Kidney and inferior vena cava abnormalities with leg thrombosis syndrome mimicking retroperitoneal lymphoma in a young man



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Kidney and inferior vena cava abnormalities with leg thrombosis syndrome mimicking retroperitoneal lymphoma in a young man
A 34‑year‑old previously healthy man was referred to the hospital due to acute edema of the left leg caused by deep vein thrombosis as well as a high suspicion of lymphoma. A few weeks earlier, he started intensive physical activity for weight reduction, following which he developed gastrointestinal infection with vomiting and diarrhea leading to dehydration. Leg edema with fever occurred shortly after. Ambulatory ultrasonography and non–contrast‑enhanced computed tomography (CT) showed occlusion of the inferior vena cava (IVC) and enlarged retroperitoneal lymph nodes (Figure 1A). On admission, he was in stable clinical condition with fever (38°C) as well as left leg and lumbar pain while moving. Physical examination revealed edema and redness of the left leg with a positive Homans sign and without palpable peripheral lymph nodes. Laboratory tests showed elevated levels of C‑reactive protein (2219 nmol/l [reference range, 0.76–28.5 nmol/l]), procalcitonin (1.4 ng/l [<0.05 μg/l]), fibrinogen (9.52 g/l [1.5–4.5 g/l]), D‑dimer (7287 μg/l [<460 μg/l]), platelet count (437 × 109/l [150–350 × 109/l]), and creatinine (120 μmol/l [53–106 μmol/l]), whereas lactic dehydrogenase and coagulation factors were normal. Testicular cancer was excluded based on normal ultrasound findings. Low‑molecular‑weight heparin (enoxaparin) was continued, and antibiotic therapy (amoxicillin and clavulanic acid) was started. A CT‑guided biopsy of the enlarged retroperitoneal lymph nodes was performed. However, the histopathologic examination showed nonspecific changes, mostly blood clots. To exclude aneurysm rupture, contrast‑enhanced CT and Doppler ultrasound were performed urgently. Both tests revealed well‑developed collateral venous circulation of the abdomen and confirmed IVC occlusion. On magnetic resonance imaging (MRI) and magnetic resonance angiography (Figures 1B–1D), the infrarenal part of the IVC was occluded and the collateral vertebrolumbar vessel was shown, which were enormously developed, tortuous, partially baggy, and clotted. Moreover, thrombosis of both iliac veins, particularly on the left side, atrophic left kidney, and a dilated azygos vein were noted. Detailed blood coagulation assays, cancer screening, as well as antinuclear, antineutrophil cytoplasmic, anticardiolipin, and anti–β2-glycoprotein I antibodies were negative. On histopathology, the suspicious lymph nodes were described as a nondiagnostic damaged connective tissue. The levels of creatinine and inflammatory parameters normalized during hospitalization. A 3‑month treatment with enoxaparin and acetylsalicylic acid was recommended, along with Doppler ultrasound to evaluate the patency of the collateral venous circulation and leg veins. The patient was referred to hematology and angiology clinics for further diagnosis, treatment, and follow‑up.
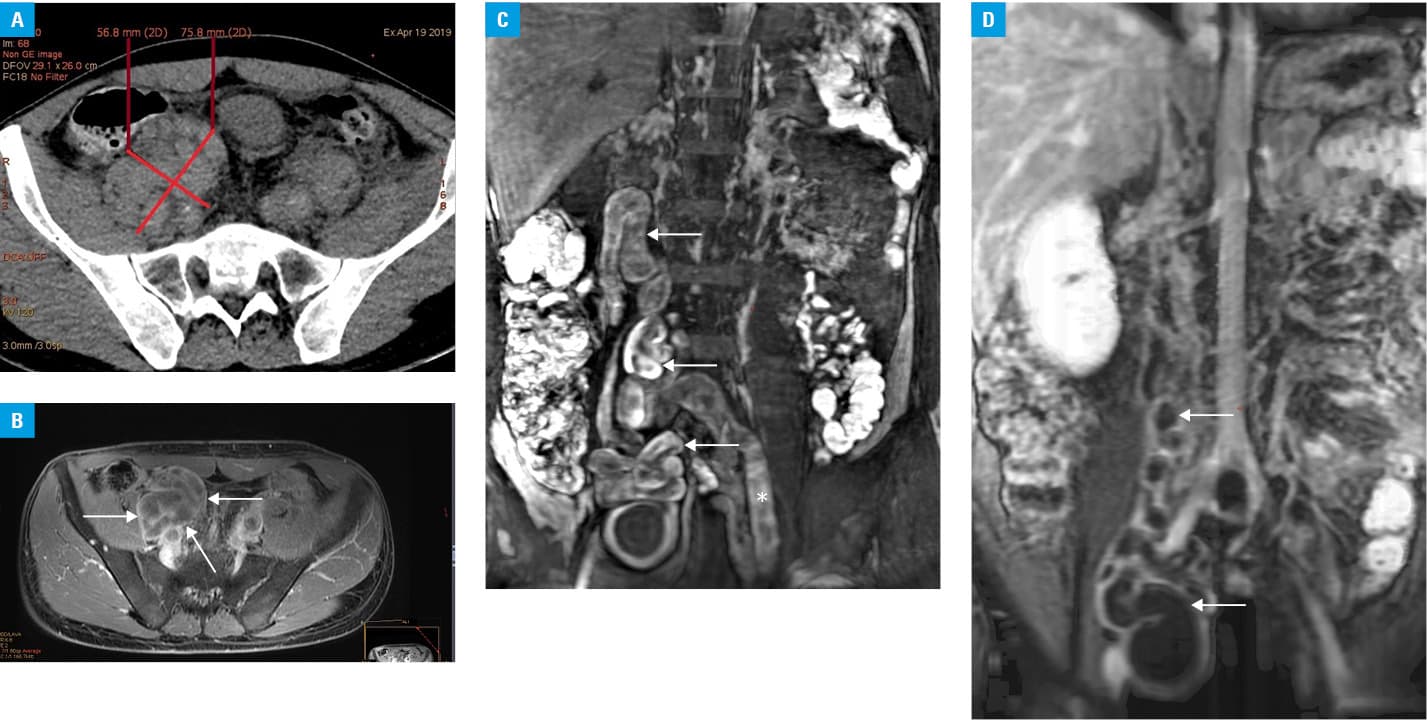
Acute deep vein thrombosis of the lower extremity in young adults is usually related to thrombophilia, immobility, trauma, surgery, or malignancy.1 Congenital occlusion of the IVC is extremely rare and is usually found during fetal development.2 Most patients are asymptomatic.3 The vertebrolumbar route is involved in 95% of cases.2 This rare congenital anomaly may mimic retroperitoneal lymphadenopathy,3,4 especially on non–contrast‑enhanced CT,5 thus contrast‑enhanced MRI is recommended.3 The association between the absence of the IVC, renal abnormalities (mainly right kidney atrophy), and leg thrombosis has been termed kidney and IVC abnormalities with leg thrombosis (KILT) syndrome.3 Additional risk factors for thrombosis such as smoking, hormonal contraceptives, or strenuous physical activity should be avoided.1 It is important to identify this entity to avoid unnecessary laparotomies and biopsies.2
- Tóth GB, Csobay‑Novák C, Berencsi A, Szeberin Z. A rare cause of ilio‑femoral deep vein thrombosis in young adults: asymptomatic chronic inferior vena cava occlusion . Orv Hetil. 2016; 157: 1361‑1365. | Crossref
- Sandercoe GD, Brooke‑Cowden GL. Developmental anomaly of the inferior vena cava. ANZ J Surg. 2003; 73: 356‑360. | Crossref
- Singh SN, Bhatt T. Inferior vena cava agenesis: a rare cause of pelvic congestion syndrome. J Clin Diagn Res. 2017; 11: TD06‑TD08. | Crossref
- Klessen C, Deutsch HJ, Karasch T, et al. Thrombosis of the deep leg and pelvic veins in congenital agenesis of the vena cava inferior . Dtsch Med Wochenschr. 1999; 124: 523‑526. | Crossref
- Regoort M, Reekers JA, Kromhout JG. An unusual cause of an inferior vena cava syndrome. Neth J Surg. 1989; 41: 92‑94.
ARTICLE INFORMATION