Attitudes of healthcare professionals towards the introduction of rapid response teams in Poland: a survey study after 6 months of a pilot program in 25 hospitals



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Attitudes of healthcare professionals towards the introduction of rapid response teams in Poland: a survey study after 6 months of a pilot program in 25 hospitals
Introduction
Rapid response team (RRT) systems are widely utilized around the world, particularly in high‑income countries.1 The rationale behind these systems is that early identification of deteriorating patients hospitalized outside of intensive care units (ICUs) should decrease in‑hospital morbidity and unexpected mortality. It is additionally increasingly recognized that such initiatives enhance communication, facilitate professional development, and may help improve the quality of end‑of‑life care.2,3
Rapid response teams are composed of different healthcare professionals (physicians, nurses, paramedics) and aim to bring ICU‑level skills and care outside of the ICU. Interventions delivered by the RRT may range from basic clinical assessment in a patient with shortness of breath, through administration of an antidote in patients on direct oral anticoagulants with life‑threatening bleeding, to intensive fluid resuscitation and appropriate antimicrobial therapy in previously unrecognized septic shock.4-7 Ideally, any intervention should result either in prompt management at the patient’s bedside or a timely transfer to the ICU.8 According to evidence from meta--analyses, RRTs can reduce in‑hospital mortality both in adult and pediatric populations.9
In July 2018, under the supervision of the National Center for Quality Assessment in Health Care, we launched a pilot study for a nationwide RRT implementation program in 25 hospitals (both teaching and nonteaching; 250–1500 beds each) evenly distributed around Poland.10
One of the main concerns about implementing the RRT system in Polish hospitals was an increased workload of active RRT members, as additional staffing was not feasible in most participating hospitals at the time of enrollment to the pilot study. Therefore, prior to initiation of the program, we designed a questionnaire that aimed to assess, after 6 months, the perceived change in workload and job satisfaction associated with the RRT introduction. We also asked healthcare professionals about their perception of their own safety and comfort at work and the influence of RRT implementation on patient safety. Our secondary objective was to test whether attitudes toward RRTs differed between members of the afferent and efferent limbs of the system and between physicians and nursing staff.
Methods
The program was initiated with a 3‑month period of internal staff training aimed at explaining the rationale behind RRTs, and it included a 1‑day course on the most common acute medical emergencies followed by 1‑day training in communication skills (both were conducted in each center). We trained both the interventional team (outreach, the efferent limb of the system) and hospital ward staff (the afferent limb, responsible for identifying deteriorating patients and triggering the response). In most hospitals, the outreach team consisted of ICU personnel (a physician‑led team with a nurse and residents as team members if available), but different compositions of the team were allowed to accommodate local organizational variations. Criteria of system activation in most hospitals were established based on abnormalities of critical vital parameters (changes in respiratory, circulatory, and central nervous system function). Two hospitals used the National Early Warning Score (NEWS 2) to systematically identify at‑risk patients and standardize the trigger and response system.11 In all hospitals, we encouraged activation of the system in case the staff had serious concerns about the patient’s clinical condition, even in the absence of specific objective clinical measures of clinical condition deterioration.
We distributed a self‑administered 11‑item questionnaire to healthcare professionals (nurses, clinicians, quality assessment and administrative workers) in selected hospitals from 13 voivodeships participating in the pilot RRT program. The first 5 questions concerned descriptive characteristics (geographical region, profession [physician, nurse, paramedic, quality assessment or administrative worker], primary workplace, work experience, role in the RRT), and the other 6 directly asked about individual perception of RRT introduction. The questions about attitudes towards RRTs are listed below.
Did the introduction of the RRT to the hospital:
1 Bring positive effects for the hospital?
2 Improve patient safety?
3 Accelerate interventions in at‑risk patients?
4 Improve your comfort and work safety?
5 Improve your job satisfaction?
6 Increase your workload?
The answers to each question included 5 possibilities: 1) Definitely yes; 2) Rather yes; 3) I have no opinion; 4) Rather not; and 5) Definitely not.
The questionnaire was nonpersonalized and available electronically through a dedicated link to the MetaClinician® website (www.metaclinician.com). Participation in the survey was voluntary, and no formal assessment of the response rate was performed. After the initial distribution of the questionnaire, we sent a reminder to team leaders or administrative representatives in the hospitals within 2 weeks. Answers to particular questions were analyzed for all respondents combined and within several subgroups created according to respondents’ role in the RRT (afferent or efferent limb of the system), professional affiliation (physicians vs nurses), job experience (<15 vs >15 years of professional experience), and primary workplace (emergency department [ED] or ICU vs other wards). We also analyzed results after using the 2018 Polish index of healthcare performance (Indeks Sprawności Ochrony Zdrowia) to stratify responses (3 categories based on the overall voivodeships’ rating of healthcare: 90–106 points vs 109–114 points vs 119–127 points, which corresponds to top 4 vs middle 4 vs bottom 5 voivodeships in the ranking).12
Statistical analysis
We performed all comparisons using the χ2 or Fisher exact test as appropriate for categorical variables, and the Mann–Whitney or Kruskall–Wallis test for Likert‑type questions. We used the Benjamini–Hoch- berg correction for post hoc tests. Two‑tailed P values of less than 0.05 were considered significant. All analyses were performed using R version 3.6.0 (R Project, Boston, Massachusetts, United States). No ethics approval was required for this study.
Results
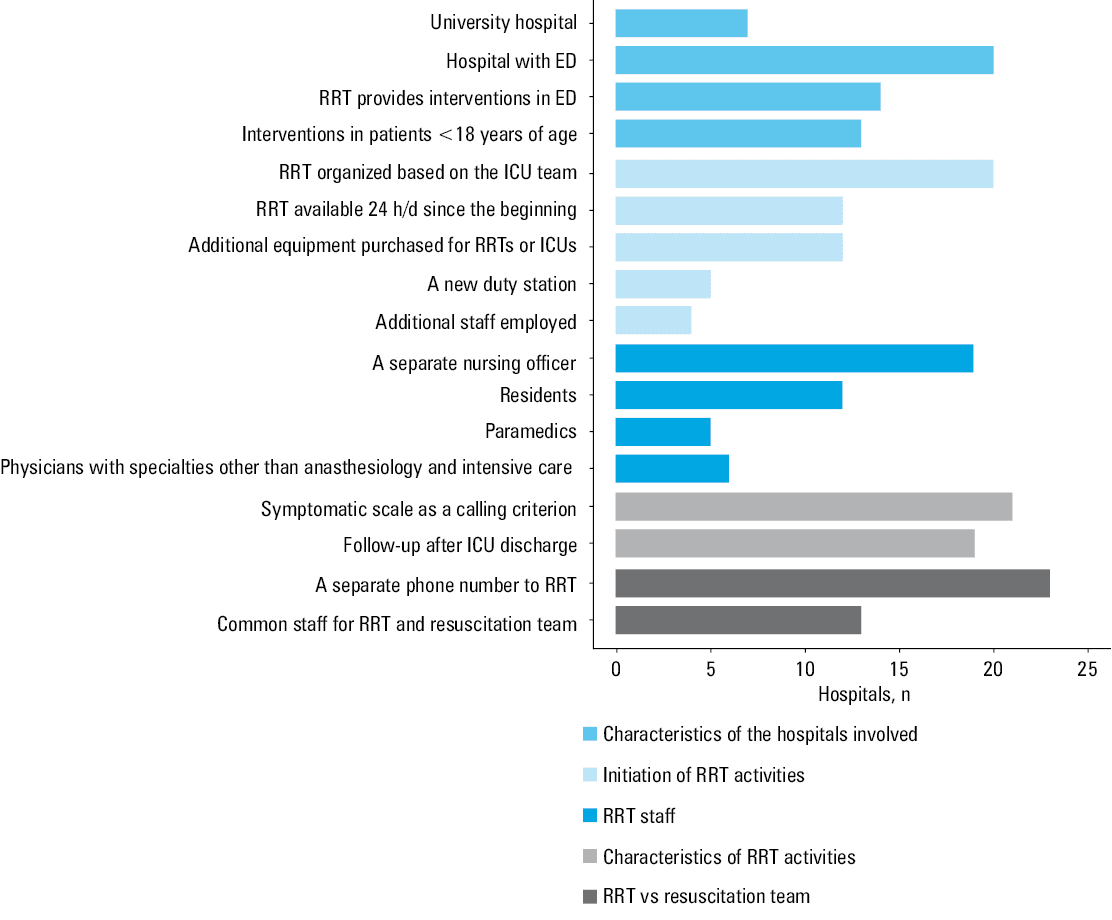
Characteristics of the RRT implementation in participating hospitals are summarized in Figure 1. Overall and stratified characteristics of surveyed participants are presented in Table 1.
- Steel AC, Reynolds SF. The growth of rapid response systems. Jt Comm J Qual Patient Saf. 2008; 34: 489‑495. | Crossref
- Lyons PG, Edelson DP, Churpek MM. Rapid response systems. Resuscitation. 2018; 128: 191‑197. | Crossref
- Salvatierra GG, Bindler RC, Daratha KB. Rapid response teams: is it time to reframe the questions of rapid response team measurement? J Nurs Scholarsh. 2016; 48: 616‑623. | Crossref
- Cieluch A, Uruska A, Falkowski B, et al. Nonadherence to potassium replacement protocol leads to prolonged management of diabetic ketoacidosis. Pol Arch Intern Med. 2018; 128: 416‑420.
- O’Byrne PM, Mejza F. Advances in the treatment of mild asthma: recent evidence. Pol Arch Intern Med. 2018; 128: 545‑549. | Crossref
ARTICLE INFORMATION