Successful endoscopic ultrasound–guided radiofrequency ablation of a pancreatic insulinoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Successful endoscopic ultrasound–guided radiofrequency ablation of a pancreatic insulinoma
A 40‑year‑old male patient with confirmed symptomatic insulinoma of the pancreas was referred for an endoscopic ultrasound (EUS)–guided radiofrequency ablation (RFA) of the lesion. In August 2019, the patient had an episode of agitation, behavioral disorders, and polyphagia. Blood tests revealed severe hypoglycemia, and symptoms relieved after consumption of a sweet meal. During diagnostic workup, the patient underwent abdominal magnetic resonance imaging, which revealed a focal lesion (9 mm in diameter) in the head of the pancreas. The finding was confirmed by EUS, and a tentative diagnosis of a neuroendocrine tumor was made. Subsequently, a starvation test was performed but had to be discontinued at the end of the first day due to hypoglycemia accompanied by symptoms of neuroglycopenia and high concentrations of insulin and C‑peptide. Based on the overall clinical manifestation and additional tests, a pancreatic insulinoma was confirmed.
The treatment of choice for functional pancreatic neuroendocrine tumors should be surgical resection whenever possible.1 However, surgical removal is associated with a significant risk of mortality as well as risk of pancreatic insufficiency and diabetes after surgery. The patient made an informed decision to undergo an alternative treatment, namely, EUS‑guided RFA. This decision was considered acceptable because insulinoma is benign in more than 90% of cases and very rarely presents with multiple lesions.2
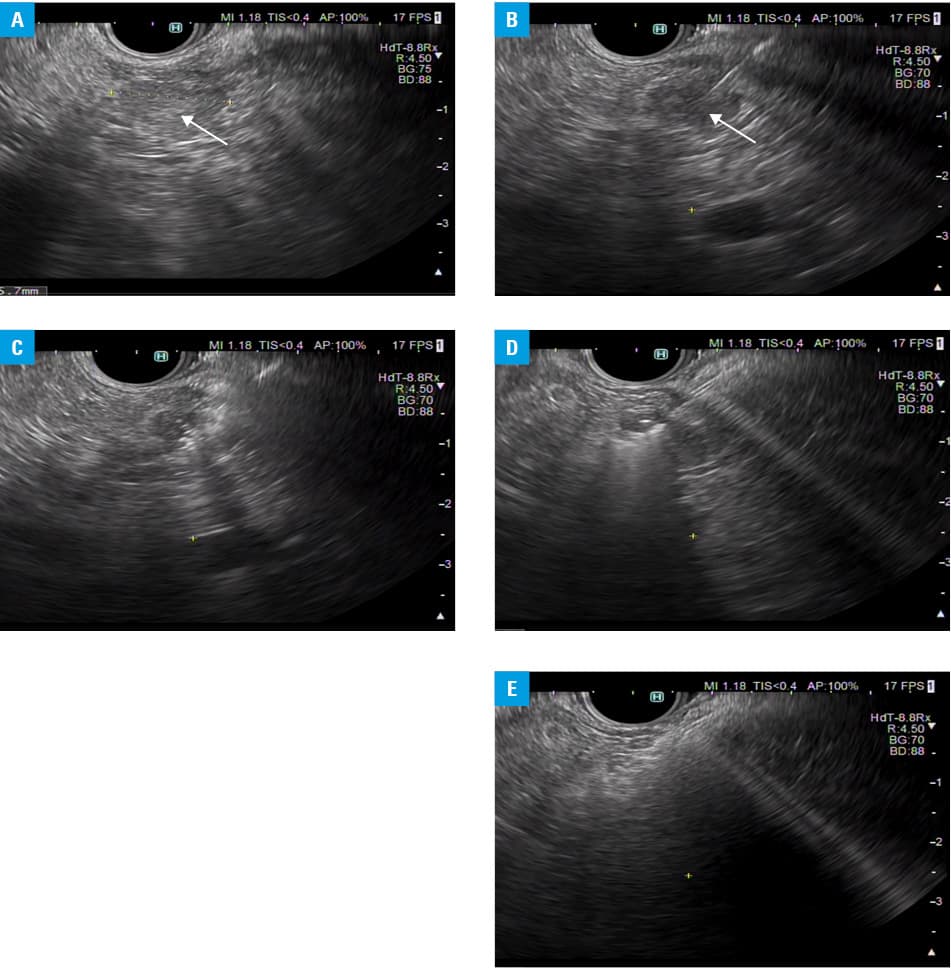
The patient was subjected to another EUS examination, which confirmed the presence of a well‑delineated, highly vascular, and hypoechoic lesion in the pancreatic head, without infiltration of the surrounding vessels (Figure 1A). Subsequently, an RFA electrode was placed directly into the lesion under EUS guidance (Figure 1B), and RFA in three 10‑second sessions with a power of 50 W was performed (Figure 1C and 1D). This resulted in the loss of vascular flow within the tumor‑feeding vessels on eFLOW Doppler ultrasound (Figure 1E). The procedure was complicated by acute necrotizing pancreatitis with a moderately severe course. However, the patient made a good recovery with conservative treatment, and his glucose levels remained within the reference range.
The RFA method has been known for a long time. This technique uses the radiofrequency current to produce thermal energy that causes tissue necrosis.3 So far, the anatomy of the pancreas and its rich vascularization have prevented the effective, targeted, and safe use of RFA. However, owing to a recent progress in therapeutic EUS, EUS‑guided RFA of pancreatic lesions has been successfully developed. The technique allows a precise delivery of antitumor treatment that combines tumor necrosis and enhancement of the immune response. In a prospective multicenter French study, 14 pancreatic neuroendocrine tumors were treated with RFA.4 Twelve lesions completely resolved (efficacy, 86%) when assessed at 1 year after procedure. Most complications are related to thermal injury to the pancreatic parenchyma and surrounding structures, including superior mesenteric vessels, bile ducts, stomach, and duodenum.5
It seems that the above technique will become a novel and much less invasive alternative to the current treatment of pancreatic neuroendocrine tumors in selected cases. However, more data are needed about its safety, long‑term effectiveness, and clinical indications.
- Buicko JL, Finnerty BM, Zhang T, et al. Insights into the biology and treatment strategies of pancreatic neuroendocrine tumors. Ann Pancreat Cancer. 2019; 2: 12. | Crossref
- Pai M, Habib N, Senturk H, Lakhtakia S, et al. Endoscopic ultrasound guided radiofrequency ablation, for pancreatic cystic neoplasms and neuroendocrine tumors. World J Gastrointest Surg. 2015; 7: 52‑59. | Crossref
- Armellini E, Crinó SF, M. Ballarè M, Occhipinti P. Endoscopic ultrasound‑guided radiofrequency ablation of a pancreatic neuroendocrine tumor. Endoscopy. 2015; 47 (suppl 1): 600‑601. | Crossref
- Barthet M, Giovannini M, Lesavre N, et al. Endoscopic ultrasound‑guided radiofrequency ablation for pancreatic neuroendocrine tumors and pancreatic cystic neoplasm: a prospective multicenter study. Endoscopy. 2019; 51: 836‑842. | Crossref
- Gaidhane M, Smith I, Ellen K, et al. Endoscopic ultrasound‑guided radiofrequency ablation (EUS‑RFA) of the pancreas on a porcine model. Gastroenterol Res Pract. 2012: 431451.
ARTICLE INFORMATION