Notable effect of bromocriptine monotherapy on macroprolactinoma with self-limited cerebrospinal fluid rhinorrhea



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Notable effect of bromocriptine monotherapy on macroprolactinoma with self-limited cerebrospinal fluid rhinorrhea
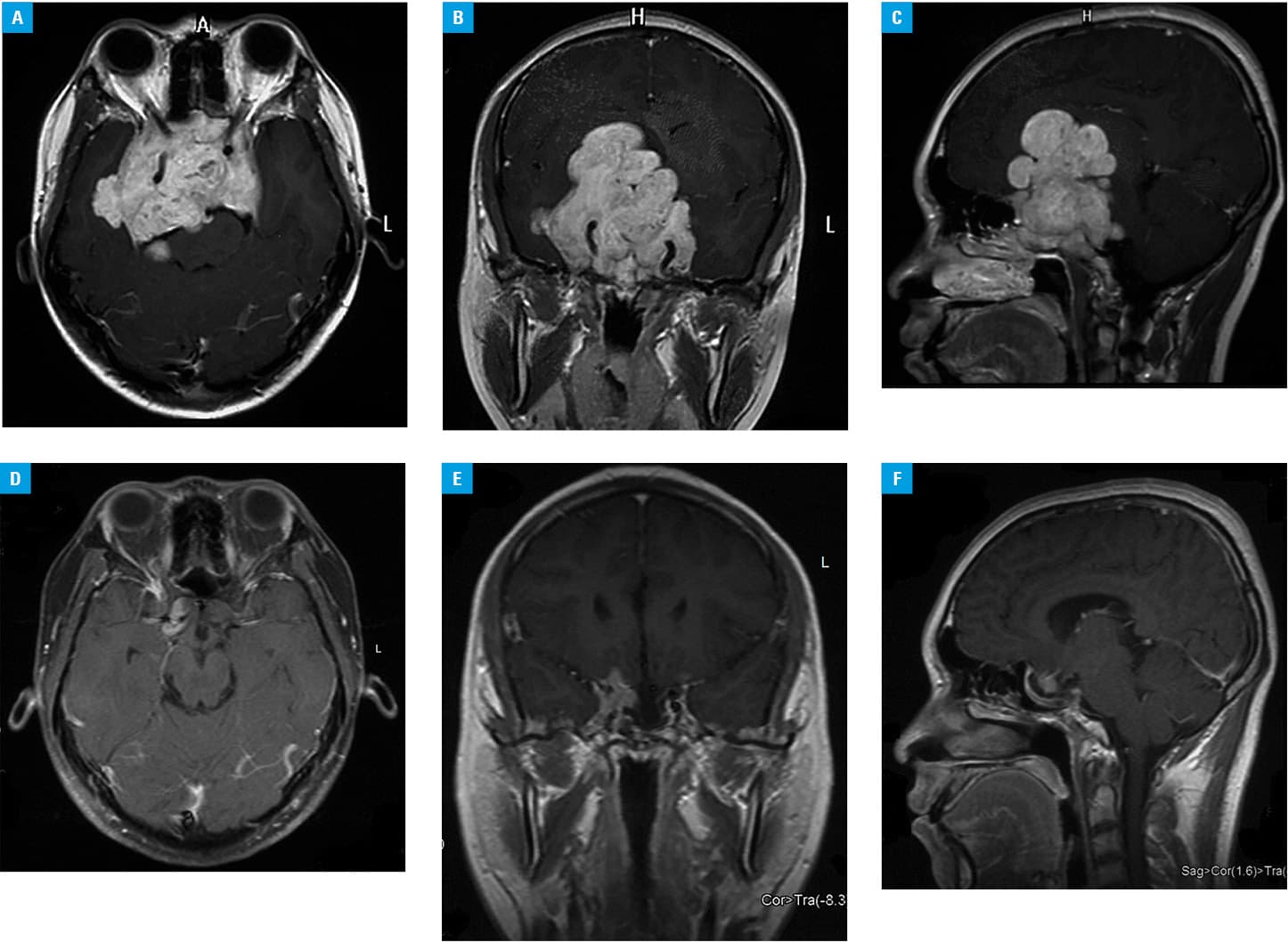
A 19‑year‑old man was admitted to an outpatient clinic because of progressive visual impairment and homonymous hemianopsia for 2 years. Cerebral magnetic resonance imaging revealed a giant mass within the sellar region (8.0 × 6.9 × 5.7 cm) (Figure 1A–1C). The serum prolactin level was initially higher than 470 ng/ml (reference range, 4.04–15.2 ng/ml). The therapy with bromocriptine was initiated at a dose of 15 mg/d. During the therapy, a significant increase in β-2‑transferrin was detected in nasal effluents, which confirmed that the patient suffered 2 episodes of unilateral (right) intermittent cerebrospinal fluid (CSF) rhinorrhea lasting about 1 month each after 1 month and 2.5 years of bromocriptine administration, respectively. After being informed of the risks, the patient still refused the repair of CSF leakage for economic reasons. Therefore, he was treated with antibiotics (oral cefdinir, 0.1 g, 3 times daily), in addition to the recommendation of bed rest and cleaning of the nasal cavities. The CSF rhinorrhea stopped spontaneously. Magnetic resonance imaging revealed that the maximum diameter of the pituitary adenoma reduced to 2.4 cm (Figure 1D–1F) after 3 years of medication. Moreover, the prolactin level normalized. The final dose of bromocriptine was 6.25 mg/d, and CSF rhinorrhea did not recur during subsequent follow‑up visits.
Prolactinomas are endocrine‑related pituitary neoplasms, accounting for 40% of all pituitary tumors,1 of which 3% to 5% are giant prolactinomas with a diameter of 4 cm or larger.2 Bromocriptine monotherapy is effective in the treatment of giant prolactinomas, including a significant reduction of tumor volume and normalization of prolactin levels.1 However, cabergoline is an excellent option for patients with bromocriptine‑resistant macroprolactinomas.3 Bromocriptine‑induced CSF rhinorrhea occurs in early medical treatment, particularly in the first few weeks. Previous studies suggested that once the diagnosis of CSF rhinorrhea is confirmed, direct surgical repair by a minimally invasive endoscopic endonasal technique is the most effective method, while other strategies include the discontinuation or reduction of dopamine agonists to allow tumors to regenerate in order to prevent leakage.4 Contrary to previous reports, 2 patients with spontaneous CSF rhinorrhea also experienced rhinorrhea subsidence with dopamine agonist treatment.5 Therefore, although the mechanism remains unclear, conservative treatment of CSF rhinorrhea should be attempted in the early stage to avoid unnecessary surgery. It is also advisable to monitor CSF rhinorrhea during treatment.
- Szczepanek‑Parulska E, Filipowicz D, Kuśmierek A, et al. Remarkable remission of an invasive giant prolactinoma under high‑dose bromocriptine monotherapy. Pol Arch Intern Med. 2017; 127: 559‑560. | Crossref
- Shimon I. Giant prolactinomas: multi‑modal approach to achieve tumor control. Endocrine. 2017; 56: 227‑228. | Crossref
- Huang HY, Zhai W, Tang H, et al. Cabergoline for the treatment of bromocriptine‑resistant invasive giant prolactinomas. Endocrine. 2018; 62: 464‑469. | Crossref
- Česák T, Poczos P, Adamkov J, et al. Medically induced CSF rhinorrhea following treatment of macroprolactinoma: case series and literature review. Pituitary. 2018; 21: 561‑570. | Crossref
- Suliman SG, Gurlek A, Byrne JV, et al. Nonsurgical cerebrospinal fluid rhinorrhea in invasive macroprolactinoma: incidence, radiological, and clinicopathological features. J Clin Endocrinol Metab. 2007; 92: 3829‑3835. | Crossref
ARTICLE INFORMATION