Fibrinogen Łódź: a new cause of dysfibrinogenemia associated with recurrent thromboembolic arterial events



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Fibrinogen Łódź: a new cause of dysfibrinogenemia associated with recurrent thromboembolic arterial events
A 51‑year‑old woman was referred for thrombophilia testing due to recurrent thromboembolism. She had 3 episodes of embolism experienced at the age below 50 years, namely, to the right brachial artery, to the left external iliac artery and the common femoral artery with thromboembolectomy, and to the right popliteal artery. She was treated with acenocoumarol (target international normalized ratio, 2–3). Due to nontherapeutic international normalized ratio values, in 2017 she was switched to rivaroxaban 20 mg per day and aspirin 75 mg per day. The patient had a single short episode of paroxysmal atrial fibrillation; however, there were no abnormalities on repeated electrocardiogram, 24‑hour Holter recordings, and transthoracic echocardiography. She had 4 miscarriages and 1 successful pregnancy. Her son had myocardial infarction at the age of 23 years. At the first clinic visit in August 2018, she was in good medical condition. After switching to enoxaparin, thrombophilia screening was performed with negative results. However, a low fibrinogen concentration by von Clauss assay (1.17 g/l [reference range, 2.1–4.0 g/l]) combined with prolonged thrombin time of 22.7 seconds (reference range, 10.3–16.6 seconds) and normal fibrinogen antigen level determined nephelometrically (2.5 g/l; [reference range, 1.8–3.5 g/l]) were found. Thrombotic‑related dysfibrinogenemia (category 3B according to the new classification by Casini1) was diagnosed in January 2019. To confirm it, a whole‑exome sequencing analysis was performed at the Health 2030 Genome Center Sequencing Platform in Geneva, using Exome Research Reagents (Integrated DNA Technologies, Geneva, Switzerland), multiplexing 12 samples during library preparation, with an estimated mean coverage of 70X. Variant calling was filtered for variants located in a gene panel of 27 genes of the coagulation and fibrinolytic pathways. The presence of variants in the fibrinogen genes was confirmed by Sanger sequencing.
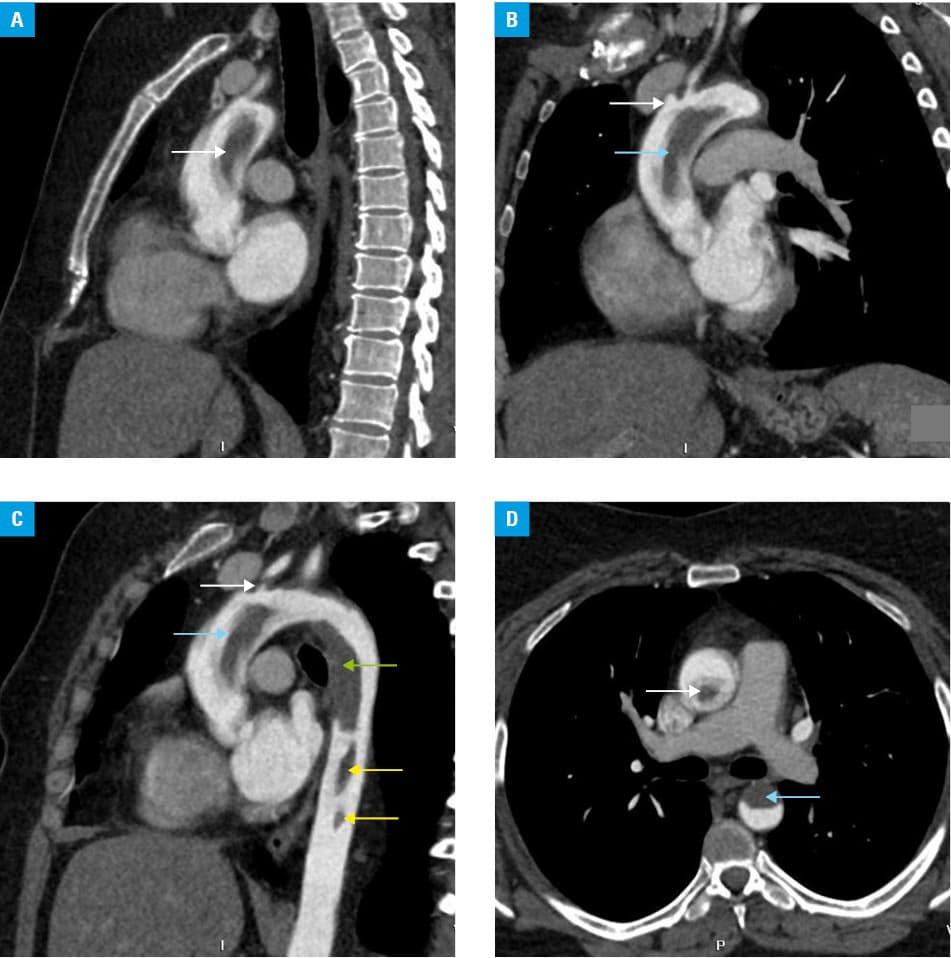
Despite the use of rivaroxaban and aspirin, computed tomography angiography (January 2019) showed large thrombi in several arteries including the ascending aorta (Figure 1A–1D). The patient was referred for consultations with vascular and cardiac surgeons. In March 2019, while on rivaroxaban 20 mg per day and aspirin, ischemic stroke with left‑sided paresis and aphasia occurred due to the right internal carotid artery occlusion. The patient was switched to apixaban (5 mg twice a day) in combination with low‑dose aspirin.
The exome sequencing analysis identified a novel heterozygous missense mutation in FGG exon 8: c.998 A>G; p.His333Arg (p.His307Arg without the signal peptide) which we named Fibrinogen Łódź. This mutation, predicted to be deleterious by the SIFT prediction algorithm and probably damaging by the PolyPhen‑2 algorithm, affects the same amino acid as Fibrinogen Mannheim II.2
Fibrinogen Łódź is unique due to numerous severe arterial thrombotic manifestations in patients below 50 years of age without any venous thrombosis or bleeding and apparent resistance to rivaroxaban. Such clinical phenotype in patients with dysfibrinogenemia is quite uncommon, although 25% of cases of dysfibrinogenemia are associated with mainly venous thrombosis, for example, Fibrinogen Dusart.3 This case suggests that dysfibrinogenemia should be considered in patients with arterial thromboembolism at an early age. Establishing a proper diagnosis of dysfibrinogenemia allows the initiation of anticoagulant therapy and genetic counseling in asymptomatic family members, similarly as in other thrombophilias.4,5
- Casini A, Undas A, Palla R, et al; Subcommittee on Factor XIII and Fibrinogen. Diagnosis and classification of congenital fibrinogen disorders: communication from the SSC of the ISTH. J Thromb Haemost. 2018; 16: 1887‑1890. | Crossref
- Dear A, Dempfle CE, Brennan SO, et al. Fibrinogen Mannheim II: a novel gamma307 His->Tyr substitution in the gammaD domain causes hypofibrinogenemia. J Thromb Haemost. 2004; 2: 2194‑2199. | Crossref
- Wypasek E, Klukowska A, Zdziarska J, et al. Genetic and clinical characterization of congenital fibrinogen disorders in Polish patients: identification of three novel fibrinogen gamma chain mutations. Thromb Res. 2019; 182: 133‑140. | Crossref
- Bagoly Z. Uncovering the genetic background of natural anticoagulant deficiencies: time to look behind the scenes. Pol Arch Intern Med. 2017; 127: 465‑467. | Crossref
- Wypasek E, Corral J, Alhenc‑Gelas M, et.al. Genetic characterization of antithrombin, protein C, and protein S deficiencies in Polish patients. Pol Arch Intern Med. 2017; 127: 512‑523. | Crossref
ARTICLE INFORMATION