Metachronous skin cancers as an indicator of a posttransplant solid tumor in a kidney recipient



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Metachronous skin cancers as an indicator of a posttransplant solid tumor in a kidney recipient
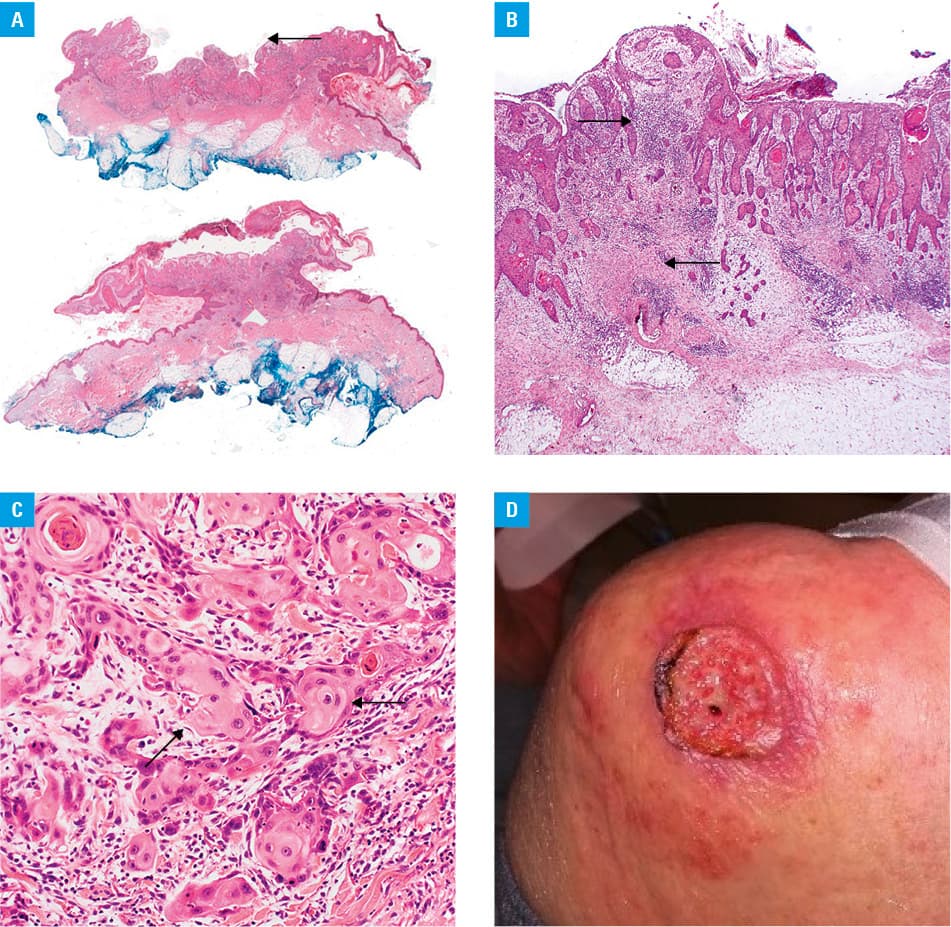
We present a case of a 66‑year‑old female smoker with terminal kidney failure since August 2014 in the course of polycystic kidney disease, 4 years after kidney transplant (May 2015), and receiving triple‑drug immunosuppression (tacrolimus + glucocorticoid + mycophenolate mofetil). Additionally, the patient had 5 metachronous skin cancers and concomitant primary pulmonary adenocarcinoma. One year after the transplant surgery, she developed a skin lesion on her right lower leg (irregular, beige‑white, of 1.5 cm in diameter), which was excised in July 2016. Histopathologic examination confirmed cutaneous squamous cell carcinoma (SCC). Other clinically overt skin lesions appeared in August 2017 (on the right forearm, 2.4 cm × 1.5 cm) and July–August 2018 (on the left elbow, Figure 1A–1D; on the right hand, 1.1 cm × 0.9 cm). All these lesions were excised with free margins, and histopathologic results confirmed basal cell carcinoma, SCC in situ, and well‑differentiated (G1) SCC. The lesions were located at sites exposed to ultraviolet radiation. In September 2018, another skin lesion developed, in the left shoulder area. The tumor grew rapidly, and in February 2019, it reached the size of 10 cm × 10 cm × 5 cm. It was surgically removed, and a histopathologic examination revealed a keratoacanthoma (Figure 1A–1D). During the follow‑up, the patient was in good general condition. As the patient was on triple immunosuppressive therapy, she was closely monitored for cancer, but no other proliferative lesions were revealed. In early April 2019, the patient developed bronchitis followed by bronchopneumonia. As there was no improvement of pneumonia, a lung computed tomography scan was performed, which revealed numerous coin lesions in both lungs. Due to the advanced stage of the process, diagnostic procedures were limited to cytology of pleural fluid and talc pleurodesis. Histopathology revealed lung adenocarcinoma with the p40(–), TTF‑1(+++) pattern. The patient died 2 weeks later due to respiratory insufficiency.
Basal cell carcinoma, cutaneous SCC, and keratoacanthoma are common nonmelanoma skin cancers. It was reported that immunosuppressive agents used after an organ transplant reduce the antitumor effect of immune cells, thus increasing the risk of skin cancer, as compared with healthy population.1 Of note, the symptom of spontaneous pain or pain on touching, which is not common in the general population, is a significant indicator of the invasive form of SCC.2,3 In our case, a primary pulmonary adenocarcinoma developed in a smoking patient 4 years posttransplant. The presence of a keratoacanthoma in transplant recipients should prompt physicians to perform cancer screening, because this tumor is associated with a higher risk of posttransplant malignancy and death.4,5
- Mittal A, Colegio OR. Skin cancers in organ transplant recipients. Am J Transplant. 2017; 17: 2509‑2530. | Crossref
- Oh CC, Hofbauer GFL, Serra AL, et al. Painful skin lesions and squamous cell carcinoma predict overall mortality risk in organ transplant recipients: a cohort study. Br J Dermatol. 2017; 176: 1179‑1186. | Crossref
- Bouwes Bavinck JN, Harwood CA, Genders RE, et al. Pain identifies squamous cell carcinoma in organ transplant recipients: the SCOPE‑ITSCC PAIN study. Am J Transplant. 2014; 14: 668‑676. | Crossref
- Marcil I, Stern RS. Risk of developing a subsequent nonmelanoma skin cancer in patients with a history of nonmelanoma skin cancer: a critical review of the literature and meta‑analysis. Arch Dermatol. 2000; 136: 1524‑1530. | Crossref
- Kang W, Sampaio MS, Huang E, Bunnapradist S. Association of pretransplant skin cancer with posttransplant malignancy, graft failure and death in kidney transplant recipients. Transplantation. 2017; 101: 1303‑1309. | Crossref
ARTICLE INFORMATION