Redistribution of dabigatran after idarucizumab administration in a 90-year-old woman with renal failure due to persistent large intestinal bleeding



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Redistribution of dabigatran after idarucizumab administration in a 90-year-old woman with renal failure due to persistent large intestinal bleeding
A 90‑year‑old cachectic woman with hypertension, diabetes, permanent atrial fibrillation (CHA2DS2-VASc score, 6), and a history of ischemic stroke (Figure 1A), treated with dabigatran 110 mg twice a day, was admitted to the department of cardiology due to weakness and dehydration. Soon after admission, she was diagnosed with major lower gastrointestinal bleeding associated with decreasing blood pressure. Laboratory tests performed 34 hours after dabigatran intake revealed an elevated thrombin time of 234.6 seconds, activated partial thromboplastin time (aPTT) of 180 seconds, and an international normalized ratio (INR) of 21. In addition, the patient’s renal function deteriorated, with serum creatinine level of 1.5 mg/dl, glomerular filtration rate of 33 ml/min as estimated by the Modification of Diet in Renal Disease Study equation and of 19 ml/min as calculated by the Cockroft–Gault equation, and hemoglobin concentration of 12.5 g/dl. The plasma concentration of dabigatran was higher than 360 ng/ml (STA‑ECA II, Diagnostica Stago, Paris, France) and could not be quickly reduced due to poor diuresis.
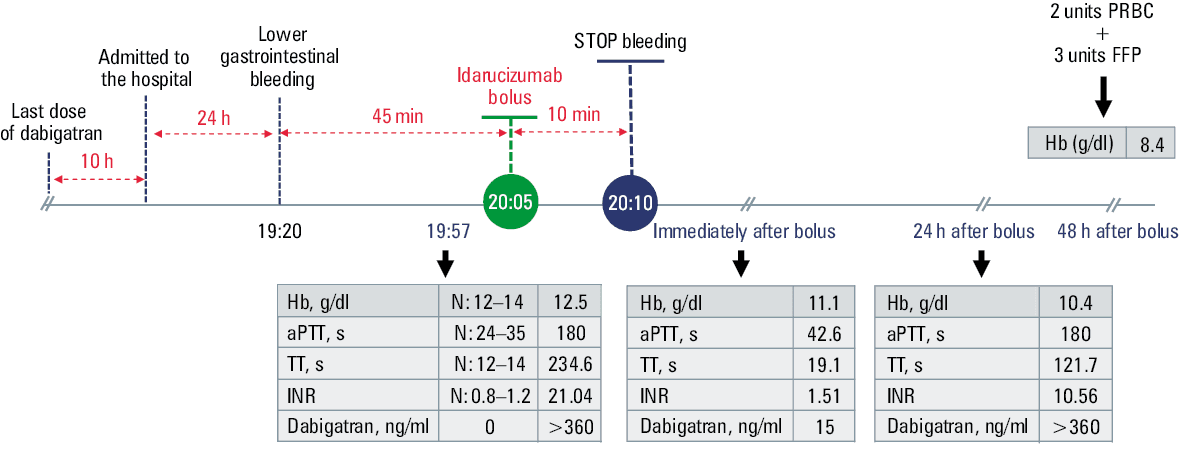
We administered an intravenous bolus injection of the reversal agent for dabigatran, namely, 5 g of idarucizumab. As a result, bleeding stopped and coagulation parameters normalized immediately, with thrombin time of 19.1 seconds, aPTT of 42.7 seconds, INR of 1.51, and plasma concentration of dabigatran of 15 ng/ml (Figure 1B).
However, on the following day, the laboratory blood clotting tests showed elevated values again, including a higher plasma concentration of dabigatran (Figure 1B). The patient presented with epistaxis and hemoptysis, but major bleeding was not observed and the patient was hemodynamically stable, with good diuresis. Sepsis complicated the in‑hospital course and the patient died on day 12.
With a history of ischemic stroke and atrial fibrillation, this patient had a very strong indication for anticoagulant treatment. However, her renal function was assessed using glomerular filtration rate estimated by the Modification of Diet in Renal Disease Study equation instead of the Cockcroft–Gault formula.1 This is very important especially in the elderly, in whom each formula can evaluate renal function differently. In this situation, dabigatran might not have been the best anticoagulant.
Idarucizumab was administered due to severe gastrointestinal bleeding. It binds free and thrombin‑bound dabigatran and immediately neutralizes its anticoagulant effects.2,3 Although the prognosis was uncertain due to the patient’s age and comorbidities, the decision to initiate idarucizumab was made unanimously. In our opinion, this was the only way to avoid post‑hemorrhagic shock.4
Our case highlights that after administration of idarucizumab, the concentration of dabigatran in the circulatory system rapidly decreases to a very low level. This creates a gradient that leads to the redistribution of dabigatran from the extravascular compartments into the vessels.1,5 If the concentration of dabigatran in the extravascular space is very high due to accumulation of the drug in the course of uncontrolled severe exacerbation of renal failure, repeated administration of idarucizumab may be necessary to further bind dabigatran.
Measuring dabigatran levels after the application of the reversal agent may be relevant in detecting the redistribution of dabigatran. Although it is possible to administer a second dose of idarucizumab, it is rarely done because a single dose is sufficient to bind up to the 99th percentile of the drug concentration as observed in the RE‑LY (Randomized Evaluation of Long‑Term Anticoagulation Therapy) trial.1,2
- Eikelboom JW, van Ryn J, Reilly P, et al. Dabigatran reversal with idarucizumab in patients with renal impairment. J Am Coll Cardiol. 2019; 74: 1760‑1768. | Crossref
- Pollack CV Jr, Reilly PA, van Ryn J, et al. Idarucizumab for dabigatran reversal – full cohort analysis. N Engl J Med. 2017; 377: 431‑441. | Crossref
- Tomaszuk‑Kazberuk A, Łopatowska P, Młodawska E, et al. Successful use of idarucizumab as a reversal agent for dabigatran in a patient with acute dissected aortic aneurysm. Pol Arch Intern Med. 2017; 127: 68‑70. | Crossref
- Pruszczyk P, Tomaszuk‑Kazberuk A, Słowik A, et al. Management of bleeding or urgent interventions in patients treated with direct oral anticoagulants: 2017 recommendations for Poland. Pol Arch Intern Med. 2017; 127: 343‑351. | Crossref
- Hegemann I, Ganter C, Widmer CC, et al. Ongoing redistribution of dabigatran necessitates repetitive application of idarucizumab. Br J Anaesth. 2018; 121: 505‑508. | Crossref
ARTICLE INFORMATION