Life-threatening bleeding from an aneurysm in the arcuate artery of the kidney as a rare complication of granulomatosis with polyangiitis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Life-threatening bleeding from an aneurysm in the arcuate artery of the kidney as a rare complication of granulomatosis with polyangiitis
Granulomatosis with polyangiitis (GPA) is a systemic necrotizing inflammation of small and medium‑sized vessels. It most commonly affects the upper respiratory tract and kidneys,1 but it can also develop in other organs.2 Bleeding from aneurysms formed during the disease is a rare complication. In a Japanese review, 21 cases of arterial aneurysms in GPA were identified. In 4 cases, renal arteries or their branches were affected.3 Usually, aneurysms in the course of vasculitis were incidental findings during radiologic examination or was identified after aneurysm rupture.4
A 50‑year‑old, previously healthy man was hospitalized at a district hospital for 1 month due to fever, night sweats, and progressive pedal edema. Blood tests revealed high C‑reactive protein (CRP) levels, while computed tomography (CT) suggested pneumonia. The patient’s condition did not improve with broad‑spectrum antibiotic therapy. Development of kidney failure (increase in creatinine levels from 0.7 mg/dl to 3.7 mg/dl) and progression of pulmonary infiltrates with cavity formation raised the suspicion of GPA, and the patient was transferred to our unit.
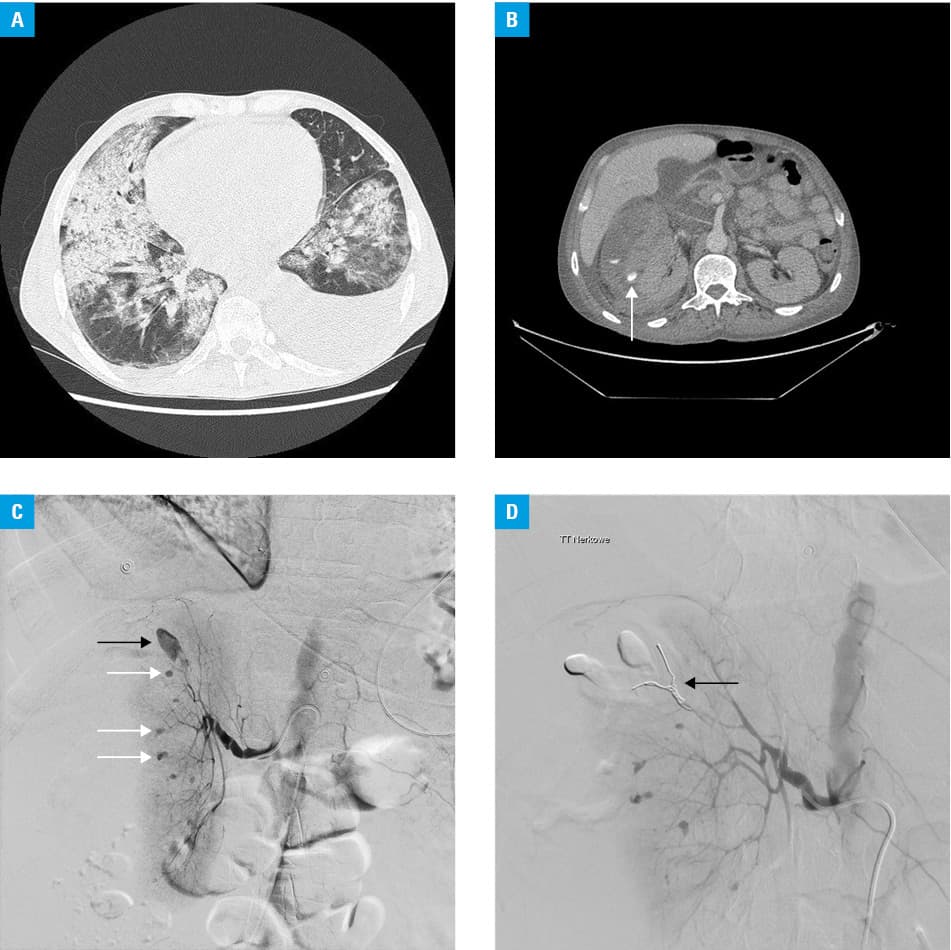
On admission, the creatinine level was 4.1 mg/dl; CRP, 211 mg/l; and albumin, 15 g/l; while cytoplasmic antineutrophil cytoplasmic antibody (cANCA) titer was 1:2560 and anti‑proteinase 3 antibody, 188 RU/ml. The patient presented with significant shortness of breath, and massive pulmonary infiltrates typical of GPA were noted on a CT scan (Figure 1A).
Severe, life‑threatening GPA with rapidly progressing glomerulonephritis was diagnosed. On a concomitant use of piperacillin/tazobactam, co‑trimoxazole and fluconazole, the patient started intravenous methylprednisolone, followed by pulse cyclophosphamide and plasma exchange therapy. Hemodialysis was started due to oliguria, overhydration, and lung edema. Vegetations on the aortic valve suggestive of endocarditis were found on echocardiography, and therapy with vancomycin was added.
On the 15th day of hospitalization, the patient experienced severe pain in the right flank, with a significant reduction in hemoglobin levels. Computed tomography angiography revealed a massive hematoma adjacent to the right kidney, with active bleeding from the ruptured aneurysm of the arcuate artery (Figure 1B). Numerous nonbleeding aneurysms in both kidneys were also visualized. Urgent embolization of the bleeding vessel was performed, which stopped the hemorrhage (Figure 1C and 1D). During hospitalization, control CT was performed twice, showing no further bleeding.
After the third pulse of cyclophosphamide, the patient’s condition improved and regression of pulmonary infiltrates was observed, but the patient remained dialysis dependent. Transesophageal echocardiography showed no signs of endocarditis. The patient was discharged home on a reduced dose of steroids. Laboratory tests at 1 month showed cANCA titers of 1:1280 and anti–proteinase 3 antibody titers of 147 RU/ml. Clinically, the patient presented again with endocarditis and pneumonia. His condition deteriorated and he died due to septic shock.
In conclusion, major hemorrhage from an aneurysm of a medium or large‑sized artery can be a rare manifestation of ANCA‑associated vasculitis. The signs suggestive of internal hemorrhage should raise the suspicion of this complication and prompt urgent diagnostic CT followed by intravascular intervention or surgery. In the present case, the hemorrhage was successfully managed with endovascular intervention, and the immunosuppressive therapy with steroids and cyclophosphamide induced remission of GPA.5 Unfortunately, the patient died of infectious complications, which is the most common cause of mortality in that population.
- Jennette JC, Falk RJ. Small‑vessel vasculitis. N Engl J Med. 1997; 337: 1512‑1523. | Crossref
- Gałąska R, Kulawiak‑Gałąska D, Czuszyńska Z, et al. A rare case of complex cardiac involvement in granulomatosis with polyangiitis. Pol Arch Intern Med. 2017; 127: 63‑65. | Crossref
- Niimi N, Miyashita T, Tanji K, et al. Aortic aneurysm as a complication of granulomatosis with polyangiitis successfully treated with prednisolone and cyclophosphamide: a case report and review of the literature. Case Rep Rheumatol. 2018; 2018: 9682801. | Crossref
- Tomosugi T, Takahashi T, Kawase Y, et al. Accessory left gastric artery aneurysms in granulomatosis with polyangiitis: a case report and literature review. Nagoya J Med Sci. 2017; 79: 75‑83.
- de Groot K, Harper L, Jayne DR, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody‑associated vasculitis: a randomized trial. Ann Intern Med. 2009; 150: 670‑680. | Crossref
ARTICLE INFORMATION