The interplay between muscle mass decline, obesity, and type 2 diabetes
Key words: insulin resistance, muscle mass decline, sarcopenic obesity, type 2 diabetes



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The interplay between muscle mass decline, obesity, and type 2 diabetes
The world’s population is progressively becoming older, and age‑related conditions are a major public health concern. A worrying phenomenon worldwide is the increasing obesity among aging societies, which occurs in parallel with a higher prevalence of sarcopenia in older populations. As a result of the combination of these 2 states, new medical conditions, such as sarcopenic obesity, have recently become a public health concern. Data from the literature indicate a higher risk of metabolic syndrome, type 2 diabetes (T2D), and atherosclerosis among patients with sarcopenic obesity than the risk associated with simple obesity or sarcopenia alone. The mechanisms underlying sarcopenic obesity are multifactorial. There is an interplay between low‑grade inflammation, insulin resistance, hormonal changes, a sedentary lifestyle, eating habits, and aging. The aim of this review is to summarize the available data regarding the definition, epidemiology, and pathways that lead to sarcopenic obesity, as well as treatment strategies.
Introduction
Sarcopenia refers to age‑associated muscle mass decline. Various medical societies define sarcopenia in different ways.1 The most well‑known and frequently used criteria were published in 2010 by the European Working Group on Sarcopenia in Older People (EWGSOP), which define sarcopenia as loss of muscle mass and low muscle function (strength or performance).2 After 8 years, the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) published a revised European consensus on the definition and diagnosis of sarcopenia based on the scientific and clinical evidence that has accumulated over the last decade.3 According to the updated consensus, the EWGSOP2 uses low muscle strength as the primary parameter of sarcopenia since it reflects muscle function in the most reliable way. Moreover, in these revised guidelines, it is acknowledged that strength is better than mass for predicting adverse outcomes. As stated by the EWGSOP2, sarcopenia could be suspected when low muscle strength is detected. To make a diagnosis of sarcopenia, the additional presence of low muscle quantity or quality is necessary in the presence of low muscle strength. When the 3 criteria (low muscle strength, low quantity or quality, low physical performance) are fulfilled, sarcopenia is considered severe.
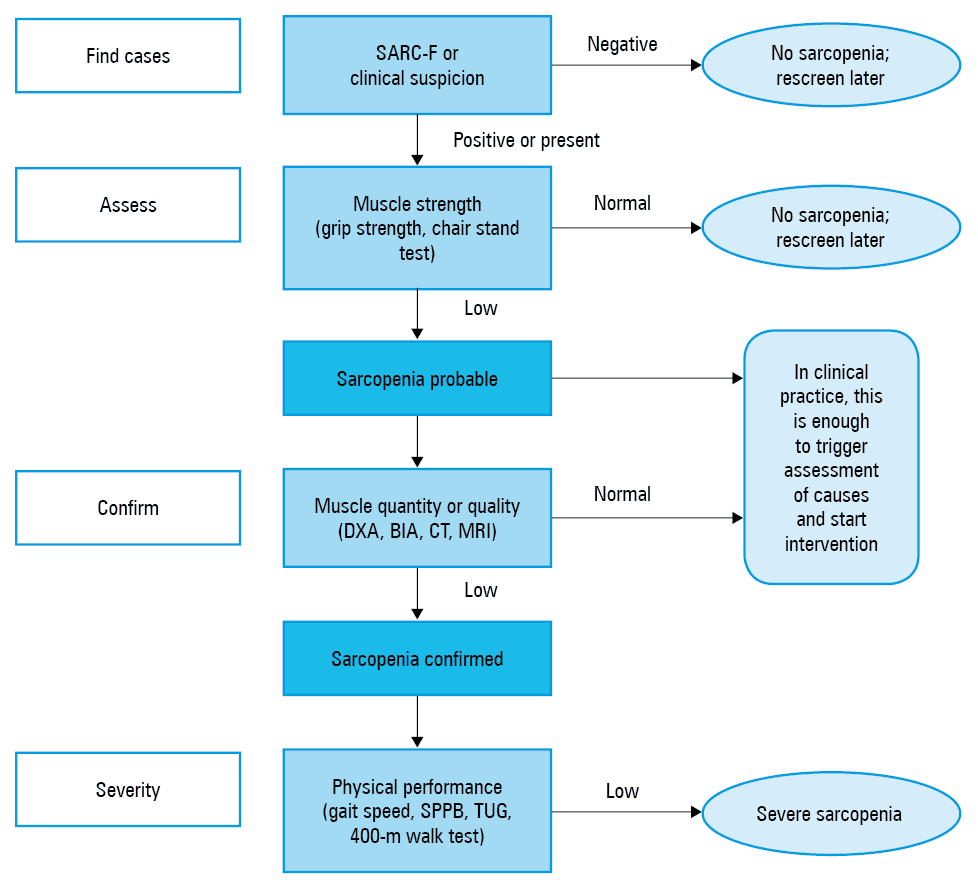
Of note, there is a selection of measuring tools by which muscle mass is assessed. Computed tomography (CT) scans and magnetic resonance imaging (MRI) are considered the gold standards for muscle mass evaluation.2,3 The cutoff points for low muscle mass are not yet well defined for these measurements. Due to the limited access and high cost of the abovementioned imaging studies, the EWGSOP recommends dual‑energy X‑ray absorptiometry (DXA) as a reference method.2,3 Bioelectrical impedance (BIA) methods correlate with DXA, but BIA assessments seem to be less reliable because they are also dependent on hydration status.4 The EWGSOP2 updates its algorithm for sarcopenia case findings, diagnosis, and severity determination. The EWGSOP2 advises using the SARC‑F questionnaire to identify individuals with probable sarcopenia. In the next step of the algorithm, they recommend performing grip strength and chair‑stand measures to identify low muscle strength. To confirm low muscle quality or quantity, the DXA or BIA methods are advised for use in usual clinical care (Figure 1). EWGSOP2 provided cutoff points relevant to clinical practice (Table 1). The prevalence rates of sarcopenia vary significantly because of different definitions, measurement tools, and patient populations. The recently published data from a meta‑analysis involving 35 articles, estimate the prevalence of sarcopenia to be 10% in men and 10% in women.5 A higher prevalence of sarcopenia in both sexes has been identified among non‑Asian populations than among Asian populations (11% vs 10% in men and 12% vs 9% in women, respectively).5 However, the results from various studies regarding the association between gender and reduced muscle mass are inconsistent.6,7
Criteria | Men | Women | |
a Cutoff point for dual‑energy X‑ray absorptiometry
Abbreviations: ASM, appendicular skeletal muscle mass; others, see Figure 1 | |||
Low strength by chair stand and grip strength | Grip strength | <27 kg | <16 kg |
Chair stand | >15 s for 5 rises | ||
Low muscle mass | ASMa | <20 kg | <15 kg |
ASM/height2 | <7.0 kg/m² | <5.5 kg/m² | |
Low performance | Gait speed | ≤0.8 m/s | |
SPPB | ≤8 points score | ||
TUG | ≥20 s | ||
400‑m walk test | Noncompletion or ≥6 min for completion | ||
Sarcopenia and central obesity are changes in body composition that are both age related and often coexist in older patients. Obesity with sarcopenia is known as sarcopenic obesity, a new medical condition that is associated with a higher incidence of metabolic syndrome and type 2 diabetes (T2D).8 Sarcopenic obesity is generally defined as the combination of low lean body mass and high fat mass.9 There is no universally accepted definition of sarcopenic obesity; its current version is based on the definitions of sarcopenia and obesity. Different criteria used in diagnosing sarcopenic obesity affect the prevalence rates of sarcopenic obesity, which vary from 4% to 94%.10
Pathogenesis
The mechanisms underlying sarcopenic obesity are multifactorial. There is an interplay between aging, hormonal changes, a sedentary lifestyle, eating habits, and low‑grade inflammation combined with insulin resistance (Table 2).11
Sarcopenia | Primary sarcopenia | Age‑related sarcopenia |
Secondary sarcopenia | Activity‑related sarcopenia: sedentary lifestyle, limited mobilityDisease‑related sarcopenia: advanced organ failure, inflammatory, malignancy or endocrine diseasesNutrition‑related sarcopenia: inadequate dietary intake, malabsorption, gastrointestinal disorders (diarrhea, inflammatory bowel disease), or use of medication | |
Obesity | • Family inheritance
• Behavioral causes: poor eating habits, excessive calorie intake, sedentary life style
• Hormonal and metabolic effects
• Increase fat mass, mainly visceral obesity
• Low grade inflammation
• Insulin resistance | |
Aging as the physiological process contributing to sarcopenic obesity
The peak muscle mass in humans is estimated to occur at 30 years of age, and from that moment, a gradual loss of muscle mass begins, as well as parallel weight increase, mainly in the form of gained fat mass.12 An ectopic accumulation of fat, mostly in the liver (nonalcoholic fatty liver disease),13 muscles,14 and pancreas (nonalcoholic pancreatic disease) can be observed with aging.15 The result of skeletal mass decline is a decrease in the basal metabolic rate, which can fall by approximately 30% between 20 and 70 years of age,16 while the caloric intake does not necessarily decrease over the lifespan17; these changes together may lead to increased fat accumulation. Adipose tissue accumulation, insufficient physical activity, and decrease in protein intake are considered to be the most important factors contributing to muscle mass loss and obesity, leading to sarcopenic obesity.18
Muscle fibers are divided into 2 main types: slow‑twitch (type I) and fast‑twitch (type II) muscle fibers. Slow‑twitch muscle fibers are more efficient at using oxygen as fuel for continuous extended muscle contractions over a long period. Fast‑twitch fibers use anaerobic metabolism to create fuel, and they are better at generating short bursts of strength or speed than slow muscles. However, fast‑twitch fibers fatigue more quickly. A greater loss in the number and area of type II versus type I motor units with age has been observed.19 The loss of type II muscle fiber is mainly responsible for the reduced power of muscles, which is reflected by slower functional performance, such as slower gait speed and reduced muscle power.20
Loss of muscle power may appear earlier than loss of muscle strength associated with sarcopenia.21 Muscles have the ability to regenerate through the proliferation and differentiation of satellite cells.22 A number of local transcription factors, cytokines, and hormones (testosterone, insulin, insulin‑like growth factor 1 [IGF‑1]) stimulate this process.23 On the other hand, myostatin inhibits the proliferation and differentiation of satellite cells. The ability of satellite cells to proliferate decreases with age;24 moreover, obesity reduces the ability to repair skeletal muscle.25
Hormonal changes related to sex and aging
Changes in estrogen and testosterone occurring throughout the life course induce changes in body composition. In menopausal women, visceral fat mass and waist circumference increase, while fat‑free mass has a tendency to decrease.26 Estrogen deficiency enhances the age‑related decline of skeletal muscle mass, its strength, and regenerative capacity. In menopause, a decrease in skeletal muscle stem cells is observed because the ovarian hormones are necessary for satellite cell maintenance, self‑renewal, and protection from apoptosis, thereby promoting optimal muscle regeneration.27 It has been shown that estrogen protects skeletal muscle against apoptosis via its effects on heat shock proteins and mitochondria. Thus, estrogen deficiency contributes to the loss of muscle mass through apoptotic pathways.28 Moreover, decreased endogenous estrogen levels lead to disruptions in insulin secretion and insulin sensitivity, which predisposes to T2D, both independently of and additionally to aging.29 Menopausal hormone therapy containing estrogens can alter these changes and influence the repair of skeletal muscle mass.30,31
In men, during the natural process of aging, testosterone declines by approximately 1% per year, which negatively affects muscle mass and fat distribution.32 Physiologically, testosterone promotes muscle protein synthesis by increasing amino acid metabolism in skeletal muscle and alters androgen receptor expression.33 Moreover, testosterone enhances the regeneration of muscle tissue through satellite cell activation.34 Moreover, it has been shown that physiological decline of dehydroepiandrosterone, growth hormone, and IGF‑1 contributed to the development of sarcopenia.35
The role of diet
Additionally, the main problem in older people is inadequate protein intake compared with the overall protein requirements. Inadequate intakes of protein36 and vitamin D37 have been shown to promote sarcopenic obesity. Optimal protein intake is considered to be essential for maintaining muscle mass and strength. Therefore, efforts should be made to ensure that elderly patients in particular consume the recommended daily amount of protein.38
From adipose tissue inflammation to sarcopenic obesity
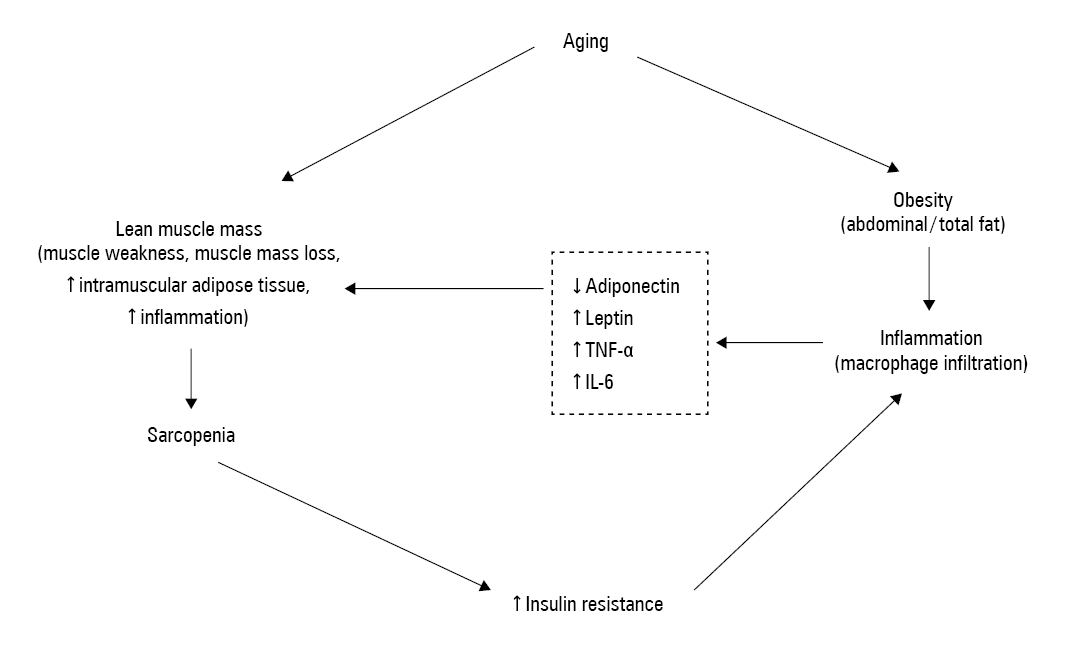
Age‑related weight gain results in fat accumulation.39 Excess adipose tissue is characterized by an increase in the size and number of adipocytes, which causes the infiltration of macrophages and other immune cells secreting proinflammatory cytokines and adipokines,40 leading to local and systemic chronic low‑grade inflammation.41 This obesity‑induced inflammation has been shown to be associated with muscle mass decline42 and may also result in insulin resistance. Moreover, this unfavorable adipokine/cytokine profile precedes insulin resistance and increases inflammation and oxidative stress, leading to ectopic fat deposition.43 The interplay between obesity, inflammation, muscle mass decline, and insulin resistance creates a vicious cycle (Figure 2) resulting in sarcopenic obesity and T2D development. Additionally, visceral adipose tissue accumulation is associated with a future loss of skeletal muscle, which is one of multiple mechanisms leading to sarcopenic obesity.44
In addition to general fat accumulation, as mentioned above, the ectopic storage of lipids between muscle fibers is a significant risk factor for further muscle dysfunction in older adults.45 Intramyocellular lipids cause a reduction in the number of mitochondria and produce reactive oxygen species, which may reduce the oxidative capacity of muscle, contributing to impaired muscle function.46
The main factors contributing to low‑grade inflammation are the overexpression of tumor necrosis factor (TNF) α in visceral adipose tissue and the infiltration of adipose tissue with macrophages.47 This mechanism links obesity and the immune system. During the process of weight gain, anti‑inflammatory M2 macrophage switches to pro‑inflammatory M1 macrophage, triggering the inflammatory process.48 M1 macrophages secrete pro‑inflammatory molecules such as TNF-α, interleukin (IL) 1, and IL‑6.49 TNF-α has been shown to directly reduce adiponectin signaling, mitochondrial biogenesis, and myogenesis in primary human myotubes.50
Adipose tissue is an active endocrine organ, and apart from cytokine secretion, it also produces adipokines (leptin and adiponectin, among others), which are involved in appetite, satiety, and energy expenditure regulation, and are associated with glucose and insulin levels and lipid metabolism.51 Adiponectin stimulates fatty acid oxidation and glucose uptake in skeletal muscles and adipose tissue through AMP‑protein kinase signaling.52 Interestingly, this effect is not observed in obesity.53 Moreover, the level of adiponectin decreases with age and with weight gain and negatively correlates with the amount of fat tissue.54 Adiponectin acts through its receptors AdipoR1 and AdipoR2, which are abundantly expressed in human skeletal muscle and primary myotubes.55 In contrast to adiponectin, the other adipokine, leptin, is positively correlated with overall adipose mass.56 Leptins exert a pro‑inflammatory effect by activating monocytes, leading to the secretion of the pro‑inflammatory cytokines TNF-α and IL‑6.57 An increased level of TNF-α and IL‑6 reduces the anabolic role of IGF‑1. Moreover, many of the anabolic effects of leptin on skeletal muscle are likely to be mediated by IGF‑1.57 Leptin receptors are abundant in skeletal muscles, and their expression is altered by physical activity.58 The effects of leptin are countered by adiponectin, but monocytes activated by leptin produce TNF-α, which inhibits adiponectin, resulting in reduced synthesis of muscle mass protein.59
Myocellular pathway potentially mediates the development of sarcopenia
Intramuscular fat infiltration in combination with low‑grade inflammation can result in an imbalance of myocytes that produce myostatin.
Myostatin, a member of the TGFβ superfamily, is a negative regulator of the growth of skeletal muscles.60 Myostatin contributes to muscle mass decline by inducing oxidative stress and producing reactive oxygen species in skeletal muscle cells through the TNF-α pathway.61 Interestingly, myostatin is also enhanced in aged skeletal muscle.62
Another factor involved in the crosstalk between muscle mass and obesity is irisin, a myokine that is mainly secreted from skeletal muscles during exercise and that may mediate some beneficial effects of exercise in humans, such as weight loss and an increase in thermoregulation. An increase in irisin causes the browning of human white adipose tissues. Irisin reduces pro‑inflammatory cytokines and induces M2 macrophage polarization, resulting in the anti‑inflammatory action of irisin on fat cells.63 Irisin promotes oxidative metabolism and mitochondrial biogenesis and reduces metabolic risk.64 Irisin positively correlates with muscle mass strength and metabolism.65 In several studies, it was reported that myostatin is upregulated and irisin is downregulated in sarcopenia.66,67 The opposite profile of myostatin/irisin has been proposed as promoting the browning of white adipose tissue with a beneficial effect on weight and insulin sensitivity.68
Other molecules are bone morphogenetic proteins, which enhance muscle growth by diminishing the negative effects of the TGFβ/myostatin/activin signaling pathway.69 Bone morphogenetic proteins promote the browning of white adipose tissue and inhibit insulin resistance and adipose fat tissue inflammation.70
The molecules mentioned above, secreted by myocytes, participate in crosstalk between skeletal muscles and adipose tissue, exerting negative effects.
Metabolic consequences of sarcopenic obesity
The interplay between reduced muscle mass and obesity can lead to insulin resistance, metabolic syndrome, and T2D. It has been shown that sarcopenic obesity increases the risk of metabolic syndrome and insulin resistance development more than obesity or sarcopenia alone.71 Similar findings have been found in the white population, where sarcopenic obesity was also associated with metabolic syndrome.72 The results of the study by Srikanthan et al73 supported the data mentioned, showing that relative muscle mass is inversely associated with prediabetes status. The same author showed that sarcopenia in patients under 60 years of age significantly correlates with a higher prevalence of T2D among obese populations.74 The findings listed above indicate that a one‑time measurement of muscle mass is associated with T2D and that a gradual decline in muscle mass observed over a few years correlates with glucose dysmetabolism and the development of T2D.11 In our study, we observed that a reduction in muscle mass over a 5‑year time span is a risk factor for T2D susceptibility, independent of insulin resistance among adults.75 Furthermore, the Korean Genome Epidemiology Study showed that low muscle mass was strongly associated with an increased risk of T2D, independent of obesity, in middle‑aged Korean adults during a 9‑year follow‑up.76 This is all the more important in the light of the fact that diabetes increases the risk of cardiovascular disease through various mechanisms, which have been recently well described and discussed by Gajos.77
Muscle mass in primary tissue contributes to whole‑body insulin‑mediated glucose disposal, accounting for almost 40% to 50% of lean body mass.78 Insulin is a powerful anabolic hormone that simulates muscle protein synthesis in young people but not older people.79 An adequate supply of essential amino acids stimulates protein synthesis.80 Physciologically, insulin acts through the mammalian target of rapamycin pathway that inhibits the degradation of protein. The impaired insulin signaling associated with insulin resistance may contribute to muscle loss in diabetes.81 Moreover, in aged muscle, the supply of amino acids and the perfusion of muscle are impaired,82 which may provide an additional explanation for the reduced protein synthesis. Moreover, in elderly individuals, impaired insulin‑mediated suppression of proteolysis is observed.83
Another important consequence of sarcopenic obesity is a higher risk of disability than that of healthy people.84 Sarcopenic obesity results in an increased risk of falls and fractures and leads to mobility disorders. Moreover, sarcopenic obesity is associated with cardiac disease, respiratory disease, and cognitive impairment and contributes to a reduced quality of life. Obese patients with reduced muscle mass are more prone to knee osteoarthritis and depression and have worse psychological health than individuals with normal muscle mass and a normal waist circumference.85 Data relating to sarcopenic obesity and mortality are conflicting.86 In financial terms, the presence of sarcopenia increases the risk of hospitalization and the cost of care during hospitalization.
Management of sarcopenic obesity
Taking into consideration all of the possible consequences of sarcopenic obesity, we should develop treatment strategies for obese patients with reduced muscle mass. The main points of treating sarcopenic obesity are based on weight loss together with an increase in physical activity. Intentional weight loss in older adults reduces morbidity and improves physical function.87 Anti‑obesity medications (liraglutide, orlistat, naltrexone/bupropion) are approved for use in obese patients younger than 65 years old, but they have not been evaluated for use among obese sarcopenic patients.88 In 9 older adults taking GLP‑1, a weight decrease (2 kg) was observed with a marginal improvement in the skeletal muscle index.89 The available data suggest that weight loss without exercise, while reducing fat mass, also inevitably decreases lean mass, thus worsening sarcopenia.90 The combination of a well‑balanced diet with exercise (aerobic plus resistance program) has been proposed as the best choice for the management of sarcopenic obesity.91 Aerobic training improves cardiometabolic health by reducing oxidative stress and inflammation. It also increases insulin sensitivity, decreases blood pressure, and improves the blood lipid profile. Notably, during aerobic training, energy expenditure is 2- to 3‑fold higher than during resistance training. During resistance training, the preferential reduction in visceral fat compared to peripheral fat is observed. Moreover, resistance training prevents the regaining of fat, especially visceral fat. Resistance training may be more useful to counteract sarcopenia, and aerobic training may be more useful to address obesity. The results from intervention studies (3- and 6‑month randomized controlled trials) revealed that people who performed resistance and aerobic exercise experienced more benefits, such as improved physical performance test, better quality of life, and greater strength compared with the same parameters in the aerobic group or resistance group alone.92 The combination of aerobic and resistance training could reduce the development of sarcopenia, decrease fat accumulation, and minimize the risk of developing metabolic disease.
Apart from physical activity, dietary intervention is the main goal of treatment strategies. A suggested approach is a calorie restriction of 500 to 1000 kcal per day to achieve a 0.5‑kg weight loss per week.93 Reduction in weight should be enhanced by adequate protein consumption to avoid protein anabolism during weight loss. The source of protein, the timing of protein intake, and specific amino acid consumption stimulate muscle synthesis.94 The recommended protein intake is 1.0 to 1.2 g/kg per day in healthy patients without renal failure.95 It has been shown that protein supplementation and resistance training increase lean mass, upper body strength, and leg strength more than resistance training alone.96 There are no available data in terms of vitamin D supplementation as a monotherapy for sarcopenic obesity. One intervention study in a Japanese population showed that vitamin D together with amino acid supplementation, tea catechins, and a combination of exercise reduced fat mass and improved physical function but not muscle mass in individuals with sarcopenic obesity.97 In summary, the right combination of exercise, a moderate‑weight‑loss‑inducing diet with an adequate protein supplementation seems to be the most effective strategy in terms of sarcopenic obesity treatment. Studies based on animal models have indicated that calorie restriction prevents age‑associated diseases and extends longevity by modulating mitochondrial activity and decreasing oxidative stress.98 Weight loss should be gradual to avoid a rapid loss of muscle mass. To the best of our knowledge, in terms of pharmacological management, there have been no trials evaluating the effects of the available anti‑obesity medications in obese sarcopenic subjects. Recently, a paper was published that showed the beneficial effect of myostatin antibodies among the elderly, demonstrating a decrease in body fat, an increase in skeletal muscle mass, and physical capacity improvement,99 but these findings should be confirmed in individuals with sarcopenic obesity. Only one study evaluating the impact of bariatric surgery in sarcopenic obese and nonsarcopenic obese patients showed similar weight loss and similar improvements in comorbidities in both the sarcopenic and nonsarcopenic morbidly obese groups.100
Conclusions
Sarcopenic obesity is a new challenging condition in aging populations, especially in the context of the current obesity epidemic. Sarcopenic obesity is a chronic state resulting in metabolic consequences, impairment of physical capacity, and likely an increased risk of mortality. The question regarding sarcopenic obesity is associated with an agreement on a uniform definition and the use of DXA rather than other measurement tools. It would be helpful to systematize the results from research and trials to create recommendations. Clarifying the mechanism that contributes to sarcopenic obesity may be useful for developing novel therapies. It should be kept in mind that weight loss, together with adequate protein intake and exercise, is essential for the management of sarcopenic obesity.
- Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014; 15: 95‑101. | Crossref
- Cruz‑Jentoft AJ, Baeyens JP, Bauer, JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010; 39: 412‑423. | Crossref
- Cruz‑Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019; 48: 16‑31. | Crossref
- Heymsfield SB, Gonzalez MC, Lu J, et al. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc. 2015; 74: 355‑366. | Crossref
- Shafiee G, Keshtkar A, Soltani A, et al. Prevalence of sarcopenia in the world: A systematic review and meta‑analysis of general population studies. J Diabetes Metab Disord. 2017; 16: 16‑21. | Crossref
ARTICLE INFORMATION