromes, hematologic disorders, and infections (Table 1).8,9 In addition, several medications, such as antimigraine drugs (ergot alkaloids), nonselective β-blockers, clonidine, psychostimulants (cocaine, amphetamine, methylphenidate), atomoxetine, risperidone, and aripiprazole are known to induce secondary RP.10,11 Interferons, ribavirin, cyclosporine, chemotherapies (bleomycin, vinca alkaloids, gemcitabine, and cisplatin), and selective serotonin reuptake inhibitors (insufficient scientific evidence to be recommended in the treatment of RP) were also reported to be related with RP.12 Furthermore, a recent analysis in the World Health Organization pharmacovigilance database VigiBase revealed a possible risk of RP with the use of proton pump inhibitors.13 Additionally, even though there are no descriptions in the literature, unexpected RP was reported to be associated with exposure to drugs (hepatitis B vaccine, isotretinoin, leflunomide, hydroxycarbamide, rofecoxib, telmisartan, and zolmitriptan).14
Obstructive vascular diseases | Atherosclerosis, microemboli, diabetic angiopathy, thromboangiitis obliterans (Buerger disease) |
Malignancies | Adenocarcinomas (lung, breast, ovarian), hematologic malignancies |
Endocrine diseases | Hypo- and hyperthyroidism, carcinoid syndrome, pheochromocytoma |
Hematologic disorders | Cryofibrinogenemia, cold agglutinin disease, paraproteinemia, multiple myeloma, polycythemia, microthromboembolism |
Infections | Parvovirus B19, cytomegalovirus, hepatitis B and C viruses, Helicobacter pylori, mycoplasma |
Mechanical factors | Crutch pressure, thoracic outlet syndrome, scalenus anticus syndrome, cervical rib, carpal tunnel syndrome |
Occupational and environmental exposure | Vibration (white hand vibration syndrome), trauma to the upper extremities (hypothenar or thenar hammer syndrome), frostbite, vinyl chloride monomer, chlorinated and nonchlorinated solvents (acetone, toluene, xylene, etc) |
The pathophysiology of RP is complex and only partially known. Mechanisms for RP include augmented activity of postsynaptic α2‑adrenergic receptors and closing of both arteriovenous anastomoses and finger arterioles.15 Secondary RP in SSc underlies a microvasculopathy and an abnormal function of the endothelium, leading to an imbalance of vasoactive factors including, among others, the overproduction of the vasoconstrictor endothelin 1 (ET‑1) and underproduction of the vasodilator nitric oxide and prostacyclin.16
Primary RP has an earlier onset (median age at onset is around 14 years) and is characterized by milder symptoms.17 Secondary RP often has a later onset (usually after the age of 40, rare in children) with more severe symptoms, which leads to complications such as digital ulcers, finger necrosis, and amputation or associated infection and osteomyelitis.17 Early detection of SSc or any other cause of secondary RP could allow early treatment and better patient outcomes.
The aim of this review was to clarify and provide update on the workup and management of RP based on the published data from the past 4 years. The MEDLINE database was searched for primary and secondary sources related to the topic, using the term “Raynaud’s phenomenon.”
Aspects of differential diagnosis
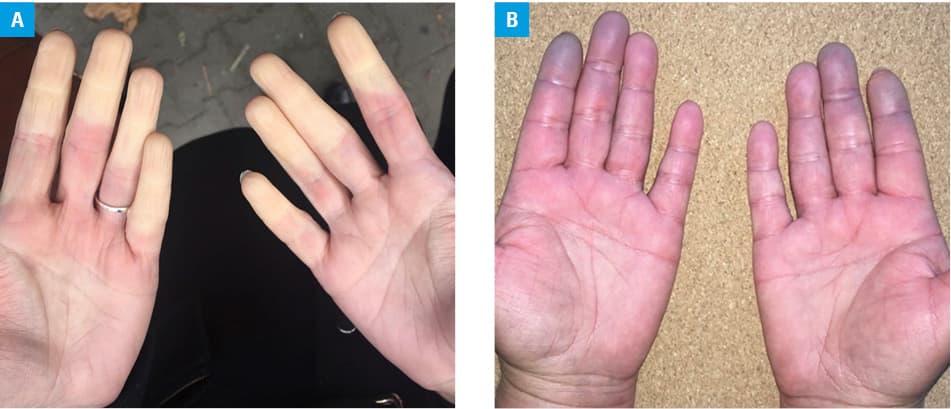
The triphasic or biphasic color changes are required to make the diagnosis of RP.18 White(pallor) and blue(cyanosis) are the 2 most important colors (Figure 1A and 1B).18 Patients must report cold temperatures as one of the triggers for their RP attacks.18 In contrast, blue or purple finger syndromes present with no changes in color when subject to temperature changes.19 Triggers other than cold (eg, emotional stress), standardized questionnaires, photographs of episodes provided by patients, bilateral hand involvement even if asynchronous and asymmetrical, history of attacks at sites other than the hands, well demarcated color changes, numbness, and paresthesia are deemed helpful but not required to diagnose RP.18 Clinical recognition of the functional vascular acrosyndromes, such as erythromelalgia, acrocyanosis, and chilblains, helps avoid an unnecessary investigation, although these disorders may coexist with RP.20 To evaluate for large‑vessel occlusive arterial disease, peripheral pulse examination (palpation of the subclavian, brachial, radial, and ulnar arteries), the Allen test and segmental blood pressure measurements in the upper extremity can be performed.
Laboratory examinations
All patients presenting with RP should undergo blood tests including full blood count, measurement of erythrocyte sedimentation rate or serum C‑reactive protein levels, and antinuclear antibody (ANA) testing.21 It is known that the presence of SSc‑associated antibodies (anticentromere, anti‑topoisomerase I, or anti‑RNA polymerase III) and abnormal nailfold capillaries at baseline increases the likelihood of developing definite SSc, whereas their absence at baseline practically excludes this outcome.22 Positivity for ANAs is also an important predictive factor for the evolution to CTD other than SSc.22 In particular, most of the transitions to CTD were toward undifferentiated CTD and systemic lupus erythematosus.22 The routine investigations should also comprise a biochemical profile, thyroid function tests, protein electrophoresis, and chest radiography.23
Evaluation of the microcirculation
Capillaroscopy
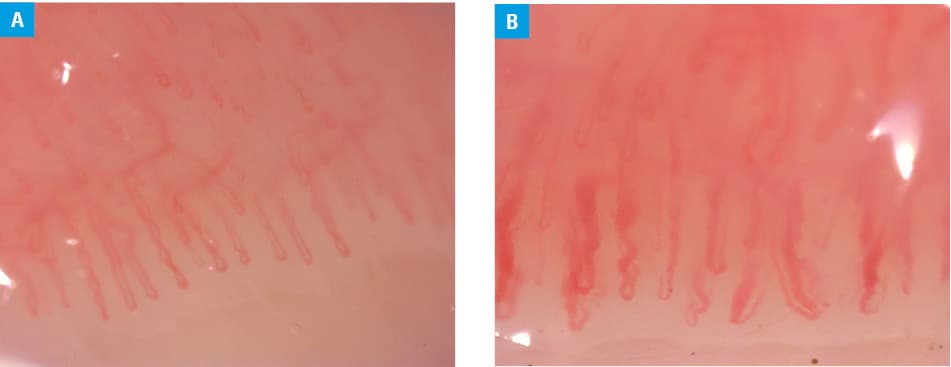
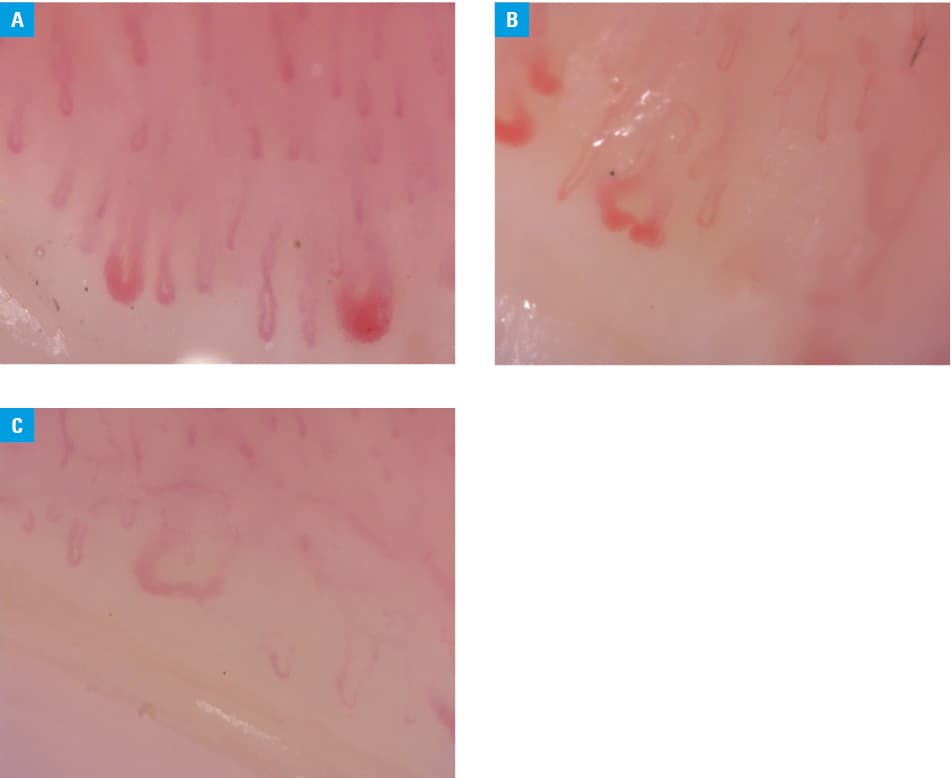
Capillaroscopy is used to analyze in vivo images of skin microcirculation in the nailfold bed of the second to fifth fingers of each hand. This method detects and quantifies the microvascular changes that characterize secondary RP associated with SSc or scleroderma spectrum disorders.24 The main parameters that are assessed on capillaroscopic examination are as follows: shape of capillaries, distribution, mean diameter of the arterial limb, mean diameter of the venous limb, mean capillary length, mean capillary density (normal range, 7–12 capillaries/mm), visibility of the subpapillary plexus, and presence of abnormalities such as capillary tortuosity, dilated (capillary limb >20 μm) or giant (capillary limb >50 μm) capillaries, elongated or short capillaries, hemorrhages, avascular areas, and neoangiogenic capillaries.24 International multicenter studies demonstrated that the reliability of the simple capillaroscopic definition of normal and abnormal morphologies of capillaries was excellent, even when used by clinicians with varying levels of expertise in capillaroscopy (Figure 2A and 2B).25,26 The presence of giant capillaries and microhemorrhages and the number of capillaries have a significant prognostic value for predicting SSc or a scleroderma spectrum disorder.24 Furthermore, capillaroscopy identifies morphological patterns specific to various SSc microangiopathy stages and is now included in the diagnostic criteria for primary RP, in the criteria for very early diagnosis of SSc (VEDOSS), and in the American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria for SSc.24 The early pattern is characterized by the presence of a few enlarged and giant capillaries and no evident loss of capillaries, with a well‑preserved capillary distribution (Figure 3A).24 In the active pattern, there are frequent giant capillaries and microhemorrhages, as well as a moderate loss of capillaries with mild disorganization of the capillary architecture (Figure 3B).24 Typical characteristics in the late pattern include a severe loss of capillaries with extensive avascular areas and disorganization of the normal capillary array, associated with no giant capillaries and microhemorrhages, as well as the presence of abnormal capillaries (Figure 3C).24 The presence of active and late patterns on capillaroscopy was associated with a 30‑fold increased risk of definite SSc over a 3‑year follow‑up.27
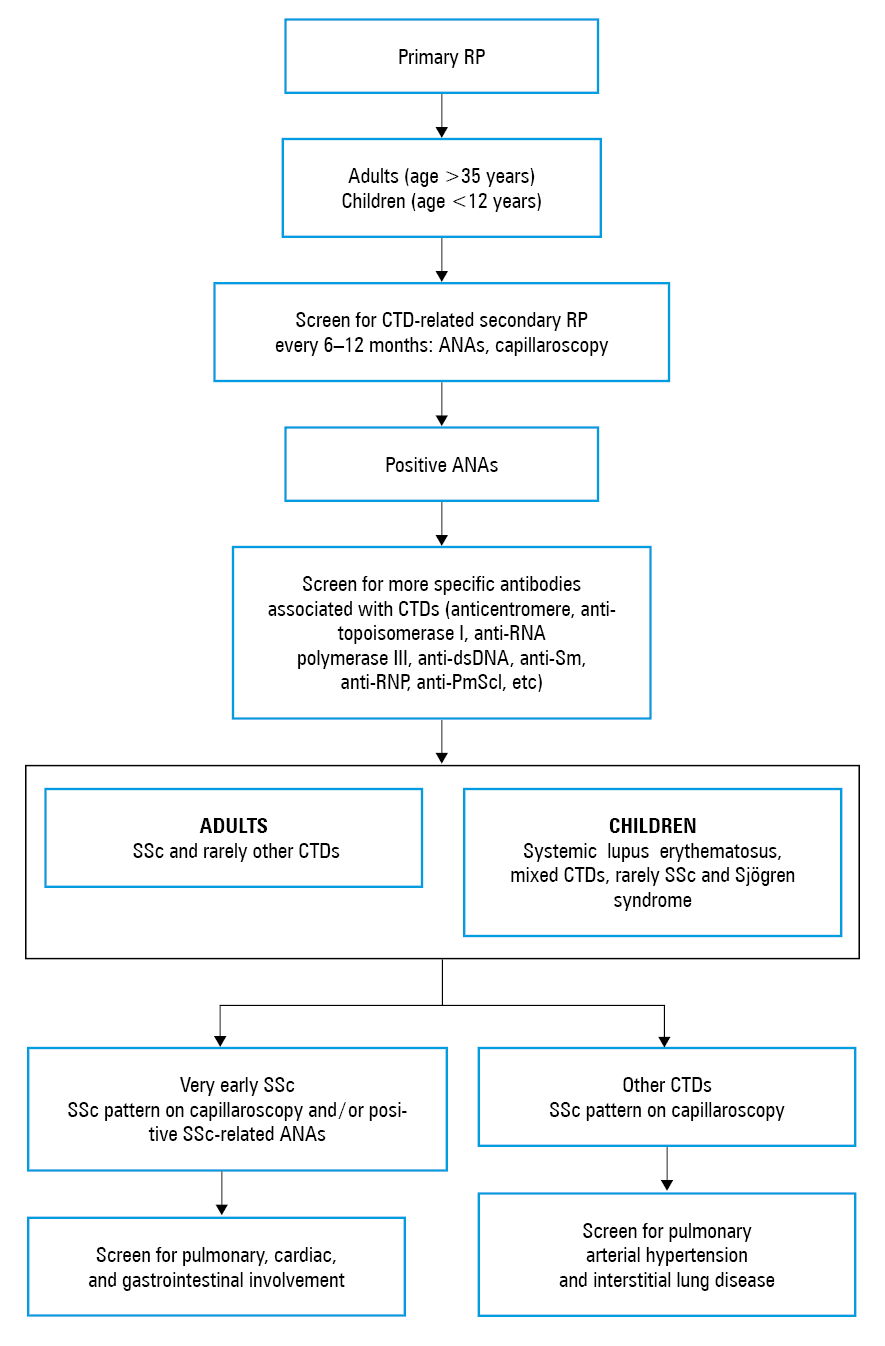
Patients with primary RP with nonspecific nailfold capillary alterations (dilations of a capillary diameter of 20 µm to 50 µm at the level of the arterial branch, microhemorrhages, and a reduction of capillary number <7) at the first capillaroscopic evaluation should be closely monitored at least every 6 months, as they run a higher risk of transition to secondary RP.28 The pattern of SSc on capillaroscopy can facilitate very early diagnosis of SSc and scleroderma spectrum disorders as well as their sequelae in patients with RP.29 A correlation between capillaroscopic findings (capillary loss and severe deformity) and the presence of interstitial lung disease in patients with SSc was observed.29 Pulmonary, cardiac, and gastrointestinal involvement may be present at the very early stage of SSc and must be screened.29 A higher prevalence of abnormal pulmonary function tests was also revealed in patients with primary Sjögren syndrome, systemic lupus erythematosus, and mixed CTDs.30-33 Therefore, it is proposed to screen for pulmonary arterial hypertension and interstitial lung disease in all RP patients with CTD.
The high intra- and interrater reliability suggests that an overall image grade, capillary density (vessels/mm), and mean vessel apical width have a potential as outcome measures in longitudinal studies.34 Few papers reported a semiautomated or fully automated methods for the quantitative assessment of the absolute nailfold capillary number on capillaroscopy images.35 Capillary density is the most reliable capillaroscopic parameter for predicting SSc progression and detecting therapy outcomes.35 This parameter was used for the construction of several scoring systems, such as the capillaroscopic skin ulcer risk index (CSURI), the microangiopathy evolution score, and the simple day‑to‑day risk.36,37
Capillaroscopy should only be carried out using equipment of good optical quality and by an experienced operator, usually in secondary or tertiary care.21 Digital videocapillaroscopy is now a gold standard: it provides a significantly higher magnification (from × 50 to × 1000) and allows a precise measurement of capillaroscopic parameters.21 Magnification of × 200 is one of the most suitable options for everyday clinical practice as well as for research purposes, providing an opportunity for the assessment of capillary distribution and certain details in the structure of the capillary loops.21 An excellent inter- and intraobserver agreement was also obtained by experienced vascular physicians for the diagnosis of SSc pattern with a magnification of × 100.38 According to the authors, it is easier to assess the global architecture of the capillary bed using wide‑field capillaroscopy ( × 100) than narrow‑field capillaroscopy ( × 200).38 A comparative evaluation of dermoscopy and capillaroscopy in RP showed that 80% of patients had the same status, normal or abnormal, for both capillaroscopy and dermoscopy, which resulted in the same clinical management.39 Nonetheless, the reference method continues to be capillaroscopy.39
Infrared thermography
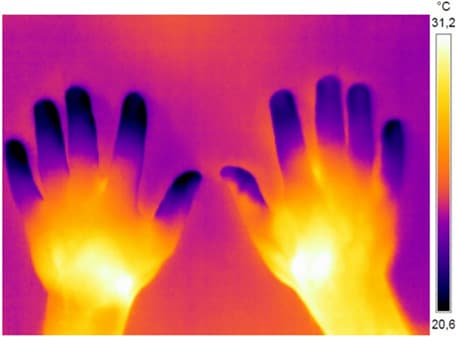
Thermography assesses vascular function (blood flow), providing a color image of the surface temperature (Figure 4). Dynamic testing of patients’ response to cold challenge is mainly used to diagnose RP.40 The assessed parameters are basal temperature prior to cold provocation, temperature immediately after the cold challenge, the maximum temperature recovery rate (the time between the end of the cold challenge and the onset of rewarming), recovery index (the ratio between a temperature increase and an initial temperature decrease × 100%).40 The thermal gradient (fingertips and the dorsum of the hand difference) may be applied to differentiate between healthy individuals and those with RP.40 While in healthy people the thermal gradient is typically positive, in RP it is usually negative due to a lower digital temperature (~26°C–28°C) in comparison with the dorsum of the hand (~31°C) in the resting state or in response to cold provocation.41 Patients with RP reheat their hands slower than controls.41 After the ice water immersion test, the digital temperature of healthy persons returns to normal in 10 minutes or less, whereas in patients with RP, it takes much longer (about 35 minutes).41 Campos et al42 suggested that the ring finger (fourth finger) could become a reference in studies to determine cutting points and to facilitate the clinical diagnosis of RP. A lower recovery rate and thermal gradient as well as a higher disparity in the nailfold temperature between the fingers at baseline and also after cold challenge were found in patients with SSc and may be useful for differentiating secondary RP from primary RP.43 As baseline images were more helpful, a mobile phone thermography seems to be a feasible additional tool in the assessment of patients with RP.44 The first multicenter study that was undertaken to determine the reliability and validity of a hand cold challenge protocol using mobile phone thermography in patients with SSc‑related RP confirmed that small variations in room temperature are acceptable during the imaging.44 Further research is needed to establish ranges of normality and abnormality and to validate the use of this method.44
Laser Doppler and other techniques
Laser Doppler techniques are tools for microcirculatory research evaluating peripheral blood flow. They were used to monitor vasoactive therapy effects in trials on SSc.45 Flow can be measured over a point (laser Doppler flowmetry) and over an area (laser Doppler imaging, laser speckle contrast analysis, and laser speckle contrast imaging).45 Some authors reported that measuring the baseline microvascular blood flow and then time‑to‑peak flow after occlusion using laser Doppler flowmetry may be a highly accurate test for differentiating patients with primary RP from healthy controls.45 The postocclusive time‑to‑peak flow had a superior specificity of 90% as compared with 66% for baseline microvascular flow.45 Laser Doppler imaging, speckle contrast analysis, and speckle contrast imaging are characterized by a higher reliability, but they are more expensive and are not yet widely accessible.46
The assessment of blood perfusion in RP may be also performed by hand perfusion scintigraphy.47 This method was reported to play a role in the diagnosis of RP and evaluating the response to therapy.47 A γ-camera dynamic first‑pass study (blood flow) during the first 60 seconds differentiated healthy controls from patients with RP (primary and secondary), while a static study (blood pool) after 5 minutes distinguished primary from secondary RP.47 However, the main disadvantage of scintigraphy is the use of radioactivity.47
It seems that the novel multisite photoplethysmography might be a practical and low‑cost cardiovascular assessment tool for differentiating SSc from healthy controls and patients with primary RP by measuring endothelial function.48 Endothelial and autonomic function as well as arterial disease were assessed using a pulse‑wave analysis.48
The identification of patients with RP and evaluation of their response to a cold stimulus over time by using photoacoustic imaging with a center frequency of 18MHz and an optical wavelength range of 680 nm to 970 nm, which allowed to quantify tissue oxygenation levels, were also reported.49 However, all these techniques are currently mainly available only in specialist centers and need further validation studies prior to their implementation in clinical practice.50
Evaluation of a potential pathology in large to medium–sized arteries
Doppler ultrasonography is commonly used for evaluation of peripheral blood flow in patients with RP.51 Some researchers prefer color Doppler ultrasound and only use power Doppler ultrasound if the flow is very low.52 Baseline flow volume measurement can be recommended to patients who refuse the examination with cold provocation.52 Vessel diameter and flow rate at baseline and after cold provocation were found to be lower in patients with primary and secondary RP than in the control group.52 Flow volume normalization time was found to be different in primary and secondary RP than that in the healthy group, even after treatment.52 Vessel patency and wall damage of the digital arteries could be visualized in patients with secondary RP.53 As structural changes are very common in patients with SSc, a significant co‑occurrence of vasculopathy (number of narrowed or occluded digital arteries) and concomitant digital ulcers or pitting scars in the same finger were found.53 Examination of digits II to V selectively might be a prognostic tool for the development of digital ulcers in patients with SSc in future studies.53 Lescoat et al54 and Schioppo et al55 suggested that the ulnar artery occlusion and finger pulp blood flow were associated with capillary loss assessed by nailfold videocapillaroscopy, but longitudinal studies are needed to explore the predictive value of these parameters.
The differentiation between a vasospastic and an obstructive mechanism may be also made using finger systolic pressures, pulse volume recording, or pulse contour analysis by strain‑gauge plethysmography or photoplethysmography.48 A difference of more than 15 mm Hg between fingers or an absolute finger systolic blood pressure of less than 70 mm Hg may indicate occlusive disease.48 The normal finger–brachial index may range from 0.8 to 1.3. Sphygmic wave amplitude is markedly lower in RP patients than in healthy controls.48
Conventional angiography and magnetic resonance angiography provide anatomic information about the location and extension of the occlusive lesions and are used to assess peripheral circulation in RP, but these techniques require an injection of contrast dye and extensive workup, which may limit their applicability for screening.48
Monitoring of patients with primary Raynaud phenomenon for the development of connective tissue disease
The diagnosis of SSc may be delayed for several years after the onset of RP and even after the onset of the first non‑RP symptom.56 Patient organization–led initiatives can play an important role in raising awareness about RP.56 Carefully designed tools can provide reassurance to people interested to learn about RP and encourage an earlier medical assessment of people at risk of a potentially life‑threatening disease such as SSc.56
No findings suggestive of secondary causes (eg, ulcerations, tissue necrosis or gangrene, sclerodactyly, calcinosis, or skin fibrosis), no history of an existing CTD, negative or low ANA titers (eg, 1:40 by indirect immunofluorescence), and normal capillaroscopy are included in the diagnostic criteria for primary RP.18 However, because some patients with characteristics of primary RP can later progress to secondary RP (Figure 5), any patient developing RP in adulthood, especially after the age of 35, should be regularly screened for the development of CTD, including SSc, with evaluation of proximal nailfold capillaries and serology testing.57 A high index of CTD suspicion should also be applied in children under the age of 12, as primary RP may be less common in younger age groups.21 Secondary RP is associated with juvenile systemic lupus erythematosus, mixed CTD, and rarely with SSc and Sjögren syndrome.21 The European expert panel recommends testing ANAs, more specific antibodies associated with CTD, and nailfold capillaroscopy in all children presenting with RP.58
Biomarkers
Several studies have suggested that in CTD microcirculatory changes develop before morphological abnormalities are seen on nailfold capillaroscopy.59 Markers of endothelial damage (plasma levels of tissue‑type plasminogen activator, von Willebrand factor, and interleukin 6) were elevated in patients with RP who subsequently developed SSc or other CTDs, even in the absence of capillaroscopic abnormalities.60 Biomarkers were also emerging as predictors of digital ulceration in SSc (increased ET‑1 and low vascular endothelial growth factor levels) and were proposed as novel markers for anti‑ischemic therapy (hypoxia‑inducible factor 1 and heme oxygenase 1) in RP.61,62
Lifestyle and psychotherapeutic interventions
A very important component of the management of patients with RP is lifestyle modification. Because RP is a vasospastic event, it is important that patients are educated to avoid vasoconstrictive stimuli, including cold, stress, repeated trauma to the fingertips, vibrating tools, caffeine‑containing drinks, nicotine, or any vasoconstrictive medications.63Patients should wear gloves in cold environments, be counseled on the importance of smoking cessation, and be given a list of commonly used vasoconstrictive drugs to avoid.63Difficulties resulting from RP are usually present and disabling all year round, which underscores the importance of nonpharmacologic strategies throughout the year.63
The activity and severity of RP can be measured by the Raynaud’s Condition Score (RCS) that looks at the quality of life (QoL), frequency and severity of attacks, and the effect of RP on an individual.64 Of note is that a number of factors, such as pain, catastrophizing, and coping strategies, may influence the RCS.65 No correlations were observed between the severity of vasoconstriction and pain intensity, pressure pain sensitivity, pain magnitude, and pain threshold.2 Significantly more patients with secondary RP had anxiety and depressive symptoms than patients with primary RP (43.9% vs 23.3% and 31.7% vs 11.7%, respectively).66 Patients with secondary RP have a poorer physical health condition and RP‑specific QoL than patients with primary RP.66 The severity of RP had one of the strongest associations with reduced hand function in SSc.67 Therefore, anxiety, depression, and reduced QoL should be considered when managing all patients with RP.64 Patients who have high levels of anxiety and depression and low QoL should be referred for psychological care.64Increasing exercise, reducing stress levels, treatments targeting pain related to RP in the course of SSc, and the development of behavioral interventions enhancing coping strategies may reduce the burden of RP in the course of SSc.65Unfortunately, in a systematic review on this topic, only 7 studies reporting biofeedback and 1 study testing a behavior therapy were identified as randomized controlled trials (RCTs).68 Five studies reported significant effects in primary outcomes of interest; however, due to missing data, relative efficacy of interventions could not be reliably assessed.68
Pharmacologic treatment
The European Society for Vascular Medicine guidelines and an update of the EULAR recommendations on the management of RP have been published recently, but the evidence base for the treatment of both primary and secondary RP is weak to moderate.21,69 Although the course of secondary RP is thought to be directly related to the progression of an underlying disorder, whether to treat or not to treat patients with SSc in the earliest phases remains a dilemma.70 It is rather believed that pharmacologic therapies should be added only if attacks remain poorly controlled and present with disabling symptoms, or if the patient has digital ulcers.71
First‑line pharmacotherapy
The recommended first‑line pharmacologic treatments for primary and secondary RP are vasodilators such as dihydropyridine calcium channel blockers (CCBs).21,69 A recent systematic review of 38 RCTs with an average duration of 7.4 weeks and 982 participants revealed that CCBs slightly reduce the frequency and severity of RP attacks, as self‑reported by patients (moderate‑quality evidence).72 In addition, CCBs produced a potentially clinically important moderate improvement in pain associated with RP.72 Nifedipine was the most extensively studied CCB, but the newer second‑generation drugs (amlodipine, isradipine, nicardipine, and felodipine) were also effective in reducing the number of RP attacks. The most common side effects are headache, dizziness, nausea, palpitations, and ankle edema. Serious adverse events (death or hospitalization) were not reported.72 Use of CCBs may also be limited by hypotension.21,69 When starting these medications, the lowest dose should be prescribed and gradually titrated every 4 weeks depending on a patient’s response.21,69
Second‑line pharmacotherapy
The use of phosphodiesterase type 5 inhibitors (PDE5i) is recommended as second‑line therapy.21,69 Tadalafil, sildenafil, udenafil, and vardenafil appeared to have significant but moderate efficacy in secondary RP.73 Adverse effects of these medications include flushing, headache, dizziness, and, less commonly, hypotension, arrhythmias, cerebrovascular accident, and vision changes.73 PDE5i should be started at a low dose, and then titrated depending on response over a period of 4 to 6 weeks.21,69 If patients with RP are not willing to take a long‑term treatment “as required,” then single doses of sildenafil before or during exposure to cold may be a good alternative.74 Due to a highly heterogeneous response, there is a need for personalized approach to the treatment of RP.74
Third‑line pharmacotherapy
Intravenous prostaglandins are recommended for severe RP in the course of SSc when oral therapy (including CCBs and PDE5i) has failed.21,69 Prostaglandins function as a strong vasodilator and also prevent platelet aggregation.
According to the PROSIT study experts, iloprost was used earlier across Italian tertiary centers (in combination with or immediately after CCBs) and represented the first‑line choice for the management of severe RP and digital ulcers in SSc.75 PDE5i were more rarely prescribed and were generally employed as late treatment for RP.75 The standard treatment protocol consists of intravenous infusion of iloprost at a rate of 0.5 to 2 ng/kg/min for 3 to 5 consecutive days, through a peripheral venous access.75 Due to common side effects (hypotension, flushing, nausea, and headaches), patients usually require hospitalization.75
According to Bellando‑Randone et al,76 in the fibrotic or atrophic phase of SSc, iloprost was well tolerated and side effects were managed by reducing or modulating the infusion rate. In edematous patients, side effects were more frequent and led to drug withdrawal, mostly because of painful digital swelling and diarrhea.76 Calcium channel blockers should be temporarily stopped while using iloprost, and such a pretreatment approach might reduce or control adverse events.76
It should be noted that portable devices for iloprost infusion have been recently designed, allowing outpatient treatment.77,78 The devices were demonstrated to be safe, feasible, and effective, with higher patient satisfaction and consequently greater treatment adherence.77,78 Other intravenous prostaglandins include epoprostenol, treprostinil, and alprostadil. There is limited evidence for the benefit of oral prostacyclin analogues in patients with RP.79
Intravenous prostaglandin infusions combined with anticoagulation (heparin, 5000 UI twice daily) is preferable in secondary RP with acute digital or limb ischemia.51 A digital or regional block with lidocaine or bupivacaine may be also performed to temporarily relieve vasospasm in such situations.7
Topical vasodilators
A meta‑analysis, which included 7 placebo‑controlled trials and a total of 347 treated patients, demonstrated a significant treatment benefit for topical nitrates for RP without serious side effects.80 However, the dose must be carefully adjusted: it should be sufficient to cause local vasodilation but not high enough to result in systemic absorption and the risk of adverse systemic effects such as hypotension, dizziness, and headache.81,82 There is limited evidence regarding the effectiveness of other topical vasodilators for the management of RP. One study suggested that topical sildenafil can significantly improve digital arterial blood flow in patients with secondary RP, while there was no significant improvement after topical nifedipine.83 A case where rosemary essential oil, as compared with olive oil, produced replicable warming of the hand in a patient with SSc and RP was also reported.84
Other options
There is insufficient evidence to recommend selective serotonin reuptake inhibitors (fluoxetine), angiotensin‑converting enzyme inhibitors (captopril, enalapril, and quinapril), angiotensin receptor blockers (losartan), α-blockers (prazosin), and phosphodiesterase 4 inhibitors (pentoxifylline) for the treatment of RP.21,69,85
Trials on ET‑1 receptor antagonists such as bosentan and macitentan showed no evidence of improvement in the frequency of RP attacks.86 Nonetheless, bosentan is currently approved for the secondary prevention of digital ulcers in patients with SSc. However, it use may cause hepatotoxicity, headache, flushing, edema, fatigue, and hypotension.86 Typically, bosentan is prescribed at a dose of 62.5 mg twice daily for 4 weeks, with the dose escalation to 125 mg twice daily if needed.86 In patients with a history of digital ulcers, low‑dose aspirin should also be used.86 It was reported that clopidogrel treatment may be associated with the development of new digital ulcers in patients with SSc.87
Riociguat and aminaphtone seem to be promising new treatment options for RP.88,89 In a pilot study, a single dose of riociguat was well tolerated and resulted in a rapid improvement in digital blood flow in some patient subsets with primary and secondary RP.88 Aminaphtone is used in some European countries in the treatment of chronic venous insufficiency of the lower limbs, leg ulcers, and diabetic microangiopathy.89 A 6‑month open feasibility study demonstrated that aminaphtone treatment increases skin blood perfusion and improves clinical symptoms of RP, with sustained efficacy for up to 6 months, even in patients with SSc.89
Some positive effects of botulinum toxin (BTX) A were reported, but its clinical significance is still unclear.90 An RCT in 40 patients with SSc showed that BTX‑A did not significantly improve blood flow to the hands of patients with SSc‑related RP, although there was a significant clinical improvement of RP in hands treated with BTX‑A.90 A 3‑year retrospective study in 15 patients revealed that BTX‑A was generally well tolerated.91 Similarly, BTX‑B injections significantly suppressed the activity of RP and digital ulcers in patients with SSc without serious adverse events.92 Weum and de Weerd93 postulated that a single ultrasound–guided BTX injection around the radial artery allowed a precise administration and distribution of BTX in the perivascular space. The single‑injection technique was much less painful, with minimal risk of temporary intrinsic muscle weakness, as compared with multiple injections in the palm of the hand.93 BTX‑A can inhibit arteriole vasoconstriction in a dose‑dependent manner by cleaving SNAP‑25 in sympathetic neurons, thus providing a theoretical basis for the treatment of RP.94
In a systematic review and meta‑analysis of 14 RCTs, herbal medicine was found to be potentially safe and effective treatment for cold hypersensitivity in the hands and feet as well as for RP.95 The most common herbal medicines were Cinnamomi ramulus or Cinnamomi cortex and Zingiberis rhizoma.95 However, according to the authors, the high risk of bias in all studies prevents definitive conclusions.95 Ginkgo biloba, acupuncture, and other alternative therapies (laser and nutritional supplements) did not prove to impact the frequency, duration, and severity of RP.7,51
Sympathectomy
In patients with RP refractory to medical treatment, digital periarterial sympathectomy can be a good treatment option, especially in cases of arteritis associated with very severe spasms.96 Endoscopic thoracic sympathectomy should be considered an ultimate choice for patients with RP who have treatment‑resistant severe symptoms and serious complications, disturbed social and daily lives, and impaired QoL.97All patients should be properly informed before the surgery about the possibility of a high rate of recurrence (66.6%).97
In summary, current pharmacologic treatments fail to completely control RP and prevent digital ulcers, and they are not tolerated by many patients. Therefore, the treatment of RP should not only focus on the vascular response but also on lifestyle interventions, including pain education, cognitive behavioral therapy, and exercise therapy. Collaboration between healthcare professionals, patient organizations, and the society can positively influence health utilization by encouraging involvement of people in their own healthcare. Such partnership is necessary for the very early diagnosis of SSc.
- Gregorczyk‑Maga I, Frołow M, Kaczmarczyk P, Maga P. Microcirculation disorders of the oral cavity in patients with primary Raynaud phenomenon. Pol Arch Intern Med. 2019; 129: 36‑42.
- Tapia‑Haro RM, Guisado‑Barrilao R, García‑Ríos MDC, et al. Pain intensity, pressure pain hypersensitivity, central sensitization, and pain catastrophizing related to vascular alterations in Raynaud’s phenomenon: a preliminary case‑control study. Pain Med. 2019; 15: pnz089. | Crossref
- Garner R, Kumari R, Lanyon P, et al. Prevalence, risk factors and associations of primary Raynaud’s phenomenon: systematic review and meta‑analysis of observational studies. BMJ Open. 2015; 5: e006389. | Crossref
- Munir S, Freidin MB, Brain S, Williams FMK. Association of Raynaud’s phenomenon with a polymorphism in the NOS1 gene. PLoS One. 2018; 13: e0196279. | Crossref
- Carlsson D, Wahlström J, Burström L, et al. Can sensation of cold hands predict Raynaud’s phenomenon or paraesthesia? Occup Med (Lond). 2018; 68: 314‑319. | Crossref
ARTICLE INFORMATION