Determination and interpretation of MTHFR gene mutations in gynecology and internal medicine



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Determination and interpretation of MTHFR gene mutations in gynecology and internal medicine
Introduction
The widespread availability of genetic tests in the diagnosis of thrombophilia (a disorder involving the propensity for thromboembolic events) has contributed to their frequent hasty ordering and inappropriate interpretation. Fear of thrombosis prompts patients and doctors to perform a panel of genetic tests involving the detection of mutations of varying significance and frequency. Misinterpreted results are often the basis for the unjustified initiation of anticoagulant therapy or thromboprophylaxis, which can provoke bleeding. This expert opinion issued by the Hemostasis Group of the Polish Society of Hematologists and Transfusiologists (Polskie Towarzystwo Hematologów i Transfuzjologów) addresses the validity of determining the 2 most common MTHFR gene mutations.
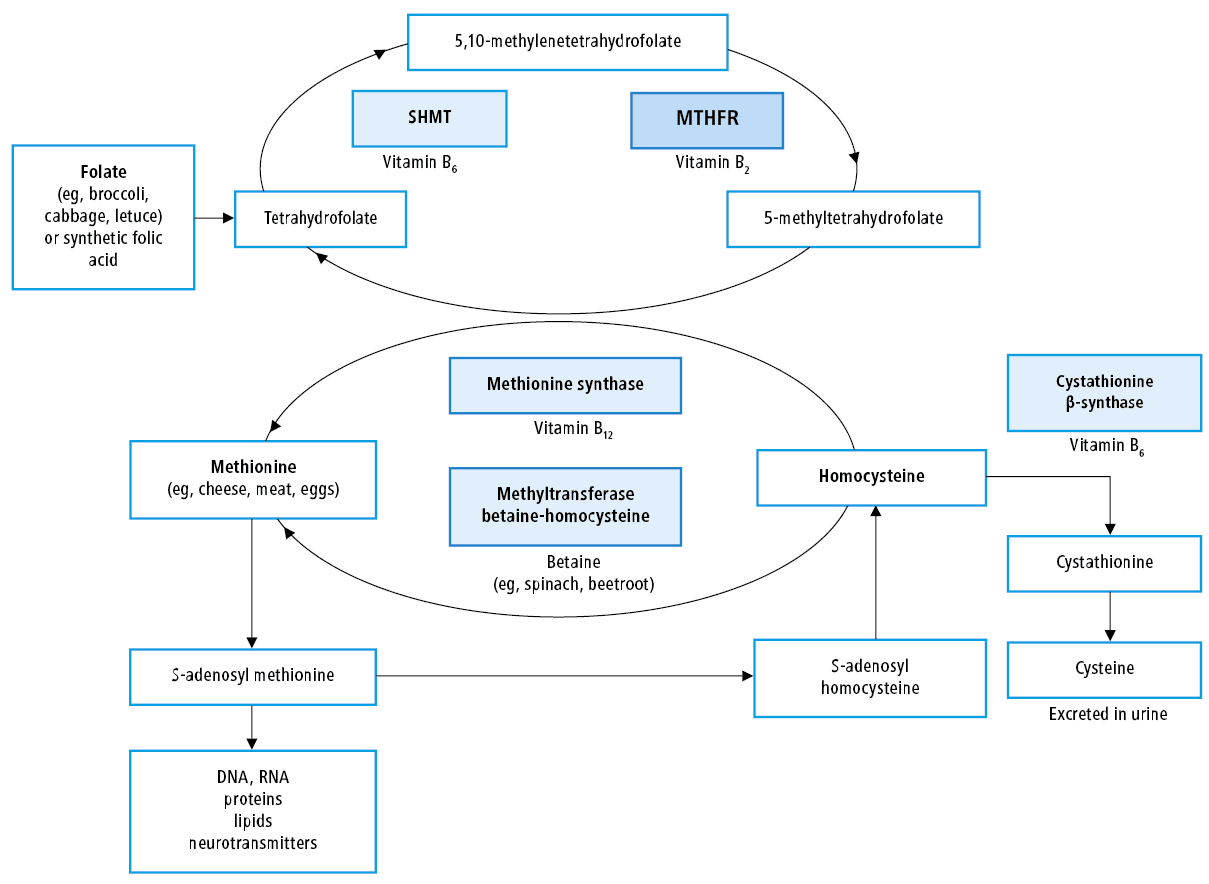
5,10‑methylenetetrahydrofolate reductase (MTHFR, EC 1.5.1.20) is an enzyme from the class of oxidoreductases, involved, among others, in the regulation of homocysteine concentration. This enzyme is necessary in the remethylation of homocysteine to methionine (Figure 1). It is also responsible for the conversion of 5,10‑methylenetetrahydrofolate to 5‑methyltetrahydrofolate, the basic active form of folates in humans.1 Homocysteine is formed in the metabolism of methionine (an amino acid necessary for the proper functioning of the body, supplied in animal proteins), and then is converted back to methionine in a reaction catalyzed by methionine synthase, whose coenzyme is 5‑methyltetrahydrofolate (the product of the MTHFR‑catalyzed reaction). S‑adenosylmethionine is formed from methionine, constituting the main source of methyl groups used in the synthesis of nucleic acids, many proteins, and lipid neurotransmitters.2 Homocysteine is finally transformed in a transsulfuration reaction involving cystathionine β-synthase to cysteine and excreted in the urine (Figure 1). The decrease in MTHFR activity promotes an increase in total homocysteine (tHcy) in the blood, especially in folate deficiency.
The MTHFR enzyme is encoded by the gene MTHFR located on chromosome 1 (1p36.22, OMIM 607093, NM_005957). The 2 most common congenital MTHFR polymorphisms in the white population are MTHFR 677C>T and MTHFR 1298A>C.
MTHFR 677C>T polymorphism
In carriers of the MTHFR 677C>T polymorphism (new nomenclature, c.665C>T, where “c” stands for coding DNA as the reference sequence; the terms C677T or C665T are no longer recommended; rs1801131 according to the Single Nucleotide Polymorphism Database), there is a cytosine (C) to thymine (T) transition at the nucleotide position of 677 in exon 4 of the MTHFR gene (according to the new nomenclature, 665), and as a consequence, a change of alanine to valine at amino acid 222 of this protein (p.Ala222Val). This heterozygous polymorphism reduces MTHFR activity by 40% (CT variant, MTHFR c. [665C>T]; [665C =]) and 70% in homozygous form (TT variant, MTHFR c. [665C>T], [665C>T]). The CT variant occurs in 20% to 40% of the white population and 1% to 4% of most other ethnicities. The TT variant occurs in about 10% of the general population in Europe.
MTHFR 1298A>C polymorphism
In carriers of the MTHFR 1298A>C polymorphism (new nomenclature, c.1286A>C, where “c” stands for coding DNA as the reference sequence; the term A1298C is no longer recommended; rs1801133 according to the Single Nucleotide Polymorphism Database), there is an adenine (A) to cytosine (C) transversion at position 1298 of the MTHFR gene (according to the new nomenclature, 1286) and, as a consequence, a change of glutamine to alanine at amino acid 429 of this protein (p.Glu429Ala). This polymorphism, found in 8% to 15% of the general white population (Asians, 1% to 4%), causes a less pronounced reduction of MTHFR activity than in the MTHFR 677C>T mutation, that is, by 10% in a heterozygous form (MTHFR c. [1298A>C]; [1298A =]) and by 40% in a homozygous form (variant CC; MTHFR c. [1298A>C]; [1298A>C]).
The decrease in MTHFR activity is more pronounced in people who are combined heterozygotes, that is, those who have the 677C>T variant in one allele of the MTHFR gene simultaneously and the 1298A>C variant in the other allele (recommended MTHFR c. [665C>T]; [1298A>C]).
The carriership of hetero- or homozygous variants of MTHFR polymorphisms is associated with a genetically determined predisposition to increased blood levels of homocysteine. Such people are more often found to have mild hyperhomocysteinemia—most often their fasting plasma levels are less than 30 µmol/l in the case of dietary folate deficiency (mainly from green leafy vegetables) (Figure 1).
A homocysteine concentration exceeding 15 µmol/l is an indicator of hyperhomocysteinemia, which is considered to be mild in the range from 15 to 30 µmol/l (>95% of cases). It is estimated that this form occurs in 5% to 7% of the general population, less often in people supplementing folate. In addition to a diet rich in animal protein (eggs, cheese, meat, etc) with a low supply of folate, hypothyroidism, chronic kidney disease, hypertension, obesity, diabetes, as well as smoking and chronic intake of certain drugs also contribute to a low degree of hyperhomocysteinemia, especially methotrexate (routine supplementation of folic acid is recommended in such patients). Vitamin B group and folic acid reduce homocysteine levels by approximately 25%.
Concentrations of homocysteine exceeding 100 µmol/l are found very rarely, and they are usually caused by very rare genetic mutations of cystathionine β-synthase, causing genetically determined disease, homocystinuria (in Poland several dozen cases), or other diseases, especially end‑stage renal disease. Homocystinuria, usually diagnosed in childhood or adolescence, is manifested by bone disorders, vision defects, and neurological disorders, and is also associated with an increased risk of premature atherosclerosis (especially stroke) and venous thrombosis.
To date, homocysteine levels have been studied in more than 600 disease entities—from migraine and autism to osteoporosis—and most commonly slightly increased levels were found in these observational reports.
In Poland, in many centers, especially private ones, it is usually recommended to pay for determination of the gene variants encoding MTHFR, and more specifically 2 common polymorphisms 677C>T (665C>T) and 1298A>C (1286A>C). Indications that prompt doctors to order such tests are usually: 1) recurrent or unprovoked (trauma, surgery, hormonal contraception, pregnancy, etc) events of venous thrombosis or pulmonary embolism; 2) obstetric complications, most often recurrent miscarriages or even a single pregnancy loss, most often in the first trimester of pregnancy; 3) sometimes only at the request of the patient.
This statement aims to briefly present the current state of knowledge on the MTHFR gene mutations and their relationship to obstetric complications and thromboembolic events as well as indications for genetic testing for these mutations.
Relationship between total homocysteine and MTHFR gene polymorphisms versus cardiovascular disease and venous thrombosis
Retrospective studies conducted in the 1980s have shown an increased incidence of homocysteine levels in the range of 15 to 30 µmol/l and MTHFR 677C>T polymorphism in the presence of concurrent folate deficiency in patients after myocardial infarction, stroke, and with coronary artery disease as well as with a history of venous thromboembolism (VTE), that is, deep vein thrombosis and/or pulmonary embolism.3-5 Meanwhile, prospective studies conducted in the next decade revealed that these correlations are weak or even nonexistent, which was best demonstrated by the results of a multicenter study published in 2002.6 Already in 2010, the American College of Cardiology and the American Heart Association made clear statements against the determination of homocysteine in the assessment of cardiovascular risk, recognizing hyperhomocysteinemia as an insignificant risk factor on the level of public health.7
Significantly higher tHcy levels and a more frequent occurrence of the MTHFR 677C>T variant were recorded in patients after a VTE incident.8,9 These relationships have disappeared in the population on a diet high in folate and B vitamins, especially in the United States, where since January 1998, folic acid is added to cereal products. Already in years from 2005 to 2010, prospective studies were published, which convincingly documented the lack of a relationship between the development of VTE and T allele and C allele carriership, respectively, for MTHFR 677C>T and 1298A>C polymorphisms.10,11 Furthermore, large clinical trials assessing whether the use of vitamin B group to reduce homocysteine levels lowers the risk of a first or recurrent VTE event have shown that, despite a 25% reduction in homocysteine levels, the risk of VTE is unchanged.12,13
Therefore, experts agree that the determination of MTHFR mutations should not be included in the panel of tests for congenital thrombophilia, that is, a genetically determined abnormality increasing the risk of VTE. The presence of these polymorphisms does not increase the risk of VTE and its recurrence, nor does it contribute to changes or prolongation of the anticoagulant therapy. The same applies to other frequently commercially commissioned genetic tests, such as the factor V gene H2 variant and the 4G/5G polymorphism (rs1799889) of the plasminogen activator inhibitor type 1 (PAI‑1) gene.
An increased risk of VTE is observed in individuals with the factor V Leiden mutation (rs6025; 5% of Poles) and prothrombin gene 20210A mutation (rs1799963; 3% of Poles), especially in the presence of additional prothrombotic factors, such as the use of hormonal contraceptives, trauma, or surgery.
In light of these data, all scientific societies advise against determination of homocysteine and MTHFR polymorphisms in the evaluation the VTE risk, considering that these tests should not be included in the diagnosis of thrombophilia.2
Relationship between homocysteine concentration and MTHFR polymorphisms and pregnancy complications, including miscarriages
Higher levels of homocysteine have been found in pregnant women with preeclampsia, premature placental abortion, and miscarriage. Currently, the prevalent view is that a slight increase in blood homocysteine levels after miscarriage is a consequence, not a cause of pregnancy loss.14 Already at the beginning of the 21st century, meta‑analyses of observational studies clearly showed that Caucasian women who are homozygous for the T allele of the MTHFR 677C>T polymorphism are not at a greater risk of recurrent miscarriages than women with the CT or CC variant of this gene. Similarly, no such relationship was detected in carriers of the C allele variant MTHFR 1298A>C polymorphism.15
As a consequence, for more than 10 years, no scientific society has recommended the determination of blood homocysteine levels or MTHFR polymorphisms in women following recurrent miscarriages (including the American College of Obstetricians and Gynecologists and the National Society of Genetic Counselors).14,16
Currently, to reduce the risk of developing neural tube defects, it is recommended to take multivitamin preparations containing 0.4 mg of folic acid before planned pregnancy.17 Higher doses should be considered in women with a previous fetal neural tube defect during pregnancy. Currently, it is not recommended to increase the dose of folic acid in pregnant women only on the basis of the detection of such a common genetic variant as MTHFR 677C>T.18,19
There is also no convincing data that other forms of folic acid, including methylated folates, are more effective than the most commonly used synthetic preparation in increasing blood folate and reducing homocysteine levels,20 therefore other forms of this vitamin should not be routinely recommended in pregnant women.
Testing for MTHFR polymorphisms is not recommended for the assessment of thromboembolic risk or for the diagnosis of recurrent miscarriages by the American College of Medical Genetics, the American Academy of Family Physicians, and American College of Obstetricians and Gynecologists.2,14
American College of Obstetricians and Gynecologists does not recommend tHcy or MTHFR mutation testing because there was no relationship between the MTHFR 677C>T polymorphism and obstetrical complications, including any increase in the risk of VTE during pregnancy.14
The position paper prepared by experts of the Polish Society of Human Genetics and the Polish Society of Gynecologists and Obstetricians on testing for MTHFR gene variants published in 2017 is consistent with other guidelines and contains the following recommendations21:
1 Studies of variants c.677C>T and c.1298A>C of the MTHFR gene are not justified in the search for the causes of recurrent miscarriages, regardless of the stage of pregnancy in which such complications occurred.2 Evaluation of these polymorphisms are not justified in diagnostics aimed at assessing the risk of developmental disorders of the central nervous system (brain and/or neural tube) in offspring, as well as other developmental defects.3 In women planning to have children, in order to reduce the risk of central nervous system defects, a standard prophylactic dose of folic acid of 0.4 mg/d should be used, regardless of the absence or presence of c.677C>T and/or c.1298A>C MTHFR polymorphism in the MTHFR gene if such a test has been performed.4 In the prophylaxis of fetal central nervous system defects, its active metabolites may also be used together with folic acid, irrespective of the absence or presence of c.677C>T and/or c.1298A>C MTHFR gene polymorphic variants.5 In the prevention of central nervous system defects in women who have previously given birth to a child with such a defect, a higher dose of folic acid in the amount of 4 to 5 mg (5 mg tablets most commonly available on the market) should be used with the possibility of using active folic acid metabolites, independently from the absence or presence of c.677C>T and/or c.1298A>C polymorphic variants in the MTHFR gene, if such a test has been performed.6 Evaluation of c.677C>T and c.1298A>C variants of the MTHFR gene are not justified in testing for hereditary thrombophilia.7 In patients who previously had the presence of c.677C>T and/or c.1298A>C variants in the MTHFR gene, but no clinical signs of thrombophilia were observed, anticoagulation (low‑molecular‑weight heparin or acetylsalicylic acid) should not be recommended.8 The analysis of polymorphic variants c.677C>T and c.1298A>C of the MTHFR gene for cancer predisposition should not be ordered.21
After reviewing the current recommendations of scientific societies and available literature, the experts of the Hemostasis Group of the Polish Society of Hematologists and Transfusiologists in cooperation with a national consultant in clinical genetics, Professor Maria Sąsiadek recommend the following:
1 MTHFR 677C>T and MTHFR 1298A>C gene polymorphisms should not be ordered in patients after obstetric complications, as in patients with an arterial or venous thrombotic event.
2 The management of women planning pregnancy or being pregnant who have detected MTHFR 677C>T and 1298A>C gene polymorphisms is the same as if these variants were absent.
3 First‑degree relatives of persons in whom polymorphisms of the MTHFR 677C>T and MTHFR 1298A>C polymorphisms have been detected should not be tested for carrying these mutations.
4 Genetic evaluation including, in addition to MTHFR gene polymorphism testing, identification of mutations of other genes associated with methionine metabolism should be considered to confirm or exclude homocystinuria in the presence of high tHcy, that is, above 100 md/l, in fasting plasma.
In summary, the testing for MTHFR polymorphisms should not be recommended in women after obstetric complications or in patients who have had venous or arterial thromboembolic events. Detection of these polymorphisms should not change clinical management, including indications for thromboprophylaxis. Performing such genetic tests with expenses covered from public funds by patients themselves is unnecessary and exposes patients to the inconvenience associated with blood drawing and concerns about misinterpretation of the results.
- Rozen R. Molecular genetic aspects of hyperhomocysteinemia and its relation to folic acid. Clin Invest Med. 1996; 19: 171‑178.
- Hickey SE, Curry CJ, Toriello HV. ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. 2013; 15: 153‑156. | Crossref
- Clarke R, Daly L, Robinson K, et al. Hyperhomocysteinemia: an independent risk factor for vascular disease. N Engl J Med. 1991; 324: 1149‑1155. | Crossref
- Eldibany MM, Caprini JA. Hyperhomocysteinemia and thrombosis: an overview. Arch Pathol Lab Med. 2007; 131: 872‑884.
- Klerk M, Verhoef P, Clarke R, et al. MTHFR 677C->T polymorphism and risk of coronary heart disease: a meta‑analysis. JAMA. 2002; 288: 2023‑2031. | Crossref
ARTICLE INFORMATION