A 50‑year‑old woman with a 15‑year history of epilepsy was admitted to our hospital due to generalized convulsive status epilepticus. The patient was initially hospitalized in the Intensive Care Unit and then in the Department of Neurology. The repeated magnetic resonance imaging of the head was normal. Extensive diagnostic workup for infectious causes revealed no abnormalities. Cerebrospinal fluid (CSF) examination showed an increased protein level and slightly elevated cytosis with lymphocyte predominance. Antinuclear antibodies (ANA) Hep‑2 were detected in serum at a titer of more than 1:2560 (speckled immunofluorescence pattern) without specificity in the immunoblot testing.
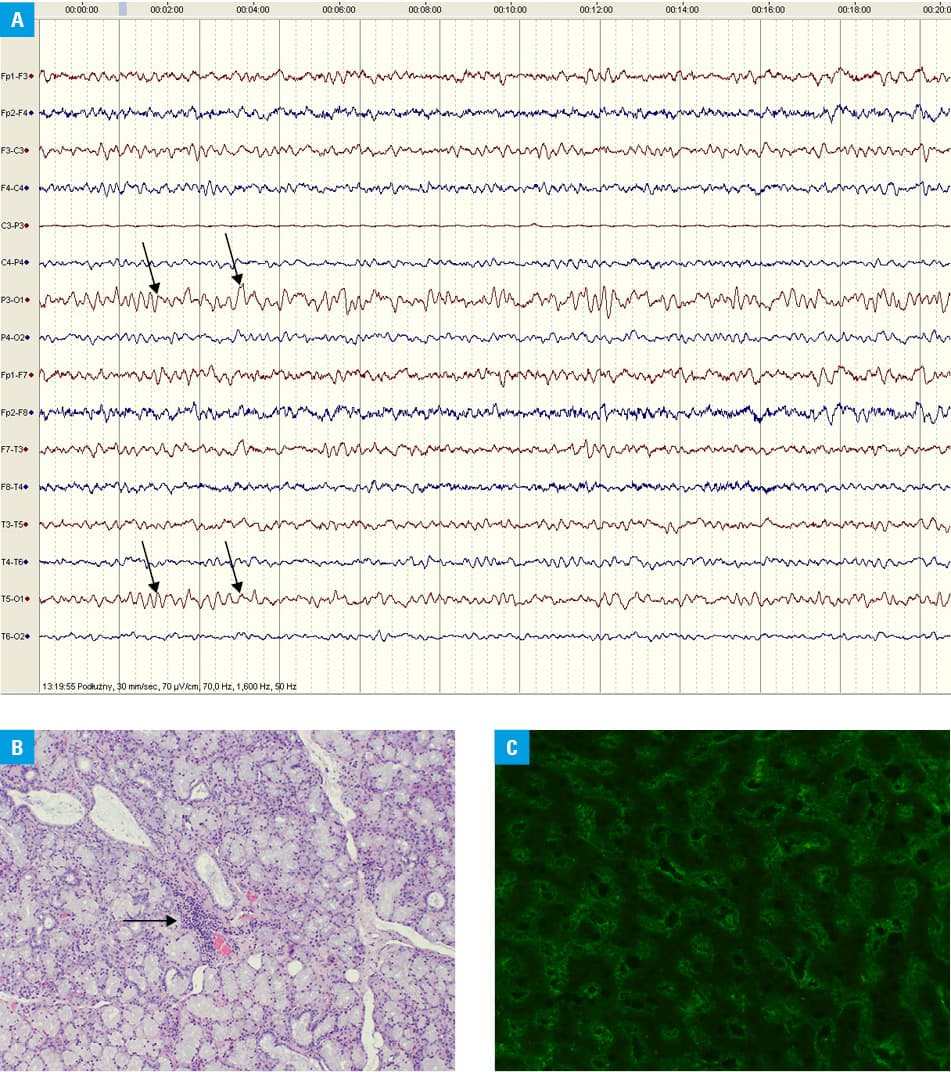
Owing to psychotic symptoms, the patient was referred to the Department of Psychiatry for further observation. Confusion, depressed mood, anxiety, as well as visual and auditory hallucinations were reported. Due to persistent epileptiform activity on electroencephalography (Figure 1A), the antiepileptic treatment was modified: lamotrigine and valproic acid were started and carbamazepine was gradually discontinued. As psychotic symptoms persisted, an antipsychotic drug (risperidone) was administered. Laboratory tests revealed reduced levels of hemoglobin (11.1 g/dl), white blood cells (2.52 G/l), neutrophils (0.81 G/l), and platelets (109 G/l). Considering the dynamics of the changes, drug‑induced toxicity seemed unlikely.
A consultation with an internist revealed a history of periodic arthralgias and muscle weakness, periodic enlargement and tenderness of the cervical and submandibular lymph nodes (not related to infection), sicca symptoms, as well as flaking skin on the hands and feet. The Schirmer test showed impaired tear secretion (right eye, 8 mm; left eye, 9 mm; reference range, >15 mm), and unstimulated whole saliva flow was significantly reduced (0.1 ml/5 min, reference range, >0.5 ml/5 min).
Based on the medical history and examination, systemic connective tissue disease was suspected. A differential diagnosis included systemic lupus erythematosus (SLE) and primary Sjögren syndrome (pSS). Both are chronic inflammatory autoimmune diseases with possible central nervous system (CNS) involvement.1,2 After histopathologic evaluation of the labial salivary glands, which showed typical lymphocytic infiltrates (Figure 1B), the patient was diagnosed with pSS (2016 American College of Rheumatology/European League Against Rheumatism criteria were fulfilled).3 Lumbar puncture was performed to assess whether neuropsychiatric symptoms might result from CNS involvement in the course of pSS. In the meantime, the patient’s condition deteriorated and limb tremor, anxiety, articulation problems, and disorientation were observed. The results of the CSF examination showed a few lymphocytes in the field of view, increased protein and albumin concentrations, oligoclonal IgG bands (type IV according to Charcot classification), and ANAs with an immunofluorescence pattern similar to that found in serum (Figure 1C).
Based on the overall clinical picture, the patient was diagnosed with CNS involvement in the course of pSS. Improvement of the general condition and complete resolution of neuropsychiatric symptoms were observed after immunosuppressive treatment with intravenous methylprednisolone pulses (5 × 500 mg), followed by oral prednisone (1 mg/kg) and intravenous cyclophosphamide infusions (15 mg/kg once a month for 6 months). This case, along with other reports,4 emphasizes the need for an interdisciplinary approach to the management of rheumatic diseases.
- Massara A, Bonanzza S, Castellino G, et al. Central nervous system involvement in Sjogren’s syndrome: unusual, but not unremarkable – clinical, serological characteristics and outcomes in a large cohort of Italian patients. Rheumatology (Oxford). 2010; 49: 1540‑1549. | Crossref
- Joseph FG, Scolding NJ. Neurolupus. Pract Neurol. 2010; 10: 4‑15. | Crossref
- Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjogren’s syndrome: a consensus and data‑driven methodology involving three international patient cohorts. Ann Rheum Dis. 2017; 76: 9‑16. | Crossref
- Wańkowicz P, Bobrowska‑Snarska D, Nowacki P, Brzosko M. Clinical manifestations of neuropsychiatric systemic lupus erythematosus in Polish patients: a single centre study from West‑Pomeranian Region of Poland. Pol Arch Intern Med. 2019 Oct 9. . | Crossref
ARTICLE INFORMATION