Severe left ventricular outflow tract obstruction associated with Kounis syndrome following iodinated contrast administration



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Severe left ventricular outflow tract obstruction associated with Kounis syndrome following iodinated contrast administration
Due to chest pain of unknown origin, a 59‑year‑old woman with a history of hypertension, hyperlipidemia, and smoking underwent coronary computed tomography angiography (CCTA) following negative dobutamine stress echocardiography. The procedure went uneventful with normal sinus rhythm of 65 bpm.
Within minutes after scanning, the patient reported severe back pain and subsequently lost consciousness, with no palpable peripheral pulse and unreadable blood pressure. Chest compressions were initiated, and once the defibrillator pads were in place, sinus tachycardia was observed and the patient regained consciousness with blood pressure of 80/40 mm Hg that did not increase over the next hour despite standard treatment1 including intravenous steroids and high doses of intravenous norepinephrine. Immediately performed echocardiography revealed the small hypercontractile left ventricle without noticeable regional hypokinesis, marked systolic anterior motion of the mitral valve apparatus (SAM), severe left ventricular outflow tract (LVOT) obstruction, maximal systolic velocity of 5 m/s, which corresponded to a gradient of 100 mm Hg (Figure 1A and 1B), mitral insufficiency, and the collapsed inferior vena cava. Transient ST‑segment elevations in leads I, II, aVF, and V2 through V6 were noted on electrocardiography and a transient borderline elevated troponin level was observed (Figure 1C). Neither coronary stenoses nor signs of SAM or LVOT obstruction were found on CCTA performed minutes before the index event (Figure 1D).
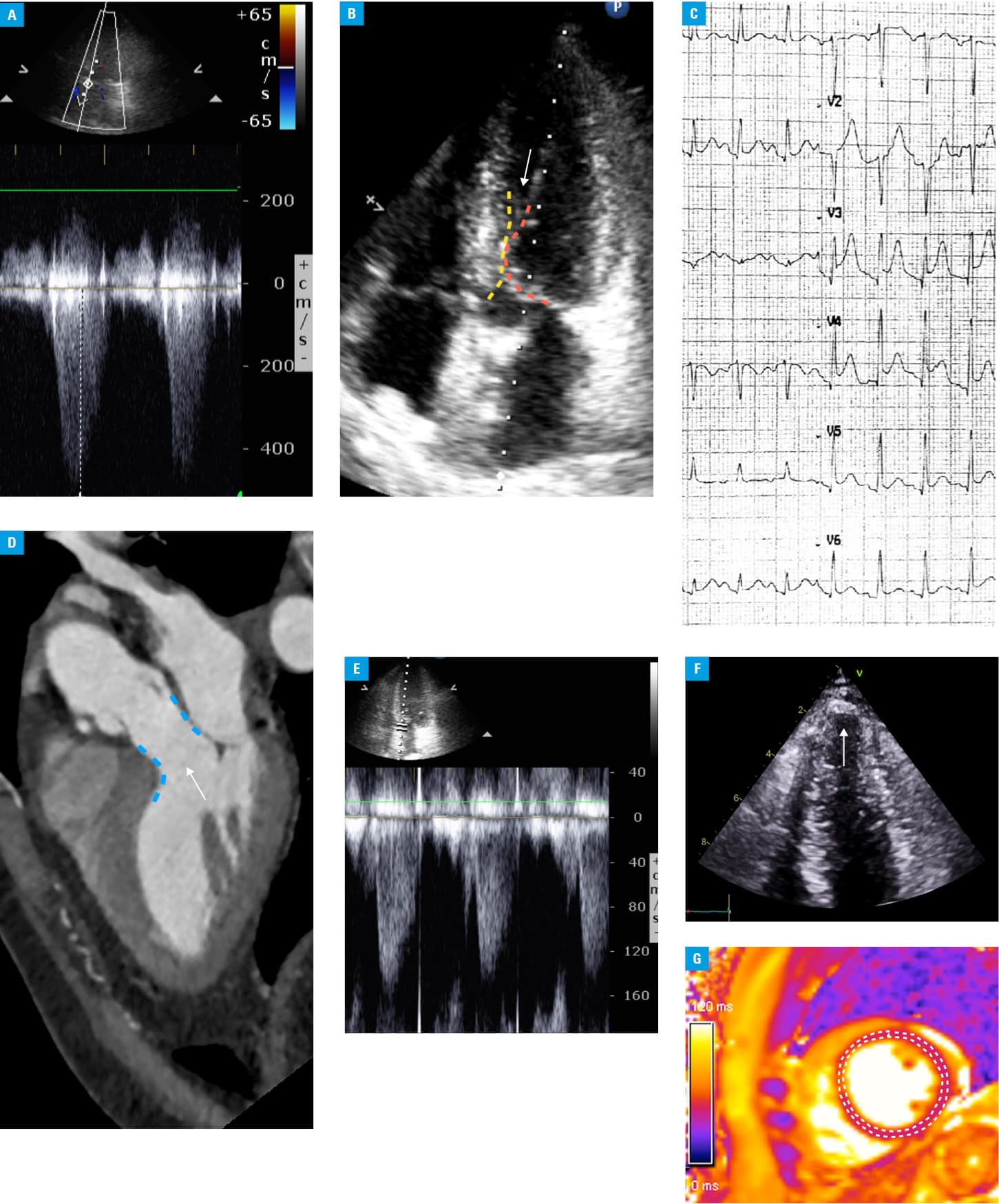
Following fluid administration, LVOT obstruction decreased to 1.6 m/s after 2 hours (Figure 1E). No further blood abnormalities were noted, except for the positive basophil degranulation test with iopromide—the contrast agent used during CCTA, which was the first examination with iodinated contrast in the patient’s medical history who had no previous allergy. Echocardiography repeated on day 3 showed slight akinesia within segment 17 (according to the American Heart Association cardiac segmentation model2), small pericardial effusion around the apex, and no LVOT obstruction (Figure 1F). These findings were still present at 1‑year follow‑up. Cardiac magnetic resonance on day 9 showed global borderline acute myocardial injury on transverse relaxation time (T2) mapping and no scar (Figure 1G).
It was concluded that this clinical presentation resulted from relative hypovolemia, rapidly reduced central venous pressure, and peripheral arterial vasodilation in response to contrast, all of which caused poor filling of the left ventricle, severe SAM, and LVOT obstruction (probably facilitated by unusually elongated papillary muscles). Coronary spasm could have also played a role (as indicated by transient ST‑segment elevation), which would imply that type 1 Kounis syndrome (ie, vasospasm caused by inflammatory mediators released during an allergic reaction to a variety of agents) might have contributed to hemodynamic collapse.2,3 Transient borderline troponin rise was most likely multifactorial in this setting.
Although type 1 Kounis syndrome following iopromide administration has been reported previously,4 this case probably represents a combination of Kounis syndrome and severe LVOTO secondary to the patient’s reaction to iodinated contrast, associated with relative hypovolemia due to prolonged fasting and the specific anatomy of papillary muscles. Lifestyle modification and a statin were recommended at discharge. One‑year follow‑up was uneventful with echocardiography findings similar to those at discharge.
- Bodzenta-Łukaszyk A, Łukaszyk M. Comment on “Calcium preparations do not inhibit allergic reactions: a randomized controlled trial”. Pol Arch Intern Med. 2017; 127: 577‑578. | Crossref
- Kounis NG. Kounis syndrome (allergic angina and allergic myocardial infarction): a natural paradigm? Int J Cardiol. 2006; 110: 7‑14. | Crossref
- Sciatti E, Vizzardi E, Cani DS, et al. Kounis syndrome, a disease to know: case report and review of the literature. Monaldi Arch Chest Dis. 2018; 88: 898. | Crossref
- Oh KY, In YN, Kwack CH, et al. Successful treatment of Kounis syndrome type I presenting as cardiac arrest with ST elevation. Chin Med J (Engl). 2016; 129: 626‑627. | Crossref
ARTICLE INFORMATION