Incidental finding of a mass in the adrenal bed following adrenalectomy due to pheochromocytoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Incidental finding of a mass in the adrenal bed following adrenalectomy due to pheochromocytoma
Adrenal incidentaloma (AI) is an asymptomatic adrenal mass detected on imaging performed for other reasons than suspected adrenal disease.1 Pheochromocytomas constitute about 3% to 7% of AIs.2 The assessment of urinary metoxycatecholamine excretion is essential in preoperative diagnostic workup and follow‑up of these tumors.3
A 67‑year‑old smoking patient with mild hypertension, glucose intolerance, and a history of myocardial infarction was diagnosed with an AI during computed tomography (CT) performed as a screening test for lung cancer (Figure 1A–1C). The heterogeneous density of the lesion raised suspicion of malignancy. The patient did not present with palpitations, sweating, headache, or anxiety. Blood levels of electrolytes, cortisol, glucose, chromogranin A, and dehydroepiandrosterone sulphate were normal. Urinary levels of metoxycatecholamines on 2 measurements were slightly elevated (metanephrine, 425 µg/24 h and 416 µg/24 h; reference range <350 µg/24 h; normetanephrine, 688 µg/24 h and 647 µg/24 h; reference range <600 µg/24 h). The patient underwent laparoscopic left adrenalectomy following premedication with doxazosin. The adrenal tumor (32 × 15 × 15 mm in size) was successfully removed. A histopathologic diagnosis was pheochromocytoma (Ki‑67 index, 2%). A follow‑up adrenal CT scan revealed a left‑sided adrenal mass (Figure 1D–1F), suggesting recurrence or incomplete tumor resection. Ten weeks following surgery, the urinary level of metoxycatecholamines measured 3 times returned to normal values (metanephrine, 41 µg/24 h, 51 µg/24 h, and 18 µg/24h; normetanephrine, 356 µg/24 h, 341 µg/24 h, and 231 µg/24 h).
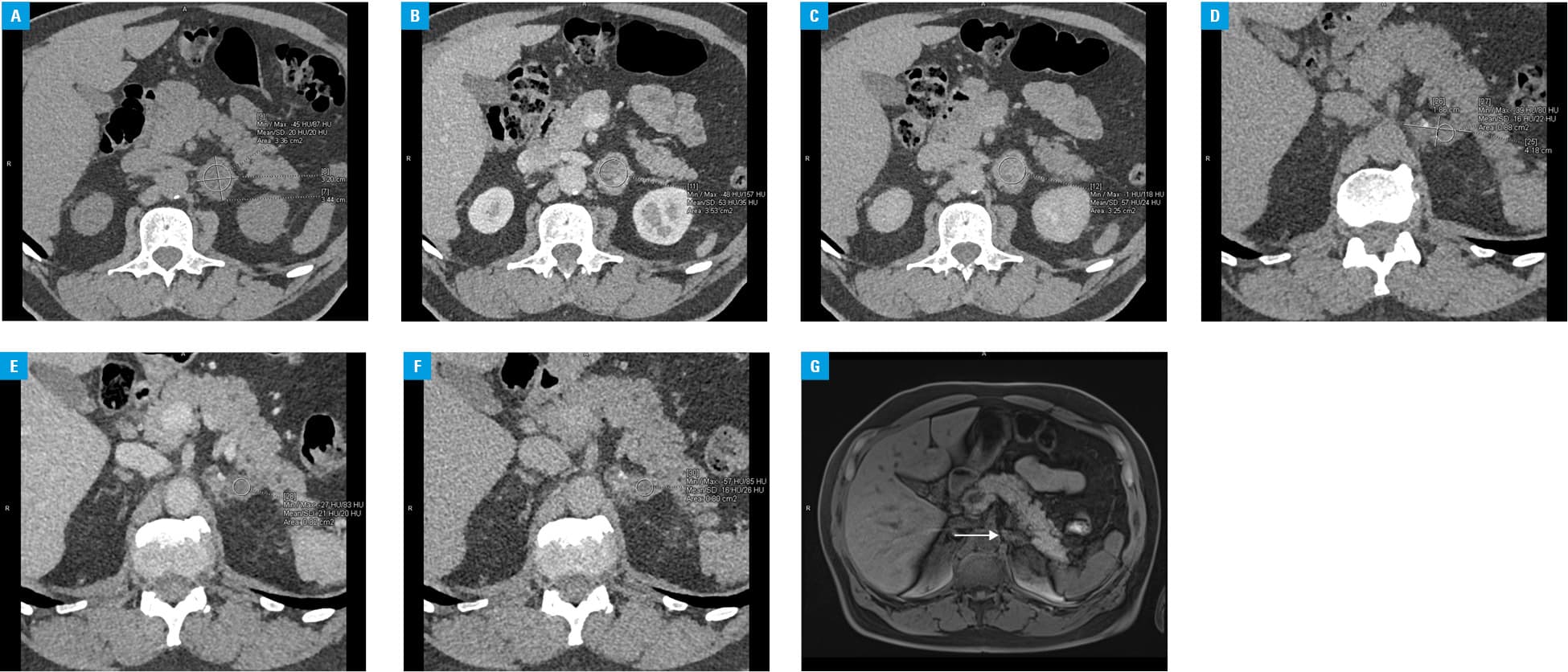
The results of control CT were surprising. The enhancement pattern after contrast media administration was different from the one before surgery. The histopathologic examination after surgery confirmed a complete resection of the adrenal mass; hence, residual tumor was unlikely. The Ki‑67 index did not suggest high malignant potential. Thus, the recurrence at 2‑month follow‑up was not probable. Due to inconsistent results of follow‑up assessment (biochemical urinalysis indicating remission and an adrenal mass on CT scan), abdominal magnetic resonance imaging was performed 4 months after surgery. It revealed that the adrenal mass was most probably an absorbable hemostatic sponge (Figure 1G). The patient was eventually diagnosed with complete remission of pheochromocytoma, and routine follow‑up at an endocrine outpatient clinic was recommended.
The material used in our patient was Spongostan (Ferrosan Medical Devices A/S, Søborg, Denmark), a hemostatic gelatin agent designed for use in surgical procedures. According to the manufacturer, it is absorbed after about 3 to 5 weeks. However, our case shows that the process may even be twice as long. The hemostatic material has already been demonstrated to mimic tumor recurrence or residual mass in the resection bed following thyroidectomy, cholecystectomy, nephrectomy, neurosurgical procedures, or gynecological surgeries.4,5 To the best of our knowledge, this is the first reported case of a patient in whom hemostatic material after adrenalectomy imitated a residual adrenal mass.
In conclusion, the presence of hemostatic material should be considered when a recurrence or an incomplete resection of an adrenal tumor is suspected by imaging soon after surgery. The awareness of such a possibility may help avoid unnecessary invasive interventions. Follow‑up imaging should be performed not earlier than 3 to 4 months after adrenalectomy to allow absorption of the hemostatic material. A different enhancement pattern after contrast media administration on follow‑up CT, along with normalization of urinary metoxycatecholamine excretion, supports the decision to delay patient evaluation for residual mass or pheochromocytoma recurrence.
- Cyrańska‑Chyrek E, Szczepanek‑Parulska E, Olejarz M, Ruchała M. Malignancy risk and hormonal activity of adrenal incidentalomas in a large cohort of patients from a single tertiary reference center. Int J Environ Res Public Health. 2019; 16. | Crossref
- Lenders JWM, Eisenhofer G. Update on modern management of pheochromocytoma and paraganglioma. Endocrinol Metab (Seoul). 2017; 32: 152‑161. | Crossref
- Lubinska M, Hoffmann M, Jendrzejewski J, et al. Successful surgical treatment of pheochromocytoma during pregnancy. Pol Arch Intern Med. 2018; 128: 322‑323.
- Heller HT, Walker BS, Sadow CA, Frates MC. Imaging appearance of topical haemostatic agents: pictorial review. Br J Radiol. 2017; 90: 20160664. | Crossref
- Learned KO, Mohan S, Hyder IZ, et al. Imaging features of a gelatin‑thrombin matrix hemostatic agent in the intracranial surgical bed: a unique space‑occupying pseudomass. AJNR Am J Neuroradiol. 2014; 35: 686‑690. | Crossref
ARTICLE INFORMATION