Isolated cardiac metastases of pulmonary carcinoid detected 13 years after resection of the primary tumor



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Isolated cardiac metastases of pulmonary carcinoid detected 13 years after resection of the primary tumor
Pulmonary neuroendocrine tumors (NETs) are a heterogeneous group of neoplasms. They can be divided into 4 categories: typical carcinoid, atypical carcinoid, and 2 high‑grade subtypes—large cell neuroendocrine cancer and small‑cell lung carcinoma.1 Pulmonary carcinoids (PCs) are rare, although their incidence has been observed to increase in recent decades. We describe a case of a woman with symptomatic isolated cardiac metastases of PC diagnosed 13 years after surgical resection of the primary tumor.
The patient was diagnosed with a tumor in the middle lobe of the right lung at the age of 44 years. In December 2004, she underwent lobectomy with lymphadenectomy. Histopathologic examination revealed pulmonary carcinoid (stage IA, T1N0M0 according to the TNM classification). She was then followed with annual chest radiography.
In May 2017, the patient presented to the emergency department with syncope. She complained of progressive dyspnea and fatigue over the past few days. Moreover, hypotension was present on admission (mean arterial pressure, 50 mm Hg). Computed tomography angiography (performed to exclude pulmonary embolism) revealed pericardial and pleural effusion with a pathological mass in the interventricular septum (Figure 1A and 1B). To confirm the diagnosis of cardiac tamponade, echocardiography was performed. It showed pericardial effusion (up to 20 mm), diastolic collapse of the right atrium, and a dilated inferior vena cava. The patient underwent pericardiocentesis to relieve symptoms. Cardiac magnetic resonance imaging (MRI) after recovery revealed 2 lesions: one in the interventricular septum (Figure 1C) and the other in the basal anterolateral segments of the heart (Figure 1D). 18F‑fluorodeoxyglucose positron emission tomography – computed tomography showed hypermetabolic areas corresponding to MRI findings, without other sites suggestive of malignancy. Pericardiotomy with biopsy confirmed typical cardiac metastases of PC (Ki67 index, 5%–10%).
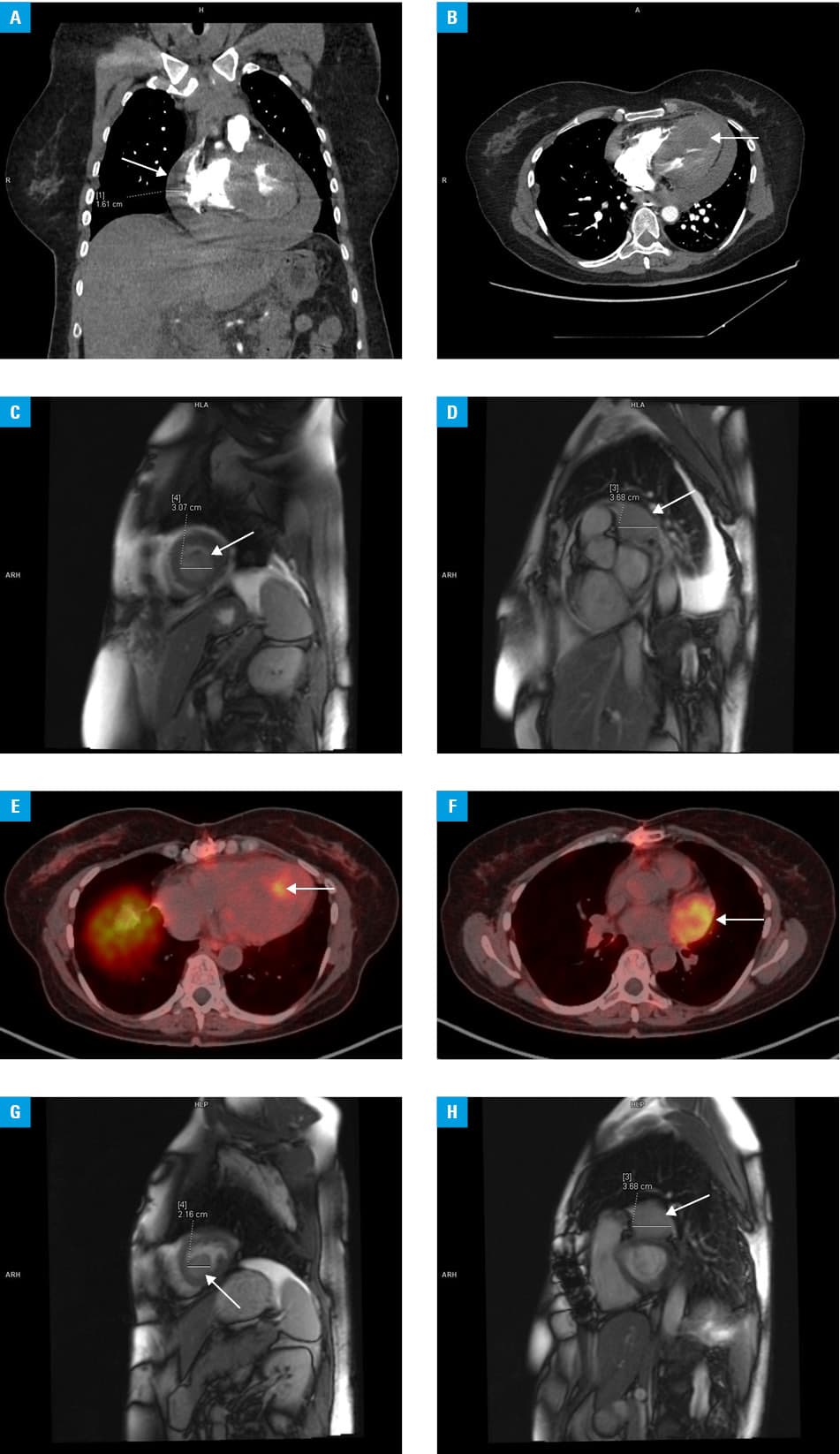
The patient was scheduled for somatostatin analogue therapy after the overexpression of somatostatin receptors in cardiac metastases had been confirmed on 68Ga‑DOTATATE positron emission tomography – computed tomography (Figure 1E and 1F). The treatment was started in September 2017. Since then, the patient has been asymptomatic. Imaging follow‑up 4 months later demonstrated good response to treatment (Figure 1G and 1H).
Pulmonary carcinoid may be asymptomatic for a long time. Symptoms may develop following local spread or metastases. An early manifestation is usually attributed to the secretion of humoral factors. Cardiac symptoms typically result from carcinoid heart disease.2 The most common sites of PC metastasis are the liver, bone, adrenal gland, and brain. To date, about 40 cases of NET metastases to the heart have been described, most of them in small‑bowel NETs.3 However, the incidence of these metastases may be underestimated, as functional imaging studies revealed the rate between 2.4% and 13%.4,5 Clinical presentation of these patients varies, from an asymptomatic course, through mild chronic symptoms (eg, arrhythmias, exertional dyspnea), to severe life‑threatening complications (acute heart failure, complete heart block, cardiac arrest, or cardiogenic shock). Metastatic lesions are usually located in the ventricles or interventricular septum.3 Cardiac metastases usually develop in patients with multiple metastatic disease.
Our report emphasizes the need for careful surveillance of patients with NETs, even many years after primary resection. Diverse imaging modalities, both morphological and functional, may be needed.
- Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015; 10: 1243‑1260.
- Bhattacharyya S, Davar J, Dreyfus G, Caplin ME. Carcinoid heart disease. Circulation. 2007; 116: 2860‑2865. | Crossref
- Jann H, Wertenbruch T, Pape U, et al. A matter of the heart: myocardial metastases in neuroendocrine tumors. Horm Metab Res. 2010; 42: 967‑976. | Crossref
- Kunz WG, Eschbach RS, Stahl R, et al. Identification and characterization of myocardial metastases in neuroendocrine tumor patients using 68Ga‑DOTATATE PET‑CT. Cancer Imaging. 2018; 18: 34. | Crossref
- Noordzij W, van Beek AP, Tio RA, et al. Myocardial metastases on 6- fluoro‑L‑DOPA PET/CT: a retrospective analysis of 116 serotonin producing neuroendocrine tumour patients. PLoS One. 2014; 9: e112278. | Crossref
ARTICLE INFORMATION